Article Text

Abstract
Introduction The Apollo system is a low profile irrigation–aspiration system which can be used for the evacuation of intracranial hemorrhage. We demonstrate the feasibility of using Apollo to evacuate intracranial hemorrhage in a series of three patients with combined neuronavigation, neuroendoscopy, and cone beam CT (CB-CT).
Methods Access to the hematoma was planned using neuronavigation software. Parietal (n=2) or frontal (1) burr holes were created and a 19 F endoscopic sheath was placed under neuronavigation guidance into the distal aspect of the hematoma along its longest accessible axis. The 2.6 mm Apollo wand was then directed through the working channel of a neuroendoscope and used to aspirate the blood products under direct visualization, working from distal to proximal. After a pass through the hematoma, the sheath, neuroendoscope, and Apollo system were removed. CB-CT was then used to evaluate for residual hematoma. When required, the CB-CT data could then be directly uploaded into the neuronavigation system and a new trajectory planned to approach the residual hematoma.
Results Three patients with parenchymal (n=2) and mixed parenchymal–intraventricular (n=1) hematomas underwent minimally invasive evacuation with the Apollo system. The isolated parenchymal hematomas measured 93.4 and 15.6 mL and were reduced to 11.2 (two passes) and 0.9 mL (single pass), respectively. The entire parenchymal component of the mixed hemorrhage was evacuated, as was the intraventricular component within the right frontal horn (single pass). No complications were experienced. All patients showed clinical improvement after the procedure. The average presenting National Institutes of Health Stroke Scale was 19.0, which had improved to 5.7 within an average of 4.7 days after the procedure.
Conclusions The Apollo system can be used within the neuroangiography suite for the minimally invasive evacuation of intracranial hemorrhage using simultaneous neuronavigation for planning and intraprocedural guidance, direct visualization with neuroendoscopy, and real time monitoring of progress with CB-CT.
- Hemorrhage
- Technique
- Technology
- Navigation
- Endoscopy
Statistics from Altmetric.com
Introduction
The Apollo system is a novel endoscopically guided irrigation–aspiration system recently cleared by the US Food and Drug Administration for tissue and fluid removal during surgery of the ventricular system. The device can also be used to evacuate intracranial hemorrhages.1
We describe a technique for the application of this device to evacuate intracranial hemorrhages in a series of patients using combined neuronavigation, direct visualization with neuroendoscopy, and real time monitoring of progress with cone beam CT (CB-CT) in the neuroangiography suite.
Methods
Patients
A series of three patients underwent minimally invasive evacuation of intracranial hematomas with the Apollo system. Clinical and imaging data were compiled and reviewed. Our institutional review board approved the assembly of this case series.
Apollo device description
The Apollo system is an aspiration–irrigation system, which can be attached via flexible tubing to the Apollo wand (2.1 and 2.6 mm diameter sizes). The wand houses an internal agitator element that, when actuated with a foot pedal, macerates clot material to maintain the patency of the system during aspiration. The main unit houses an adjustable vacuum pump for aspiration, a peristaltic pump for saline irrigation, and transmits vibrational energy to the internal agitator element within the wand. The internal agitator element is entirely housed within the wand lumen, and the vibrational energy does not exit the system. The device is designed to allow the evacuation of blood products through a minimally invasive access without clogging. Both sized wands fit through the working channels of commercially available neuroendoscopes (Lotta, Karl Storz, Tuttlington, Germany).
Apollo procedure
MR (n=1) or CT (n=2) imaging studies were uploaded into the neuronavigation software (iPlan Net; Brainlab, Feldkerchin Germany) for procedural planning and guidance. A trajectory was selected that was both technically feasible and allowed access to the longest possible axis of the hematoma. Patients were initially placed supine on the neuroangiography table, a sterile field was prepared, and an external array (Skull Reference Base with Skull Reference Array with Reflective Marker Spheres; Brianlab) was placed for registration. Patients were placed in a head lateral (n=2) or flexed (n=1) position, and a second sterile field was prepared over the region of the access. Fiducial markers were placed around the circumference of the targeted cranial access site (for later re-registration to updated CB-CT imaging, if necessary). A 14 mm perforator (Codman, Raynham, Massachusetts, USA) was used to create a burr hole. An array (Instrument Adapter Clamp with Instrument Adapter Array; Brainlab) was attached to a 19 F peel away sheath (Aesculap Inc, Center Valley, Pennsylvania, USA) which was registered to the navigation system. The sheath was then advanced using neuronavigation into the targeted landing zone within the distal aspect of the hematoma. The sheath was stabilized and the inner obturator was then removed and the liquefied component of the hematoma allowed to passively drain. The neuroendoscope (Lotta) was then inserted into the sheath, and under direct visualization the Apollo 2.6 mm wand was placed through the working channel of the endoscope.
