Article Text

Abstract
Objective Acute basilar artery occlusion (BAO) is a catastrophe with high mortality and disability. Randomized controlled trial (RCT) data supporting/refuting reperfusion treatment are sparse in acute BAO. The study objective was to pool risk estimates for death or dependency (DoD), mortality, and intracerebral hemorrhage (ICH) from published studies on BAO.
Methods Medline, Embase, The Cochrane Library, and clinicaltrials.gov were searched through August 2013 for studies of reperfusion therapies in acute BAO. Two independent authors selected studies and abstracted the data. Pooled risk ratios (RR) and mean weighted probabilities (MWP) were calculated using random effects model.
Results 45 studies (n=2056) met the inclusion criteria. Recanalization was associated with a lower risk of DoD (RR 0.67; number needed to treat (NNT) 3) and mortality (RR 0.49; NNT 2.5). ICH rate (MWP) with acute therapies was 13%. With recanalization, RR for DoD in those treated ≤12 h was 0.63, and for those treated >12 h, it was 0.67. With recanalization, RR for DoD in the intravenous thrombolysis (IVT) subgroup was 0.68; in the intra-arterial/endovascular therapy (IA/EVT) subgroup, DoD RR was 0.67. Recanalization resulted in mortality RR of 0.46 in those treated ≤12 h; for >12 h group, RR was 0.50. Recanalization resulted in mortality RR of 0.53 in the IVT subgroup, and RR of 0.48 in the IA/EVT subgroup. ICH rate for ≤12 h was 10%; ICH rate for >12 h was 14%. With IVT, the ICH rate was 9%, and with IA/EVT the ICH rate was 14%.
Conclusions Recanalization of acute BAO leads to reduction in mortality by two-fold and reduction in the risk of DoD by 1.5-fold. This study underscores the equipoise in acute BAO for comparing systemic and endovascular therapies, and testing different time windows through RCTs.
- Artery
- Intervention
- Stroke
- Thrombolysis
- Thrombectomy
Statistics from Altmetric.com
Introduction
Acute basilar artery occlusion (BAO) is a fatal form of stroke with a likelihood of death and disability of the order of 70–80%.1–6 Randomized trials of acute therapies are lacking in acute BAO with only one small randomized controlled trial (RCT, eight patients in each arm) favoring intra-arterial thrombolysis.7 Acute stroke therapies are based on the premise that recanalization of occluded vessels improves clinical outcome through reperfusion and salvage of at risk tissue. Recanalization has been adopted as a marker of treatment effectiveness in recent trials of thrombolytic and endovascular therapy in ischemic stroke. Food and Drug Administration uses the efficacy endpoint of recanalization as the basis of labeled approval of thrombectomy catheter devices for use in patients with acute ischemic strokes.
Although the recanalization hypothesis has been investigated and confirmed in previous studies on anterior circulation stroke, it has not been definitively confirmed for acute BAO.8 A wealth of observational data on the treatment of acute BAO has accumulated over decades but the lack of a control group in these studies precludes a direct comparison of reperfusion therapies utilized to treat acute BAO.
To systematically address the recanalization hypothesis in acute BAO, we adopted the approach of using the radiological endpoint of recanalization as the basis of comparison of meaningful clinical outcomes between the two arms, one in which the radiological endpoint (ie, recanalization) was achieved and the other where the endpoint failed to occur. Given the absence of RCTs to guide treatment, in the interest of timely informed decisions in public health and clinical practice,9 we sought to synthesize outcome and mortality estimates from the available studies on acute BAO.
Subjects/materials and methods
We used a predesigned protocol for literature search, study selection, data synthesis, and sensitivity analysis. We adhered to the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines.9
Search strategy and study selection
MEDLINE, EMBASE, The Cochrane Library, and clinicaltrials.gov were searched (through August 2013) to identify relevant studies in the literature with keywords and terms—‘basilar artery’, ‘basilar artery occlusion’, and ‘acute ischemic stroke’. No limits were applied to the searches. Titles and abstracts were screened by two independent authors, and articles were retrieved if they were relevant or if there was uncertainty. Bibliographies of identified studies as well as relevant reviews in the field were manually searched for potentially eligible studies. Full texts were reviewed when a decision about inclusion could not be made by screening the title and abstract. Where duplicate publication was suspected, study authors were contacted for clarification. Study authors were also contacted where needed for verification and confirmation of data.
