Article Text

Abstract
Background and objectives Although the recently marketed stent retriever thrombectomy devices have demonstrated a high recanalization rate and favorable clinical outcomes, there is a concern about the risks of intimal injuries when pulling out the stent in the unfolded position. In this study, the Solitaire Flow Restoration System and the Trevo retriever were used in a histopathological comparison of vascular injuries caused by stent retriever thrombectomy devices.
Methods Rabbit carotid arteries were used in the experiments with stent retriever thrombectomy devices. Carotid artery samples were harvested either 1 or 2 weeks postoperatively for histological examination.
Results Histological changes caused by the use of stent retriever thrombectomy devices were observed from the intimal to medial layers. With the Solitaire FR 4 mm, intimal and medial thickening was observed 1 week postoperatively, and progression of intimal thickening was observed 2 weeks postoperatively. The extent of intimal thickening tended to be greater with the Solitaire FR 6 mm than with the Solitaire FR 4 mm, but this difference was not significant. Compared with the Solitaire FR 4 mm, the Trevo had a significantly smaller area of intimal thickening.
Conclusions Although there are some differences among devices, results from this study indicate that stent retriever thrombectomy devices induce vascular damage that extends to the medial layer.
- Intervention
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
The new stent retriever thrombectomy device has demonstrated a high recanalization rate and favorable clinical outcome compared with the Merci retriever (Stryker Neurovascular),1 ,2 and two types of these devices, the Solitaire Flow Restoration System (Solitaire FR by Covidien) and the Trevo retriever (Trevo by Stryker Neurovascular), have become available in Japan since July 2014.
A direct aspiration first pass technique (ADAPT) has also been shown to have a high recanalization rate and good clinical outcome, similar to the stent retriever. The potential for endothelial injury is thought to be low, on the grounds that the clot is extracted using an aspiration catheter.3 ,4
Recent randomized control trials of mechanical thrombectomy versus conservative treatment demonstrated the positive effect of mechanical thrombectomy.5–9 In these trials, most of the mechanical thrombectomy devices were stent retrievers. Therefore, these devices have been highly anticipated in the treatment of acute cerebral infarction.
On the other hand, there are risks of intimal injuries when pulling out the stent in the unfolded position. In animal models, microendothelial trauma was histologically observed after stent retriever use.10 Kurre et al11 reported that de novo stenosis and occlusions occurred in a small proportion of patients after mechanical thrombectomy. Endothelial injury during mechanical thrombectomy may exacerbate the secondary neural injury resulting from the inflammatory pathway via tumor necrosis factor α or interleukin 1β initiated at the injured endothelium, and may contribute to a futile recanalization.12–14
For mechanical thrombectomy, it is important to understand the characteristics of endothelial injury induced by the devices. Hence research into endothelial injury resulting from mechanical thrombectomy may have some merit.14 ,15
In the present study, the Solitaire FR and the Trevo were used in a histological comparison of the vascular injuries caused by these stent retriever thrombectomy devices.
Materials and methods
All procedures were performed in accordance with international guidelines, and were approved by the ethics review board. Male New Zealand white rabbits (body weight 2.5–3.0 kg) were purchased from Japan SLC (Shizuoka, Japan). Anesthesia was maintained with isoflurane after administration of 1.0 mL barbiturate via the auricular vein. Oxygen was also administered at the same time. After fixing the animal to the surgical board in a supine position, the right inguinal region was shaved, and local anesthesia (1% xylocaine) was administered. Subsequently, the right femoral artery was exposed, and a 4 F short sheath was inserted. A microcatheter was carefully advanced to the carotid artery, and the thrombectomy device was placed and deployed. Subsequently, the stent was pulled out with constant force. All of these procedures were performed once per blood vessel. The detailed study design, stent retriever thrombectomy device used, and delivery catheters are described in table 1.
Study design
Rabbits were sacrificed by barbiturate overdose 1 or 2 weeks after the procedure. Fixation was conducted with 4% paraformaldehyde perfusion, and the carotid artery was collected.
Histological examination
Harvested carotid artery samples were cut along the short axis into five parts, fixed in 4% paraformaldehyde overnight, and subsequently embedded in paraffin. Samples were sectioned at a thickness of 5 μm and stained with H&E. Samples were examined with a light microscope at 20× magnification.
Areas of tunica intima and media were quantified using Adobe Photoshop CC by measuring the number of pixels. The tunica intima (‘intima’) was defined as the space between the endothelial cells and the internal elastic lamina, and the tunica media (‘media’) was defined as the space between the internal elastic lamina and the adventitia.
Statistical analysis
Data analysis was conducted using JMP11 (SAS Institute Inc, Cary, North Carolina, USA). Areas are expressed as means±SD and were compared using the Mann–Whitney test. A p value <0.05 was considered significant.