Initially, and throughout the majority of the case, both the Apollo wand and endoscope were maintained within the sheath. The sheath was irrigated using the irrigation port of the endoscope, and the irrigant was intermittently aspirated with the Apollo system until a clear working view was created within the sheath that allowed visualization of the surgical field at the sheath tip. When organized hematoma was visualized at the tip of the sheath, the Apollo wand was advanced under direct visualization to, or just beyond, the tip of the sheath and actuated to evacuate the blood products. When the working view became obscured, additional irrigation and aspiration was performed intermittently to clear the field. When all blood products were cleared from the working field, the sheath was retracted slightly and the procedure was repeated. The position of the sheath was typically monitored directly using the neuronavigation system (two cases) or approximated (one case, in which the neuroendoscopic trocar, rather than the sheath, was registered to the navigation system). This technique was used until the sheath had been withdrawn through the entire long axis of the hematoma. At that point, the sheath, neuroendoscopic trocar, and Apollo wand were removed. CB-CT (dynaCT; Siemens, Medical Imaging, Erlangen, Germany) was then performed. The CB-CT data were postprocessed on a workstation (Leonardo; Siemens Medical Imaging, Erlangen, Germany) and either uploaded to the neuronavigation system for guidance of a second pass (one case) or used as a control CT to confirm adequate hematoma evacuation and assess for any complications (ie, rebleeding).
Hematoma volumes were measured using a standard a×b×c/2 calculation on preoperative and postoperative imaging.
Results
Three patients (one man, mean age 61.8 years) with parenchymal (n=2) and mixed parenchymal–intraventricular (n=1) hematomas underwent minimally invasive evacuation with the Apollo system. The isolated parenchymal hematomas measured 93.4 mL and 15.6 mL and were reduced to 11.2 mL (two passes) and 0.9 mL (single pass), respectively. The entire parenchymal component of the mixed hemorrhage was evacuated, as was the intraventricular component within the right frontal horn (single pass). No complications were experienced. The average presenting National Institutes of Health Stroke Scale (NIHSS) was 19.0, which improved to 5.7 within an average of 4.7 days after the procedure.
Case No 1
A 79-year-old man with hypertension, diabetes, hyperlipidemia, and coronary artery disease on aspirin presented with left hemiplegia, left neglect, and left hemianopsia. NIHSS on presentation was 18 (figure 1). CT showed a large lobar hemorrhage involving the right parietal, temporal, and occipital lobes, with surrounding edema and local mass effect on the right lateral ventricular system. The patient was unable to accept blood products based on his religious beliefs. MRI with contrast showed no enhancement or mass lesion. CT angiography and subsequent catheter angiography showed no vascular lesion to account for the hemorrhage. Serial aspirin response units (ARU; Accumetrics Inc, San Diego, California, USA) were measured, and on post-bleed day (PBD) 4 had increased to 536.

A 79-year-old man with a large right lobar hypertensive hemorrhage. FLAIR sequences in the sagittal (A) and axial (B–D) planes demonstrate a 93.4 mL hematoma distributed within the temporal, parietal, and occipital lobes with surrounding edema. Mass effect results in near complete effacement of the ipsilateral lateral ventricle and right to left subfalcine herniation. Following evacuation with the Apollo system (two passes), sagittal (E) and axial (F–H) reconstructions at the same level show a marked reduction in the volume of the hemorrhage (to 11.2 mL) with resolution of the local mass effect and midline shift. The case was performed in the angiography suite with neuronavigation and direct visualization with endoscopy. The 19 F endoscopic sheath was registered with an attached array (I, arrow) and stabilized at the insertion site. The endoscopic trocar was placed through the sheath (I, double arrow). Fiducial markers were placed around the burr hole to facilitate re-registration to the updated dynaCT dataset(s). During the case, one operator stabilized and, when necessary, manipulated the sheath, another operated the neuroendoscope, and another operated the Apollo wand while observing the neuroendoscopic and neuronavigation monitors (J).