All study designs (retrospective and prospective) were allowed. Observational studies reporting at least 10 consecutive patients, intravenous therapy (IVT) (with recombinant tissue plasminogen activator), intra-arterial thrombolytic therapy, and/or endovascular therapies (IA/EVT) were included. All mechanical endovascular approaches were allowed. Only studies evaluating acute BAO were included. Studies or registries reporting on basilar disease where data pertaining to acute BAO could not be parsed were excluded. Studies of intracranial artery occlusions other than basilar were excluded. Studies that reported fewer than 10 patients with acute BAO, regardless of the total number of patients in the study, were excluded.
Other exclusion criteria were: publication of abstracts only, case reports, letters, comments, reviews, or meta-analyses only; animal studies; languages other than English; duplicate studies; no intervention of interest (IVT or IA/EVT); lack of outcomes of interest (functional outcome, mortality, intracerebral hemorrhage (ICH)); and not population of interest (adults >18 years). Conflicts were resolved with discussion and input from the third author.
Data extraction and study quality
Two authors independently abstracted data into a standard data form. The abstracted data were then compared and any discrepancies evaluated and resolved with discussion and input from the senior author. Study authors were contacted when the article failed to provide the necessary information. Data pertaining to treatment modality (IVT or IA/EVT), functional outcome (modified Rankin Scale (mRS) score, Barthel Index, National Institutes of Health Stroke Scale, etc), mortality, ICH, and onset to treatment time (OTT) window were extracted. Binary data were separately extracted into recanalized and non-recanalized arms for each outcome. Where data for an outcome were not separable between recanalized and non-recanalized arms, data were extracted as rates for the entire study cohort in a single variable.
Poor outcome (death or dependency) was defined as an mRS score of >3. If the study used another definition but where data were available, death or dependency was recomputed as mRS >3. When no data were available to recompute mRS, the study definition of death or dependency was followed. When available, outcome status at 3 months post-stroke was used. If assessments at 3 months were not performed, the reported final assessment closest to 3 months was used. ICH was defined as any ICH reported in the study. OTT windows were dichotomously split into ≤12 and >12 h based on the treatment window reported by the study. Studies that did not report OTT window were grouped in the >12 h OTT group.
In addition, data pertaining to trial quality and design were extracted and tabulated. All studies were evaluated for quality using a 6 category scoring system (range 0–6).10 The categories were: (1) definition of inclusion/exclusion criteria, (2) reported recanalization, (3) recanalization defined by a standard grading system, (4) outcome defined by mRS, (5) a priori definition of a window of treatment, and (6) reported symptomatic ICH. Studies received a score of 1 if the study fulfilled the criteria and 0 otherwise. After ensuring the accuracy of the extracted data, the two data forms were merged into a single form.
Statistical analysis
Publication bias
Publication bias was evaluated with Begg's and Egger's tests (significance p<0.05).11 ,12 Funnel plots were generated for visual appraisal of publication bias. Trim and fill algorithm analysis was planned a priori for adjusting the effect of publication bias on the pooled estimate13 ,14 in the event that publication bias was significant.
Heterogeneity
Heterogeneity between the studies was calculated using the χ2 test for heterogeneity (Cochran Q test). A p value <0.5, corresponding to Q>df, was regarded as significant for detection of statistical heterogeneity. Heterogeneity was quantified using I2 (I2=(Q−df)×100/Q, where df=k−1, Q=Cochran Q, df=degrees of freedom, and k=number of studies),15 and between study variance expressed as τ2. I2>50% was regarded as significant.
Data synthesis
A DerSimonian and Laird random effects model was used to synthesize data for all analyses (the random effects model defaulted to a fixed effects model when heterogeneity was absent).16 Forest plots were generated to illustrate synthesis. Pooled estimates were expressed as risk ratio (RR) and 95% CI. CI ranges that excluded 1 were regarded as significant. Number needed to treat (NNT) was calculated using the pooled risk difference (RD) for those syntheses that produced significant results. Data extracted as single group rates and sample sizes were converted with a Freeman–Tukey double arc sine and SEs calculated. These were then transformed to a probability scale during meta-analysis, yielding mean weighted probabilities (MWPs) with 95% CI.
Sensitivity analyses
Sensitivity analyses were planned a priori to account for heterogeneity. Subgroup syntheses were performed based on the mode of therapy (IVT, IA/EVT) and OTT window (≤12, >12 h). Quality score was used for a priori designed sensitivity analysis for study bias integration. Quality score was incorporated into the synthesis in Doi and Thalib's quality effects regression model yielding quality adjusted pooled estimates of death or dependency and mortality.17 To test the robustness of the syntheses, exclusion sensitivity analysis was performed to evaluate the extent to which each trial influenced the result of the synthesis. For this, each study was excluded, one at a time, and the combined value without a particular study calculated. All analyses were performed on Mix V.2.0 Pro statistical package.
