Article Text

Abstract
Background Clinical experience with the Pipeline Embolization Device (PED) has been widely described in the literature since it obtained its European CE and FDA approvals in 2008 and 2011, respectively. The new generation of PED, the Pipeline Flex Embolization Device, received the CE mark of approval in March 2014. While the implant composition has not changed, its new delivery system has some differences. One of the main changes from the previous generation is a new delivery system that makes the device resheathable until deployed over 90% of its length. We present our preliminary experience using this device.
Methods Between May and June 2014, six patients with six aneurysms were treated with the Pipeline Flex device.
Results All devices were placed properly, without technical difficulties. We successfully resheathed and repositioned the device in two cases. Minor and major intraprocedural or periprocedural events were noted.
Conclusions The Pipeline Flex device allows more precise and controlled deployment than the current PED device. Although this preliminary experience seems positive, multicenter larger series will be needed to confirm the safety and durability of this new device.
- Aneurysm
- Blood Flow
- Flow Diverter
Statistics from Altmetric.com
Introduction
The Pipeline Embolization Device (PED) has become an important tool in the management of intracranial aneurysms. After receiving the European CE mark and FDA approval in June 2008 and 2011, respectively, clinical experience with the device has been widely described in the literature.1–5 Recently, the PUFS trial demonstrated a high rate of complete occlusion of large and giant wide-necked aneurysms arising from the internal carotid artery with a reasonably low rate of major safety events.6
The second generation of PED, the Pipeline Flex Embolization Device (PED Flex), received the CE mark in March 2014. We report our preliminary experience using this device, with an emphasis on the potential technical advantages compared with the previous device.
Methods and materials
A total of six patients with a diagnosis of intracranial aneurysm were treated with the PED Flex in three University Hospitals between May and June 2014. Clinical, procedural, and angiographic data, including aneurysm size and location, device or devices used were prospectively collected into each institution database and subsequently analyzed. Intraprocedural events were selected as the primary outcome. Differences between the premorbid and discharge modified Rankin Scale (mRS) score and neurological deficit were noted as a clinical outcome.
Aneurysm size was classified by the maximum diameter, with a mean of 11.5 mm (range 4–30 mm). All cases were unruptured. Of these, three cases were asymptomatic incidental aneurysms, two were symptomatic dissecting aneurysms and one was a recanalized previously coiled aneurysm.
The patients were premedicated with double antiplatelet therapy (100 mg aspirin and 75 mg clopidogrel) a mean of 5 days before the intervention. Platelet function test responses were within the therapeutic range in all six cases at the time of groin puncture. An initial 70–100 U/kg heparin bolus was administered and activated clotting time was maintained two times above the patient's baseline level intraoperatively. Heparin was discontinued but not reversed at the conclusion of the procedure. PED Flex devices were deployed through a Marksman microcatheter (ev3, Irvine, California, USA) using a triaxial guide catheter system in all cases. Any intraprocedural event including thromboembolic complications, dissection, aneurysm rupture, endoleak, twist or flattening of the device was immediately collected after each procedure. All procedures were performed by senior neurointerventionists with experience of more than 30 cases using the PED (MM-G, AG, JLC, EG).
During the postoperative course the neurosurgical team performed a daily neurological evaluation. Minor events were considered to be those where the deficit resolved within 7 days and major events were those where the deficit was still present after 7 days. A non-contrast head CT was performed 24 h after the embolization to evaluate for silent infarcts or intracranial hemorrhage. The mRS score was collected prior to treatment and at discharge.
Results
This series included six intracranial aneurysms located at the carotid cave, hypophyseal, cavernous, supraclinoid, paraophthalmic carotid segments and the V4 vertebral segment. Four were saccular and two were dissecting.
All devices were placed properly, without technical difficulties. The delivery technique was different from the classic technique of the previous generation PED since the new PED Flex is delivered by 80% pulling the microcatheter and 20% pushing the wire. Details of the use of the device in the six patients are shown in table 1.
Aneurysms and devices characteristics, intraprocedural details and clinical status
One device had to be resheathed because it was not deployed in the desired position, after which it was deployed successfully. In another patient, full opening of the distal end of the device was not instant, with partial expansion of the device. In this case the distal end was resheathed in order to displace the sleeves or flaps with the Marksman microcatheter in an inverted fashion. After this maneuver, the distal part of the device opened fully while unsheathing with complete wall apposition (figures 1 and 2). In all the other cases the distal part of the device opened fully during initial unsheathing. Subsequent deployment of the devices was done by pushing the delivery wire and/or unsheathing the device (figure 3).
No braid twisting or endoleak occurred during any of the procedures. In the two dissecting aneurysms there was a significant difference between the proximal and distal diameter of the parent artery. We therefore deployed two devices in order to avoid delayed migration of the devices and to obtain a more anatomic and homogeneous vessel reconstruction.