On PBD 4, hematoma evacuation was performed with the Apollo system. The procedure was performed through a right parietal approach. A total of two passes with the Apollo wand–endoscopic sheath were required to achieve adequate hematoma reduction. After the initial pass, dynaCT data were directly uploaded to the neuronavigation software and used to guide replacement of the endoscopic sheath and the second pass with the Apollo wand. The Apollo wand was actuated for a total of 3 min and 40 s during the case.
No complications were encountered. The patient emerged from anesthesia at preprocedural baseline and demonstrated daily clinical improvement thereafter. On postoperative day 6, his NIHSS score had improved to 7.
Case No 2
A 56-year-old woman with a past medical history of colitis presented with the abrupt onset of right hemiparesis, aphasia, and right hemianesthesia (figure 2). Blood pressure was 180/97 mmHg on admission. NIHSS score on presentation was 17. CT and subsequent MR with contrast demonstrated a left basal ganglia hemorrhage with a circumferential region of surrounding edema with a component of restricted diffusion superiorly. Subsequent CT angiography and catheter angiography demonstrated no vascular lesion to account for the hemorrhage.
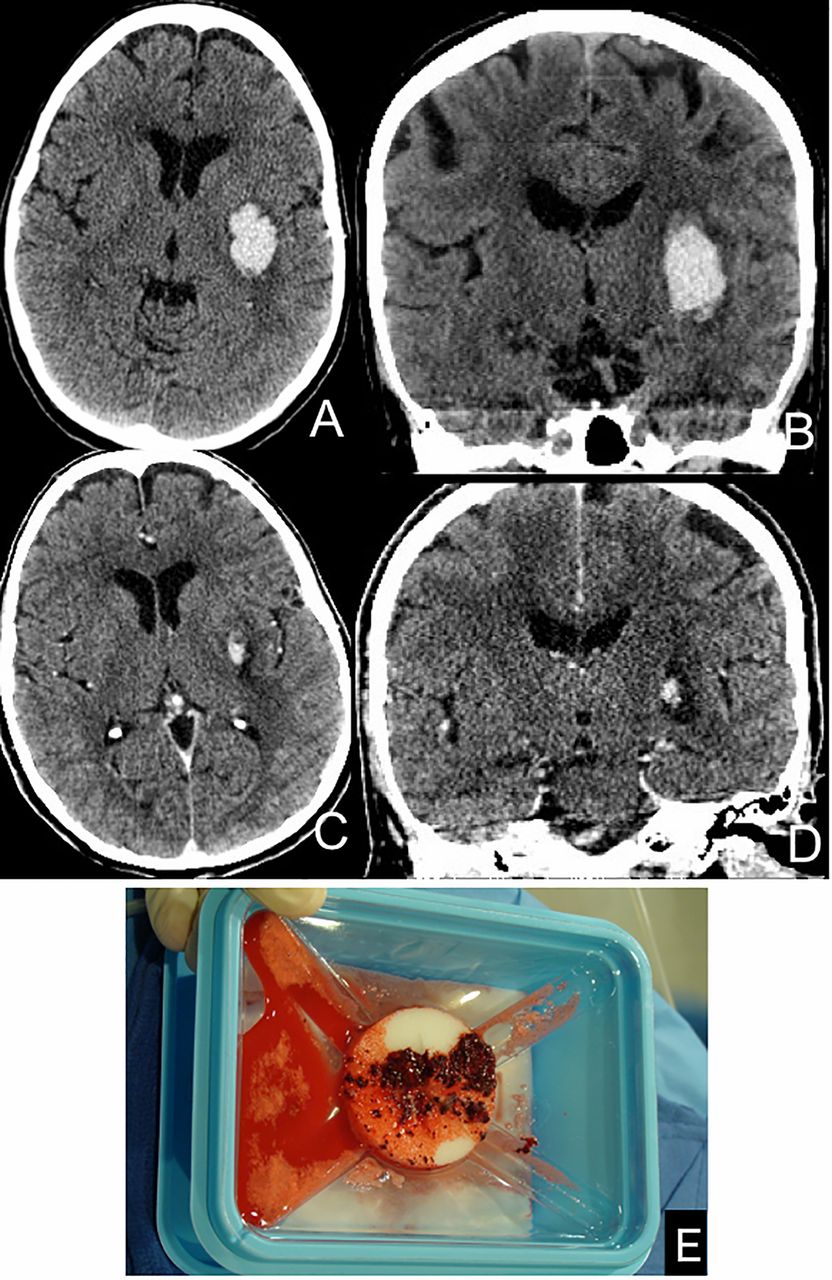
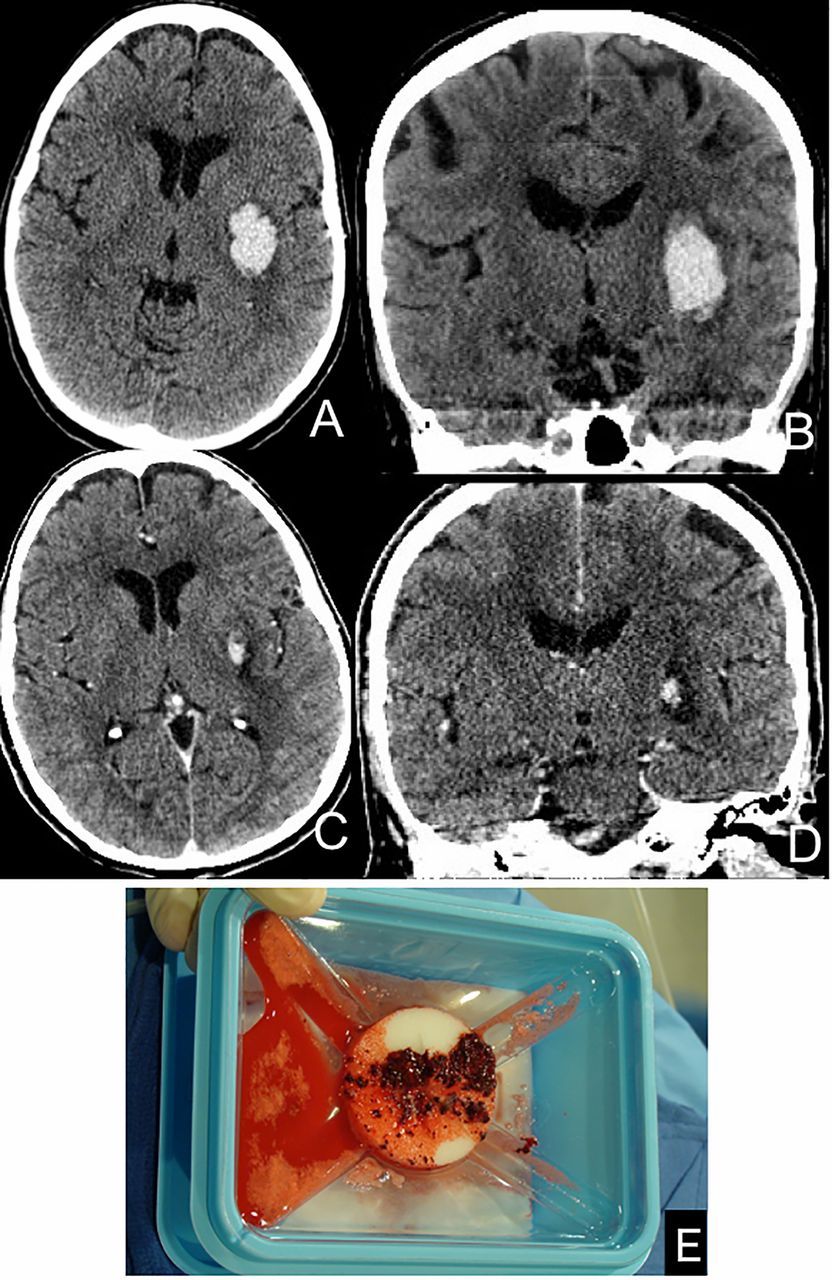
A 56-year-old woman with a left basal ganglia hemorrhage. Axial (A) and coronal (B) CT images demonstrate a 15.6 mL left basal ganglia hematoma. Following evacuation with the Apollo system (one pass), CT images at the same anatomical locations (C, D) demonstrate a marked reduction in the volume of the hematoma to 0.9 mL with collapse of the hematoma cavity. The contents of the Apollo collection canister (E) were filtered, demonstrating a mixture of liquefied blood products and numerous small clot fragments, which had been morsealized within the Apollo wand during actuation.