Results
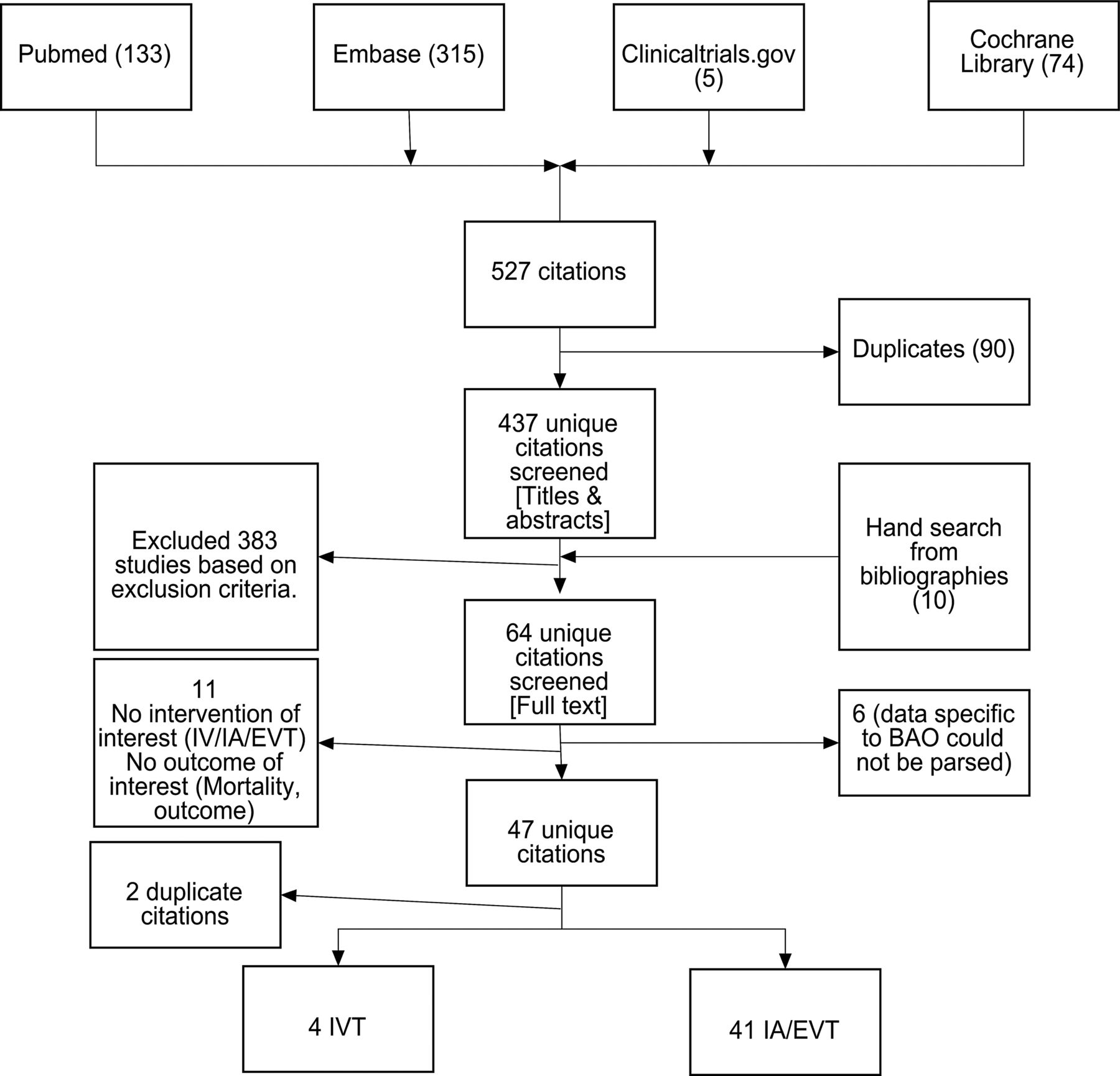
Search strategy and study selection are outlined in the flow diagram (figure 1). Forty-five studies (n=2056) met the inclusion criteria. The overall recanalization rate (MWP) was 75%. Recanalization rates were better with IA/EVT (77%; n=1715) than with IVT (59%; n=341), and among those with OTT within 12 h (81%; n=426) than those with OTT >12 h (73%; n=1630). Study characteristics are summarized in the online supplementary table (table e1).

Literature search and study selection. BAO, basilar artery occlusion; EVT, endovascular therapy; IA, intra-arterial; IV, intravenous; IVT, intravenous thrombolysis.