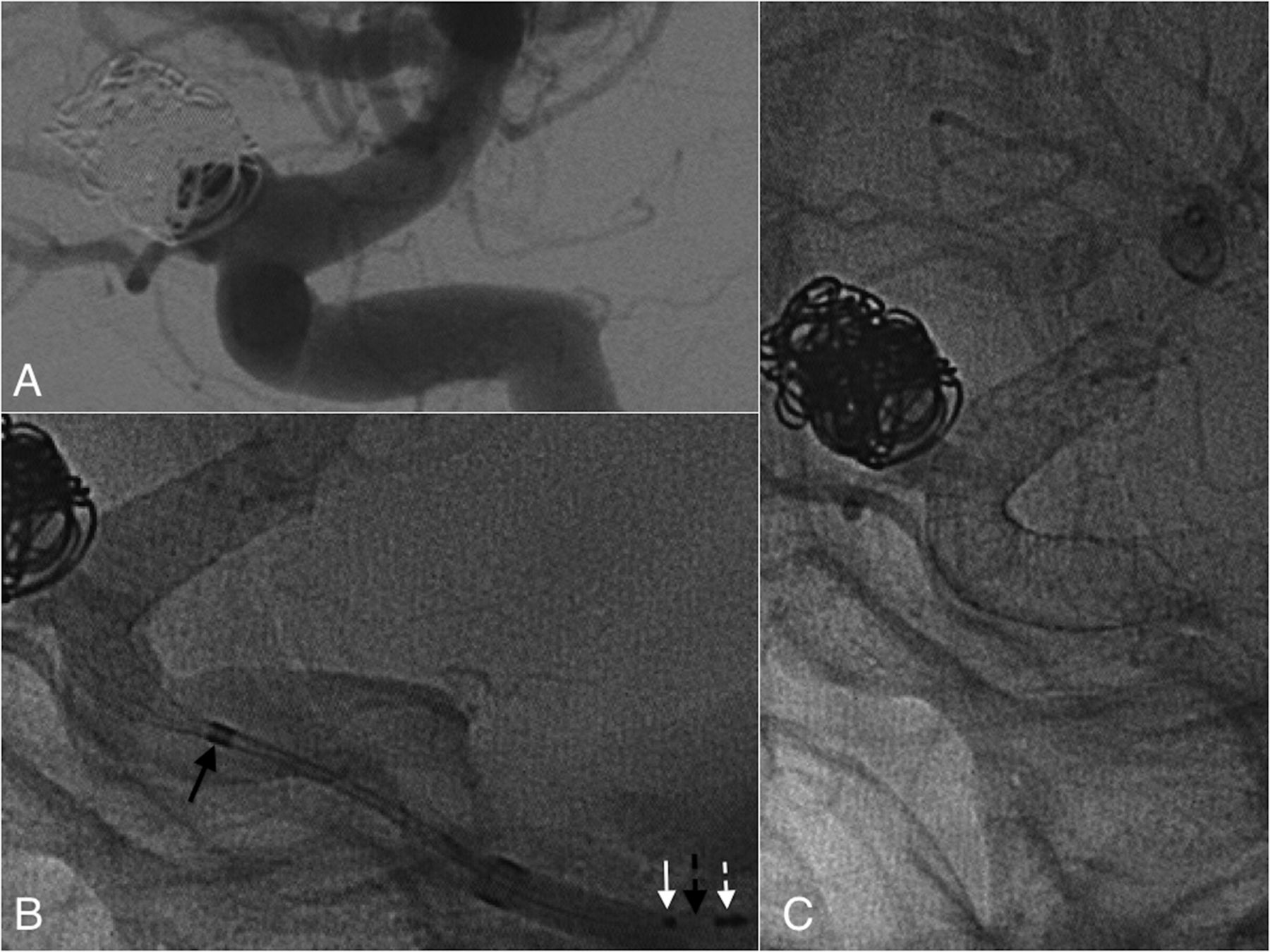
Digital subtraction angiography (DSA) oblique views and unsubtracted DSA images during deployment of the Pipeline Flex Embolization Device (PED Flex). (A) A right hypophyseal saccular aneurysm is seen. This patient also had a previous dissecting aneurysm in the ipsilateral middle cerebral artery treated with a first generation PED and a contralateral saccular aneurysm coiled 2 months earlier. (B) Initial deployment of the PED Flex showed that the braid had incomplete expansion. Note the leading wire located close to the distal end of the device, which means that one or two flaps still covered the braid. The resheathing marker (white arrow), the resheathing pad (broken arrow) and the proximal bumper (black arrow) are also noted. (C) The device was resheathed and slowly deployed again. The flaps (which are not radiopaque) were displaced in an inverted fashion and the leading wire was moved forward. The braid was then fully opened.