On PBD 2, she underwent hematoma evacuation with the Apollo system. Adequate hematoma reduction was achieved with a single pass. The Apollo system was actuated for a total of 1 min and 11 s. No complications were encountered. The patient emerged from anesthesia with some improvement in both speech and right-sided strength. Her clinical improvement continued, and on postoperative day 4 her NIHSS score had improved to 4.
Case 3
A 43-year-old woman presented with sudden onset of severe headache, which progressed quickly to coma (figure 3). CT study demonstrated a right caudate head parenchymal hemorrhage with a large intraventricular component, casting the right lateral ventricle, third and fourth ventricles, with associated hydrocephalus. On transfer to our institution, her pupils were fixed and dilated and she was sedated and paralyzed. She was taken directly to the angiography suite and bilateral external ventricular drains were placed with angioCT guidance (iGuide; Siemens Medical Imaging).2 Opening pressure was 47 mm Hg, which declined to 10 mm Hg after the ventriculostomies. Conventional angiography showed slow intracranial flow and no vascular etiology for the hemorrhage.
{kind=link}
{kind=link}
{kind=link}
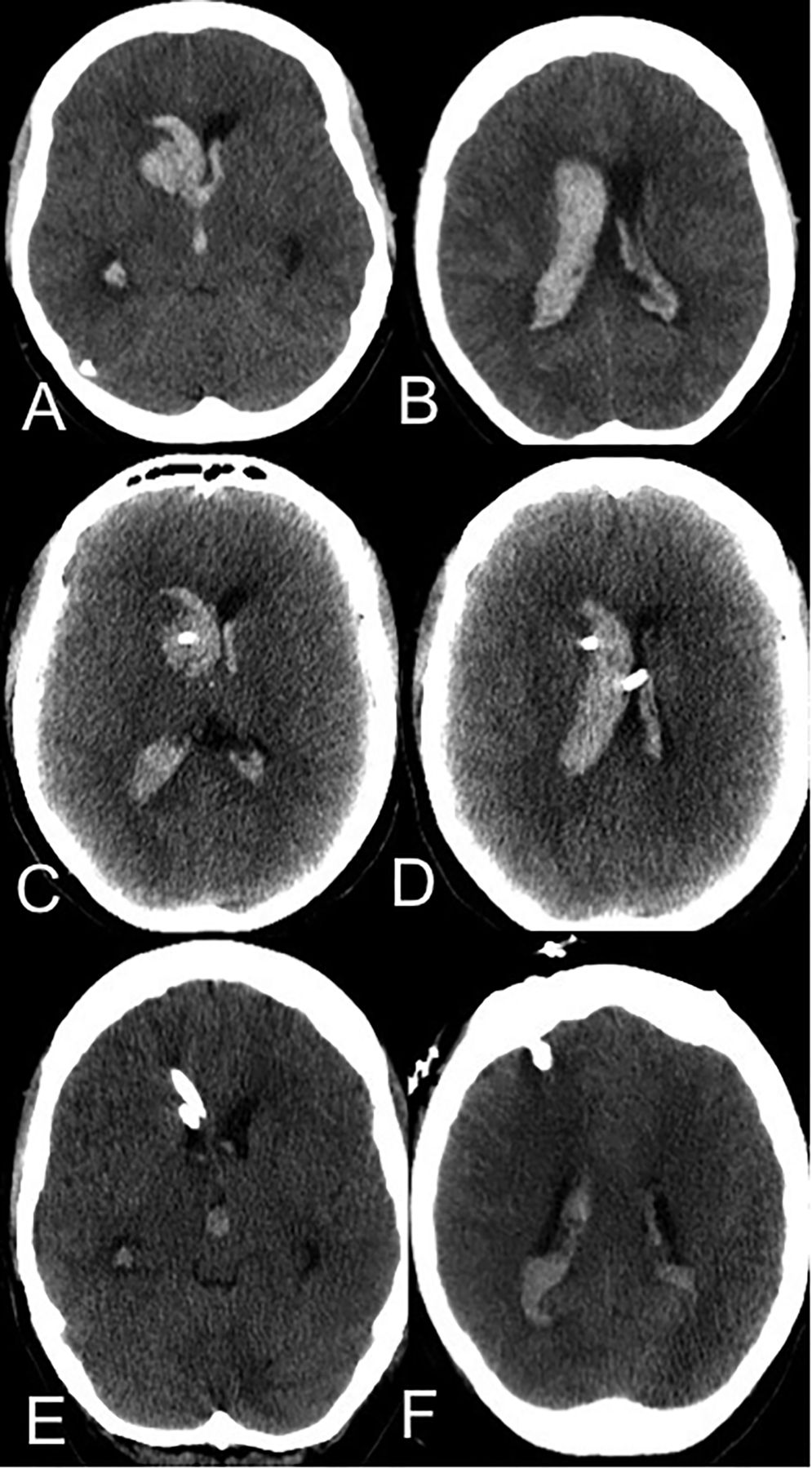
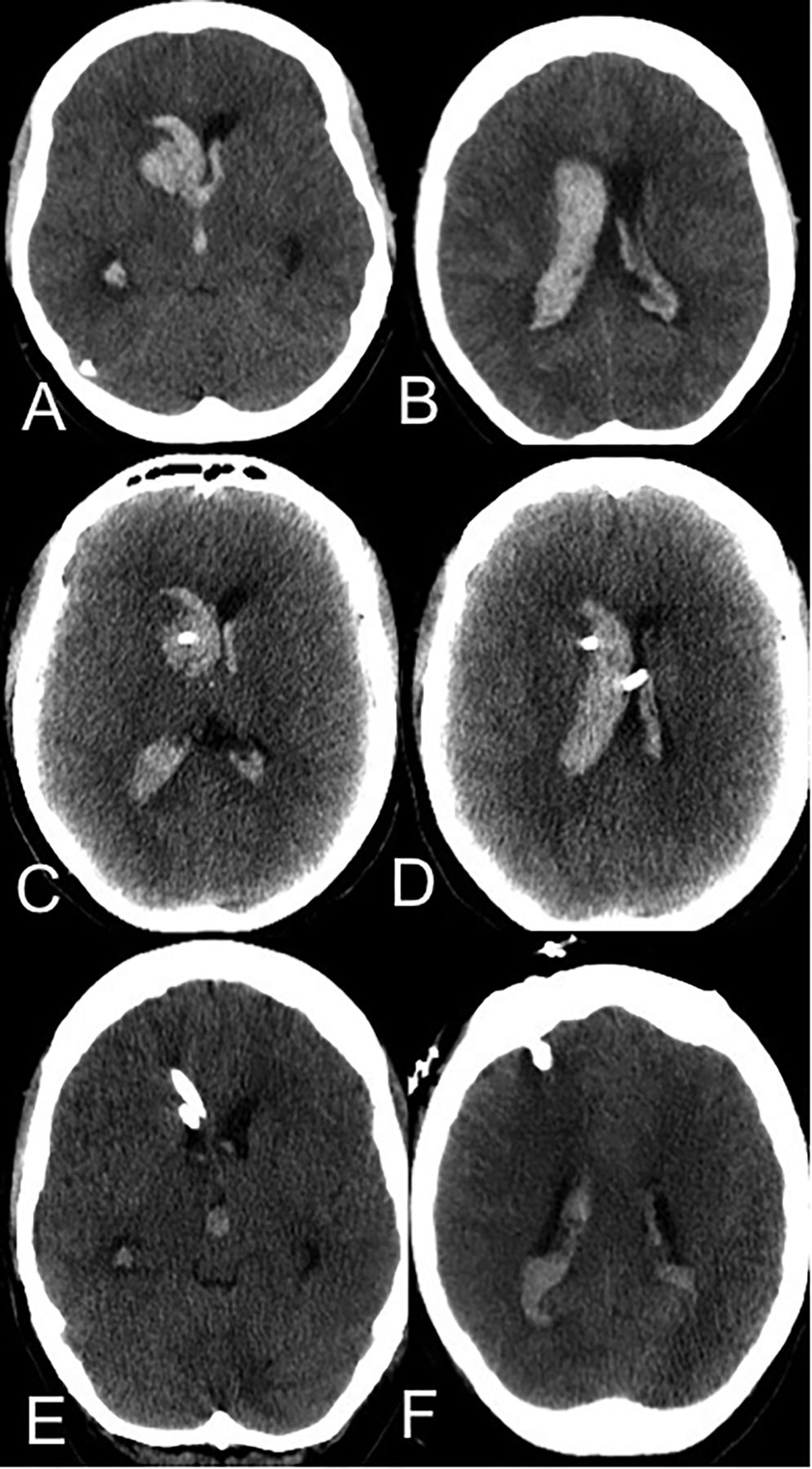
A 43-year-old woman with a parenchymal hemorrhage with intraventricular extension. Axial CT images (A, B) from the transferring hospital demonstrate a right caudate hemorrhage with rupture into the ventricle, a large intraventricular hemorrhage, and hydrocephalus. Following emergent placement of bilateral external ventricular drains, CT at approximately the same anatomical levels (C, D) shows a small reduction in the size of the left lateral ventricle with little change in the right lateral ventricular size or the volume of the intraventricular hemorrhage. Following a single pass with the Apollo system via a right frontal burr hole and placement of a third ventricular catheter, axial CT images (E, F) at approximately the same anatomical levels demonstrate complete evacuation of the right caudate hemorrhage and clearance of blood products from the frontal horn and body of the right lateral ventricle with a reduction in ventricular size.