Syntheses
Thirty-six studies (n=1800) provided data on death or dependency. Publication bias was significant on Begg's (p=0.001) and Egger's (p<0.001) tests (figure 2A, B). Statistical heterogeneity was found but the percentage of total variance attributable to heterogeneity was not significant (I2<50%). Recanalization was associated with a 1.5-fold reduction in the risk of death or dependency (NNT=3; RD=0.32) (figure 2C).
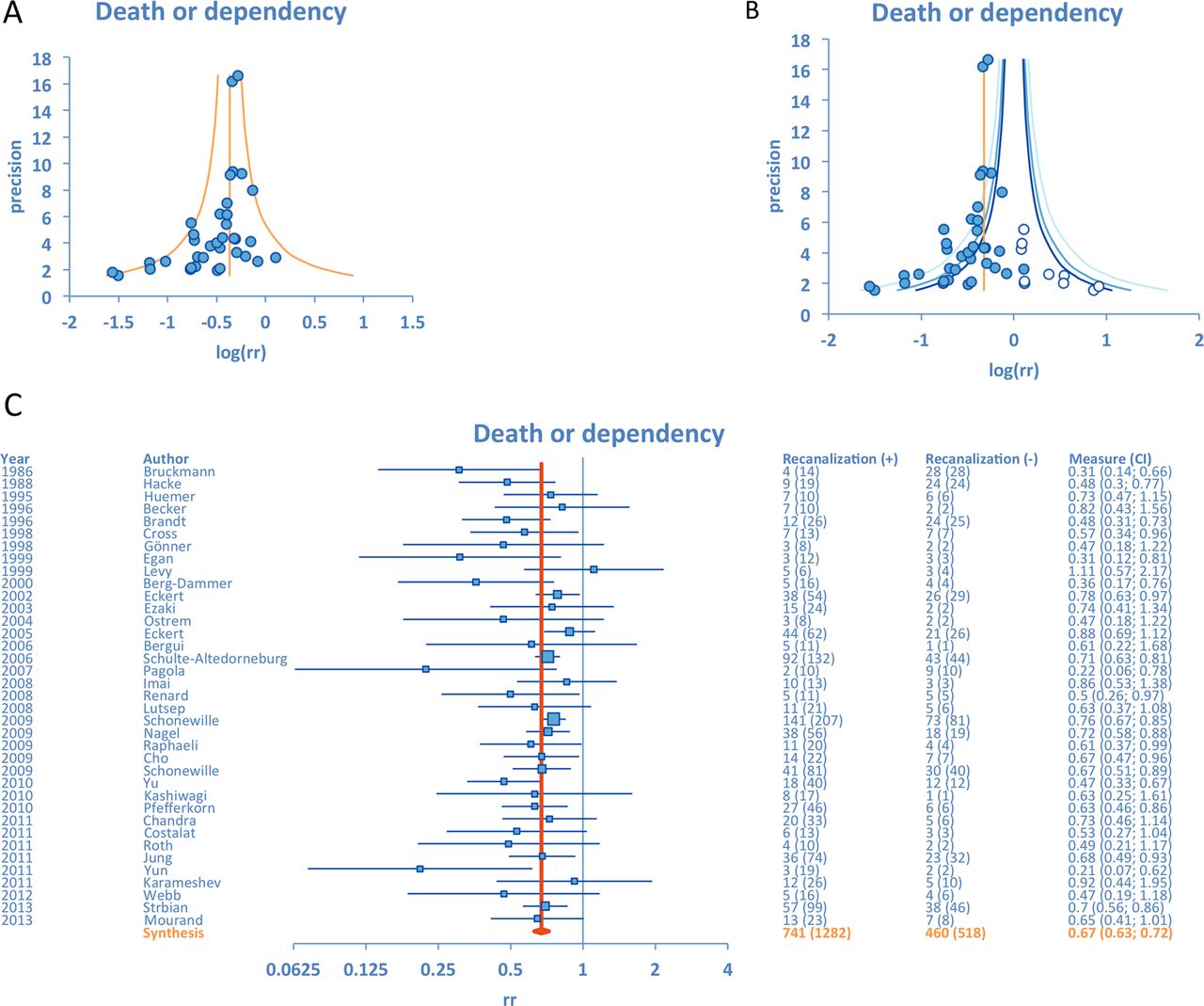
(A) Funnel plot for the synthesis of death or dependency. Publication bias was significant on Begg's and Egger's tests. Each study is represented by a single equally sized dot. With pseudo-CIs integrated into the plot, it can be used to assess how heterogeneous the studies are and which studies are relative outliers. Inverse SE is on the y axis and a log transformed ratio measure of effect size (log risk ratio) is on the x axis. (B) Trim and fill algorithm is used to impute studies that appear to be ‘missing’ due to selective dissemination. Each study is represented by a single equally sized dot and imputed studies by empty circles. Trim and fill plot shows p value limit reference lines instead of the pseudo-CIs in the funnel plot. The trim and fill plot assesses the extent of selective dissemination of evidence. This is done by checking for asymmetry (missingness of studies on one side) of the lower regions of plot, and in particular, missingness in regions of non-significance (p values >0.05). Thus, for the assessment of the possibility of selective evidence dissemination, one should be particularly interested in missingness between the central p value limits of the plot. (C) Forest plot of association between recanalization and death or dependency.