Results
Histological changes caused by the use of stent retriever thrombectomy devices were observed from the intimal to medial layers (figure 1). In the Solitaire 4 mm group, medial thickening and edematous changes were observed 1 week postoperatively. In the comparison between the Solitaire FR 4 mm and the control groups, the medial area was significantly greater in the Solitaire FR 4 mm group than in the control group (3.3×10−1±0.4×10−1 vs 2.7×10−1±0.3×10−1; p<0.05). Although intimal thickening was evident from 1 week postoperatively, a significant increase in intimal area was observed at the 2 week time point compared with 1 week (2.2×10−2±1.1×10−2 vs 0.4×10−2±0.2×10−2; p<0.05). No difference was observed in medial area between 1 and 2 weeks after the procedure (3.3×10−1±0.4×10−1 vs 3.2×10−1±0.3×10−1; p=0.46) (figure 2).
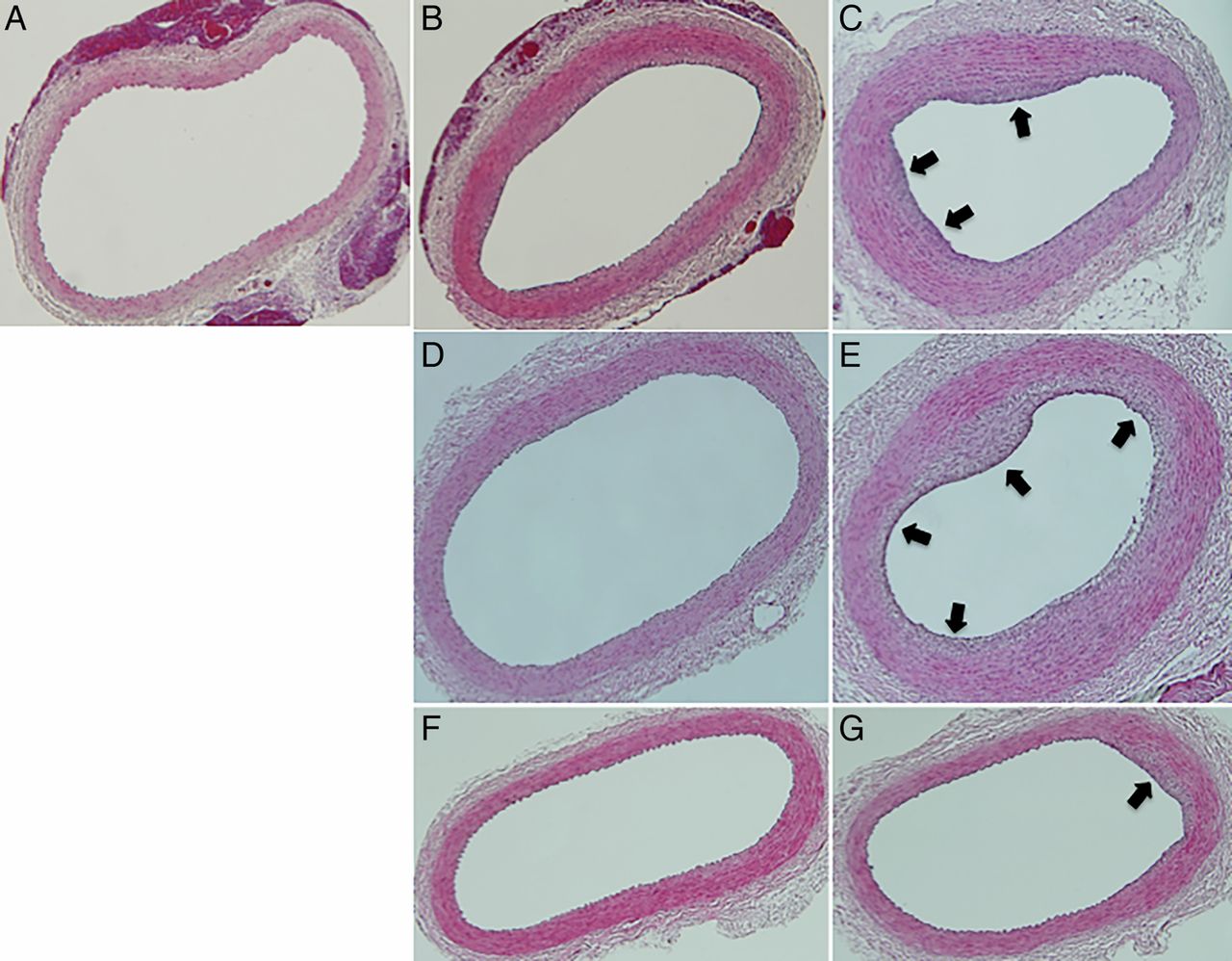
(A) Microscopic view of the left carotid artery (control sample) demonstrates a well maintained medial layer. (B) Microscopic view of the right carotid artery (Solitaire 4 mm sample, 1 week after the procedure) shows circumferential thickening of the medial layer. (C) Microscopic view of the right carotid artery (Solitaire 4 mm sample, 2 weeks after the procedure) shows focal thickening of the intimal layer (arrows). (D) Microscopic view of the left carotid artery (Solitaire 6 mm sample, 1 week after the procedure) shows circumferential thickening of the medial layer. (E) Microscopic view of the left carotid artery (Solitaire 6 mm sample, 2 weeks after the procedure) shows intimal layer thickening due to edema (arrows). (F) Microscopic view of the left carotid artery (Trevo sample, 1 week after the procedure) shows circumferential thickening of the medial layer. (G) Microscopic view of the left carotid artery (Trevo sample, 2 weeks after the procedure) shows intimal layer thickening due to edema (arrow). H&E staining, magnification ×20, for all samples.