After 12 h of ventricular drainage, her pupillary function returned and as a best motor response she withdrew her right upper extremity to noxious stimuli. Her NIHSS score was estimated to be 22.
Apollo evacuation was performed on the following day (PBD 1). The goal of the procedure was to evacuate the right caudate parenchymal hemorrhage as well as the portion of the ventricular hemorrhage within the right frontal horn. This was achieved with a single Apollo pass with actuation of the wand for a total of 52 s. A third ventricular catheter was placed through the right frontal burr hole into the region of the right foramen of Monro. No complications were encountered.
The patient emerged from anesthesia at her neurological preprocedural baseline but improved rapidly. On postoperative day 4 she was extubated and able to follow commands with all extremities. Her NIHSS score improved to 6 (2 for incorrect age and month, 1 for facial droop, 1 for left upper extremity pronator drift, 1 for dysarthria, and 1 for gaze preference).
Discussion
The present case series demonstrates the feasibility of the minimally invasive evacuation of intracranial hemorrhage using the Apollo system.
Parenchymal hemorrhage is a common neurological disease with high rates of associated mortality and morbidity.3 ,4 If complicated by intraventricular hemorrhage, the prognosis is even worse.5 ,6 No medical or surgical interventions have been demonstrated to improve outcomes thus far.7–10
The neurological injury created by parenchymal hemorrhage has been proposed to have two distinct phases. At the onset, the hemorrhage directly injures the regional brain through simple mechanical disruption.11 In the hours and days that follow, additional injury to the surrounding brain ensues, which is theorized to be a result of the direct toxic effect of blood products on the surrounding brain parenchyma and possibly local mass effect from the hematoma inducing regional ischemia in the surrounding parenchyma.12 ,13 This regional injury surrounding the hematoma is manifest on neuroimaging as perihematomal edema (PHE). Edema usually increases quickly within the first 24 h, peaks at 5–6 days, and then may begin to resolve.13–15 However, in some cases, significant delayed progression of PHE with associated mass effect can be observed even 2–3 weeks after the original hemorrhage.16
It is conceivable that early evacuation of the hemorrhagic products could mitigate or eliminate this delayed injury. However, trials of surgical hematoma evacuation have failed to show a clinical benefit.5 ,17 This failure has been attributed to the injury to normal brain tissue created by the surgical approach to the hematoma—particularly for deep hemorrhages. These findings fostered the belief that a less invasive means of hematoma evacuation could potentially be beneficial. After a series of encouraging small case series and trials, the Minimally Invasive Surgery and Tissue Plasminogen Activator (tPA) in Intracerebral Hemorrhage Evacuation (MISTIE II) trial compared a strategy of minimally invasive hematoma drainage with medical management.18 ,19 The intervention consisted of the stereotactically guided manual syringe aspiration of the hematoma using a 14 F cannula, followed by placement of a drainage catheter within the cavity, which could be irrigated with tPA to maintain its patency.20 The investigators found that the interventional procedure reduced PHE, and also demonstrated the potential to reduce length of stay and improved clinical outcomes measured at 1 year.20 ,21 Moreover, the investigators observed that, in general, greater reductions in clot size correlated with better patient outcomes, particularly if the clot volume could be reduced to under 10 mL by the end of treatment.21 However, this degree of clot reduction was only achieved in a small proportion of patients in MISTIE II, even after days of catheter irrigation with tPA. The average volume of residual clot at the end of treatment in MISTIE II was 19.6 mL.20
The Apollo system is specifically designed for the minimally invasive evacuation of tissue and fluids, including hemorrhage. The Apollo wands, which measure 2.1 or 2.6 mm in diameter, maintain their patency during hematoma evacuation by virtue of an internal agitator wire, which vibrates when actuated and macerates the hematoma during aspiration to prevent the apparatus from clogging. The Apollo system, particularly if used under direct endoscopic visualization with periodic active monitoring of progress with CB-CT, should be considerably more reliable in achieving an optimal level of hematoma volume reduction (<10 mL) than the MISTIE surgical technique—manual aspiration of a 14 F sheath to initial resistance. It follows that the Apollo procedure itself could effectively achieve optimal levels of clot reduction (to <10 mL) immediately in most patients, without the requirement for placement of a drainage catheter or days of tPA irrigation. Conceivably, this more reliable and efficient minimally invasive means of hematoma evacuation could result in even further improvement in patient outcomes.