Thirty-eight studies (n=1843) provided data on mortality. Publication bias was not significant on Begg's but borderline significant on Eggers’ (p=0.07) test (figure 3A, B). Statistical heterogeneity was found but the percentage of total variance attributable to heterogeneity was not significant (I2<50%). Recanalization was associated with a two-fold reduction in the risk of mortality (NNT=2.5; RD=0.39) (figure 3C).
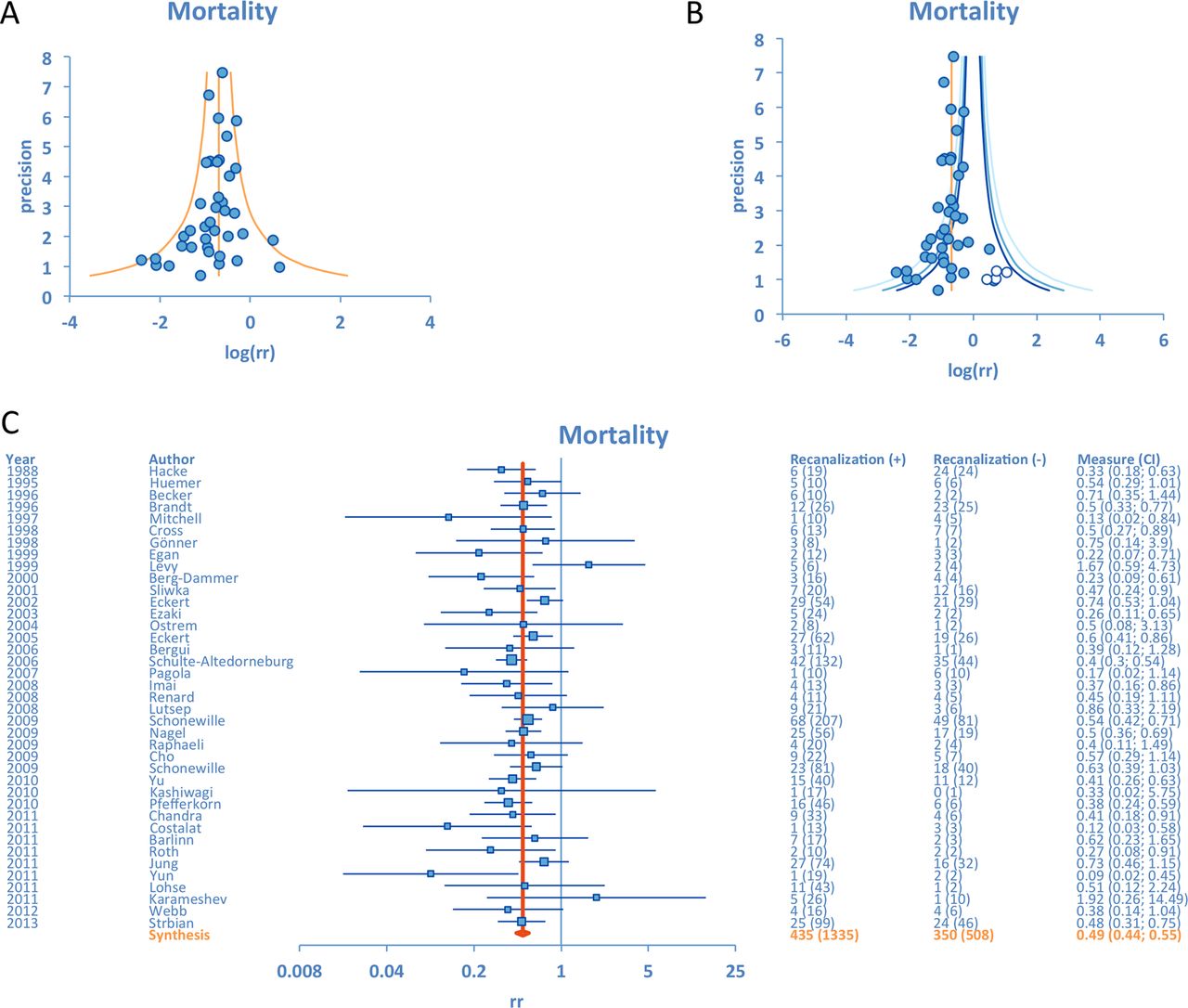
(A) Funnel plot for the synthesis of mortality. Publication bias was borderline significant on Egger's test (p=0.07). (B) Trim and fill plot for dissemination bias in the synthesis of mortality. (C) Forest plot of association between recanalization and mortality.