In vitro distal end opening test explaining the ‘inverting flaps maneuver’. (A) The implant opens instantly but sometimes the flaps (white arrows) do not open fully at the distal end of the device. (B) By resheathing the microcatheter, the flaps are displaced in an inverted fashion. (C) Unsheathing again allows full opening with perfect wall apposition.

{kind=link}
{kind=link}
{kind=link}
(A) Digital subtraction angiography views of a recanalized paraophthalmic aneurysm. (B) As with the previous generation of Pipeline Embolization Devices (PEDs), the PED Flex implant is 2–3 times longer inside the delivery microcatheter (black arrow) than the length at nominal diameter (C). The resheathing marker (white arrow), resheathing pad (broken black arrow) and proximal marker (broken white arrow) are also seen. It is crucial to understantd that the proximal bumper and resheathing pad allow the PED Flex device to be pushed out of the microcatheter when the delivery system is advanced. The resheathing pad allows the device to be resheathed back into the microcatheter.
After braid deployment, the Marksman microcatheters were tracked through the devices in order to retrieve the systems. In contrast to the current PED, no torquing was needed during retrieval because of the absence of a capture coil. Despite this, in all six cases the neurointerventionalist felt a slight resistance when the sleeves/flaps were drawn into the catheter despite doing it in a straight vessel segment with no complications.
The median length of hospital stay was 3 days. There was one postoperative event due to a 1 mm internal capsule infarct in a patient with a giant dissecting aneurysm (patient 5, table 1).
The mRS score at discharge from the hospital did not change from the admission mRS score in any but the abovementioned case.
Discussion
Clinical and technical experience with the PED has been widely described in the literature since it obtained its European CE mark in 2008.1–6 In order to overcome some of the technical challenges and to make the delivery process easier, a new generation of PED (PED Flex) received European CE mark approval in March 2014. While the implant has not changed, its new delivery system has some important differences.
One of the main differences from the previous generation is that the new delivery system makes the device resheathable until deployed over 90% of its length. The 2–3 mm protective sleeves or flaps, which are not radiopaque, protect the distal portion of the braid while the device is advanced through the microcatheter. These flaps allow instant braid release and therefore no ‘cigar-shape’ or torquing are required for the expansion of the device (figure 2). This has resulted in less foreshortening of the distal end and more precise placement.
The learning curve with the PED has been described as a predictive factor for the procedure-related complication rate.7 It is known that a decreasing complication rate could be secondary to the use of fewer PEDs because the placement of second and third devices is usually more cumbersome in the presence of previously deployed flow diverters. Also, some complications are associated with poor expansion of the device, which could lead to sacrifice of an artery8 or the need for removal by ‘corking’ or ‘pseudocorking’ techniques.9
We believe that these important challenges are more easily overcome with the new PED Flex since repositioning and resheathing allow more controlled, safe and precise deployment, lowering the number of devices per procedure. In this series we repositioned the device in one case; with the current generation PED we probably would have used a second device. Moreover, as the number of PEDs implanted influences the final cost of the procedure,10 the possibility of resheathing the PED Flex could be more cost-efficient in this setting. We have only overlapped two devices in cases of dissecting aneurysms with mismatch in arterial diameter (>1 mm) where complications such as delayed migration have been described.11 Also, by telescoping devices of different diameters, we allowed maximal device expansion, increasing metal coverage and porosity across the aneurysm neck.12 ,13
The fact that the new leading wire or tip coil is 0.012 inch and presents at 55° are also important improvements and presumably could avoid intraprocedural complications that have been described related to the leading wire of the current device.8 We have not encountered any dissection or vessel laceration in the post-embolization runs.
Finally, we experienced a slight feeling of resistance during the insertion of the flaps into the Marksman microcatheter. We therefore recommend that this baseline resistance needs to be accounted for during the initial procedures. In cases of increasing more than usual in subsequent, we would recommend to pull all the system out without drawing the flaps into the microcatheter.
We recognize that this series contains too few cases and no follow-up to draw any clinical conclusions. Our primary aim was to focus on the intraprocedural data and technical issues while collecting some basic clinical data. Although the number of cases is limited, the initial technical experience may be of use to neurointerventionalists when starting to use this device.
Conclusion
The PED Flex device allows more precise and controlled deployment than the current PED device. Although this preliminary experience seems positive, multicenter larger series will be needed to confirm the safety and durability of this new device.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors All the authors have contributed to the concept, authorship and final review of the manuscript.
Ethics approval Ethics approval was obtained from the Institutional Review Board of the Hospital Clínico Universitario de Valladolid.
Provenance and peer review Not commissioned; externally peer reviewed.