In our series, we employed multiple technologies in an attempt to optimize the safety and extent of hematoma evacuation. Firstly, neuronavigation was performed to plan the surgical approach, place the endoscopic working sheath, and document the location of the sheath with respect to the hematoma throughout the procedure. The endoscopic sheath is quite mobile and is easily displaced during manipulation of the endoscope and Apollo wand, and therefore active monitoring of its position during the procedure was critical. Secondly, endoscopic visualization was performed with the trocar maintained entirely within the working sheath. This technique provides a limited, but useful, visualization of the operative field at the end of the sheath and allows direct observation of the Apollo wand during aspiration and actuation. Visualization of the field at the tip of the sheath is helpful in localizing residual hemorrhage for targeted aspiration with the Apollo wand and for differentiating hematoma from surrounding brain tissue, thereby eliminating unnecessary manipulation and injury to surrounding brain and potentially reducing the risk of inducing additional bleeding. Moreover, direct visualization of the interaction between the Apollo wand and the hematoma is very helpful, as it allows strategic manipulation of the wand, pulsation of the suction, and application of irrigation to optimize the efficiency of clot removal. Finally, the endoscope provides an opportunity for targeted irrigation and potentially cautery in the case that additional active bleeding is encountered, although depending on the visualization this capability might be quite limited. Thirdly, active monitoring with periodic CB-CT allowed an immediate assessment of the procedure by demonstrating the volume and location of any residual hematoma as well as elucidating any associated procedural complications. The procedure could then either be terminated or immediately continued without moving the patient. In addition, any complications, particularly rebleeding, could be immediately identified and addressed. When substantial residual hematoma was identified (case No 1), the CB-CT data were uploaded to the neuronavigation system and used to create a new trajectory to the targeted residual hematoma and to guide re-placement of the endoscopic sheath. Accessibility to CB-CT makes the angiographic suite or hybrid operating room an optimal environment for these procedures. Thus each of the technologies used offers its own unique advantages, which (particularly at this early stage of experience with the procedure) are complimentary and potentially maximize both the safety and technical efficacy of the Apollo system.
There are several important limitations of the present series. Firstly, while the patients in the present series had dramatic clinical improvements following the procedure, it is possible that these improvements may have also occurred (with time) with standard conservative medical treatment. Until a larger clinical experience is available and ultimately a clinical trial performed, it will be difficult to determine with certainty the efficacy of this procedure. Secondly, the current Apollo system is in its first iteration, and the application of the system within the context of multimodality imaging guidance, direct visualization, and real time CB-CT monitoring described here is a technique that remains to be perfected. It is likely that as we learn more about the behavior and application of the Apollo system, and as the device and ancillary equipment is iterated, that some of the technologies may become unnecessary and the procedure simpler.
Conclusions
The Apollo system can be used within the neuroangiography suite for the minimally invasive evacuation of intracranial hemorrhage using simultaneous neuronavigation for planning and intraprocedural guidance, direct visualization with neuroendoscopy, and real time monitoring of progress with CB-CT.
References
Footnotes
Contributors All authors made a significant contribution to this manuscript. All authors made substantial contributions to conception and design, acquisition of the data, or analysis and interpretation of the data.
Funding The Apollo program at Stony Brook University Medical Center is supported by a grant from the Stony Brook Auxiliary and the Corso Family Charitable Foundation Inc, Cutchogue, New York, USA.
Competing interests None.
Patient consent Obtained.
Ethics approval The study was approved by the institutional review board of Stony Brook University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.