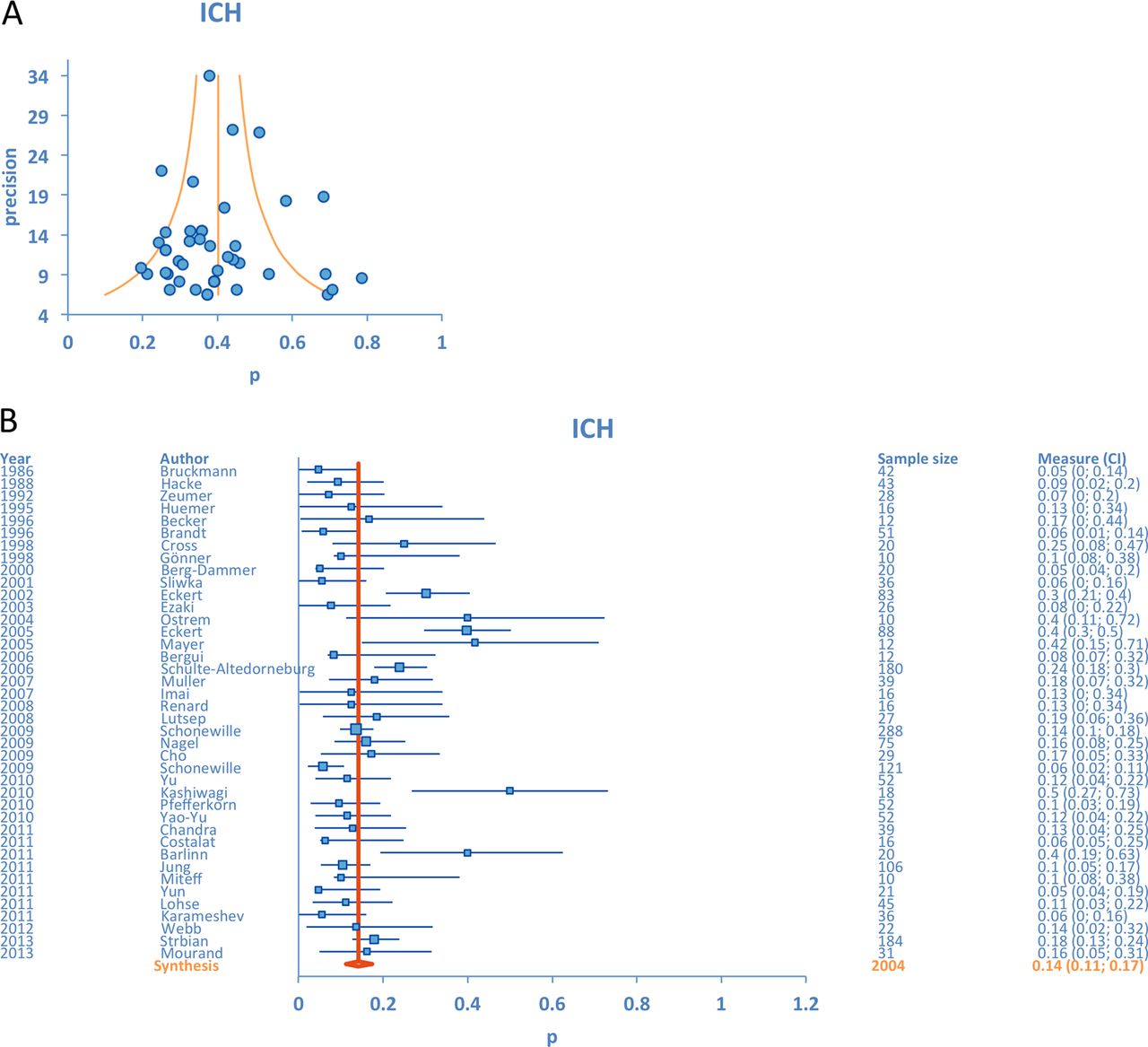
Forty-one studies (n=2060) provided data on ICH. Data for ICH were not separately extractable under recanalized and non-recanalized arms and therefore MWP were synthesized. Publication bias was not significant on Begg's and Egger's tests (figure 4A). Heterogeneity was significant (I2>50%) in the synthesis for ICH. Overall rate of ICH was 13% (figure 4B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Funnel plot for intracerebral hemorrhage (ICH). Publication bias was not significant. (B) Pooled mean weighted probability of ICH.
Pooled unadjusted and publication bias adjusted RR are shown in table 1.
Heterogeneity and pooled estimates in primary syntheses and sensitivity analyses
Sensitivity analysis
For death or dependency and mortality, subgroup analyses based on OTT window and mode of therapy accounted for heterogeneity. For these outcomes I2 remained insignificant for all syntheses and trends explained heterogeneity (table 1). Pooled estimates remained significant with syntheses based on OTT window, type of therapy, and quality adjustment.
For ICH, subgroup analyses based on OTT window accounted for heterogeneity. For ≤12 h, I2 became insignificant and the rate of ICH was 10%. For >12 h, I2 remained significant and the ICH rate was 14%. I2 remained significant for IVT and IA/EVT, and rates were 9% and 14%. The quality adjusted ICH rate was 14%.
Syntheses for all three outcomes were robust to the exclusion sensitivity analysis, and exclusion of no single study influenced the significance of the pooled estimate (see online supplementary figure e1).
Discussion
Our comprehensive systematic review and meta-analysis based on literature published through August 2013 confirms that recanalization impacts final clinical outcome in acute BAO. Recanalization of acute BAO results in a two-fold reduction in mortality and 1.5-fold reduction in death or dependency. The composite ICH rate was 13%, and lower in those treated ≤12 h (10%) and in those treated with IVT (9%). Recanalization rates of 75% overall, 59% with IVT, and 77% with IA/EVT are comparable with the rates reported in the RCTs of reperfusion therapies.
Our study has various strengths and advantages over a previous meta-analysis that reported death or dependency rates of 78% with IVT (n=76) and 76% with IAT (n=344).18 We included a greater number of patients and found 68% death or dependency rate with IVT (n=302) and 67% with IA/EVT (n=1498). A previous meta-analysis reported 50% mortality rate with IVT and 55% with IAT. We found mortality rates of 53% with IVT (n=302) and 48% with IA/EVT (n=1541). Rates reported in the previous study are mere percentages whereas our rates represent MWPs computed from a random effects meta-analysis. Decline in mortality and death or dependency rates is partly a function of increased precision given the larger number of patients in our study. Improvement in medical care and development of modern reperfusion techniques over time is likely also contributory as our meta-analysis includes more recent studies. Cumulative Forest plots illustrate that rates of death or dependency have declined over time, shifting the body of evidence further in favor of recanalization (see online supplementary figure e1). Like the previous meta-analysis, death or dependency rates were comparable between IA/EVT and IVT. But unlike the previous study, we found lower mortality with IA/EVT compared with IVT. This likely reflects use of devices with faster and more efficient recanalization rates in the more recent studies.
A strong suit of our study is the study design. While an RCT eliminates biases by ensuring lack of prior knowledge of treatment assignments between the two arms, comparison of a reperfusion therapy to conventional therapy (antiplatelet/antithrombotic) in acute BAO is viewed as unethical.19 In the absence of such RCTs, our meta-analysis design entailed that study authors had no prior knowledge of which patient will recanalize and which patient will fail to achieve recanalization. With the mechanistic reasoning that since the original studies were not designed to compare outcomes between recanalized and non-recanalized patients or between methods of achieving recanalization, the two arms in our analysis were balanced. We ensured redundancy in study selection and data extraction to minimize errors, and applied appropriate statistical methods to address issues of publication bias, heterogeneity, and study quality.
To adjust for heterogeneity from a variation in quality across studies, we reported quality adjusted pooled estimates of outcomes that were unchanged from the original. We also evaluated and accounted for publication bias, a major threat to the validity of observational study meta-analyses. Dissemination bias adjustment did not sizably change estimates of mortality and death or dependency. We reported heterogeneity and performed a priori designed sensitivity analyses to account for it when statistical heterogeneity was found. We demonstrated the robustness of our estimates with exclusion sensitivity analysis.
Our study has certain limitations. Despite our perceived balance of the two arms, observational studies lack the inherent bias elimination failsafe of randomization. Meta-analyses of RCTs are based on the assumption that each trial provides an unbiased estimate of treatment effect, with the variability between study results being attributed to random variation. Conversely, observational studies yield estimates that may deviate from true underlying relationships beyond the play of chance. Meta-analysis of such studies has the potential to be biased. However, we believe that our thorough consideration of possible sources of heterogeneity between study results provides more insights than the mechanistic calculation of an overall measure of effect, which could be biased. We found heterogeneity and reported percentages of total variation attributable to heterogeneity (I2). We were able to account for heterogeneity with our subgroup analyses based on treatment window and type of therapy.
Our subgroup analyses raise new questions while answering others. The analyses based on treatment window and modes of therapy explain heterogeneity found in the syntheses of death or dependency, mortality, and ICH. IA/EVT introduced heterogeneity in the syntheses for death or dependency and mortality. IA/EVT studies were more variable in design given the variety of mechanical and intra-arterial approaches used, and variability in anticoagulant use across studies. Recently, failure of RCTs of endovascular therapies was partly attributed to a lack of sufficient numbers of patients treated with newer generation devices capable of achieving faster and more complete recanalization.20 ,21 Development of devices that achieve faster and more efficient recanalization combined with standardization in the performance of endovascular procedures may improve outcomes.
OTT window >12 h introduced heterogeneity in the syntheses for death or dependency, mortality, and ICH. This is attributable to a wide range of windows used, the longest being no window at all. For ICH synthesis, OTT window >12 h was a more important source of heterogeneity than mode of therapy. OTT and onset to recanalization times have been recently shown to be paramount in determining outcome in patients with ischemic stroke.22 ,23 For ICH, heterogeneity is also accounted for by variation in severity as well as definition of ICH. As data pertaining to symptomatic ICH were not separable nor were data able to be grouped into recanalized and non-recanalized arms, the purport of this synthesis is limited.
Sources of heterogeneity other than treatment and time may influence outcome. Year of publication introduces heterogeneity as healthcare and technological improvements over time may result in improved outcomes. Country of origin introduces heterogeneity as practice patterns, guidelines, and protocols vary between countries. Quality metrics other than what we accounted for introduce heterogeneity. These are lost to follow-up, variation in outcome definition, time of outcome assessment, variation in recanalization definition, operator skill and experience, variability in blood pressure management, use of antithrombotics and anticoagulants, etc.
We did not find large differences in the estimates of death or dependency and mortality between IVT and IA/EVT. This is not evidence of a lack of difference between the two therapies. There was great imbalance between the number of IVT (n=4) and IA/EVT studies (n=41) in this meta-analysis. While assessment of revascularization is intrinsic to an intra-arterial procedure, it is not routine after IVT. Our pooled weighted recanalization rate of 59% with IVT is driven by the two largest IVT studies that carry most weight in the meta-analysis, those by Schonewille (n=121) and Strbian (n=184) that reported 67% and 54% recanalization rates, respectively.24 ,25 Post-treatment CT angiography, MR angiography, transcranial Doppler, or conventional angiograms were obtained in 88% in Schonewille's study, hours to days post-thrombolysis. Post-treatment angiography (MR angiography or CT angiography) was obtained in 79% by Strbian et al 24 h post-thrombolysis. The other two studies provide smaller but measurable contributions. Pagola et al (n=20) reported 50% recanalization rate by transcranial Doppler (all patients) while Huemer (n=16) reported 63% recanalization rate assessed by transcranial Doppler (n=14) and conventional angiogram (n=2).26 ,27 Our demonstration that (a) recanalization is associated with better outcomes regardless of the way recanalization was achieved and (b) 77% of IA/EVT patients achieved recanalization compared with only 59% of those treated with IVT seems to favor IA/EVT. That said, the observational study design does not allow a statistically valid comparison of the two therapies, as attempted in the previous meta-analysis.18 Hence equipoise still exists between the two strategies.
The significant treatment effect shown by our analysis in this catastrophic illness makes it unethical to justify an RCT to study the benefit of recanalization against antiplatelet/antithrombotic therapy, even outside the conventional window for IVT. Nonetheless, we believe there is equipoise for carefully designed studies to answer questions about the preferred reperfusion strategy, appropriate OTT and onset to recanalization windows, and role of anticoagulants in acute BAO.
In conclusion, recanalization is associated with a two-fold reduction in mortality (NNT 2.5) and 1.5-fold reduction in death or dependency (NNT 3). These data do not support the notion that intra-arterial/mechanical therapies are superior to intravenous recombinant tissue plasminogen activator. These results underscore the need for RCTs in acute BAO.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors GK designed the study, performed the literature search, selected the studies for inclusion in the meta-analysis, abstracted the data, performed the statistical analysis, and wrote and revised the manuscript. RBS performed the literature search, selected the studies for inclusion in the meta-analysis, abstracted the data, and revised the manuscript. AVA selected the studies for inclusion in the meta-analysis, supervised the conduct of the study, and revised the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.