Medial area (A) and intimal area (B) for the Solitaire 4 mm versus control samples. All values are expressed as means±SD. The p value was calculated using the Mann–Whitney test: *p<0.05.
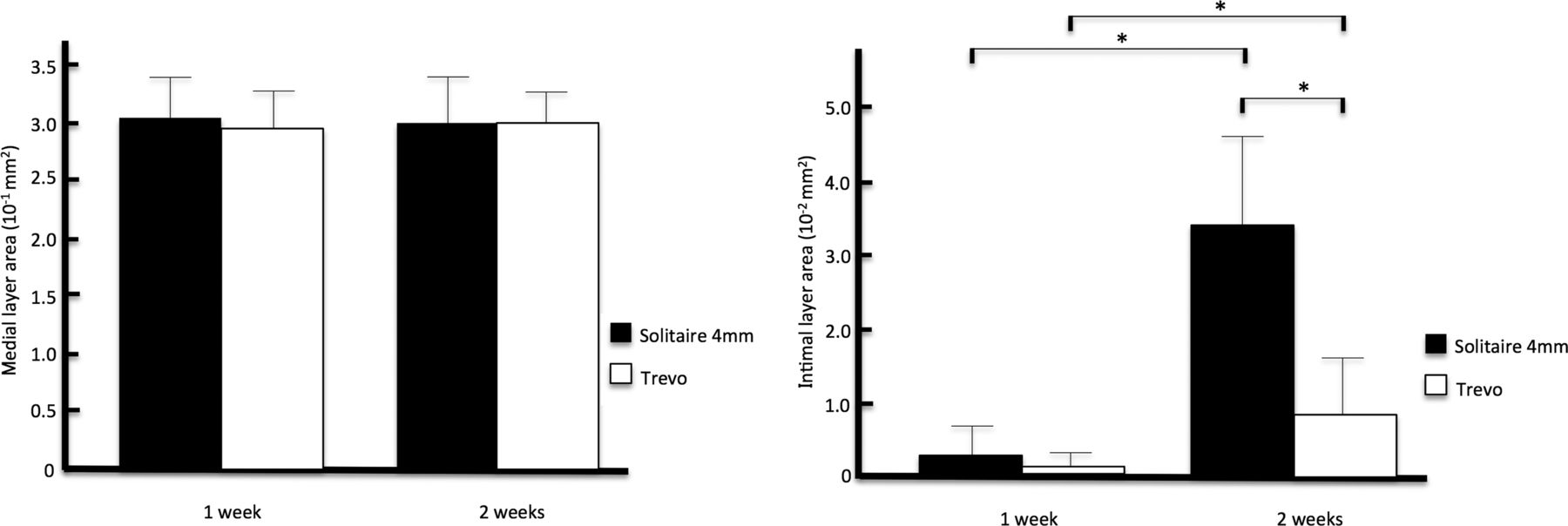
For between device comparisons, the Solitaire FR 4 mm and the Solitaire FR 6 mm were compared. With both the Solitaire FR 4 mm and the Trevo, intimal area was significantly greater at 2 weeks postoperatively than at 1 week postoperatively (0.09×10−2±0.2×10−2 vs 0.7×10−2±0.8×10−2, p<0.05; 0.2×10−2±0.3×10−2 vs 3.4×10−2±1.2×10−2, p<0.05); however, at 2 weeks, the intimal area was significantly larger with the Solitaire FR 4 mm (3.4×10−2±1.2×10−2 vs 0.7×10−2±0.8×10−2; p<0.05). There were no significant differences in medial area between the two devices at both the 1 and 2 week time points (3.0×10−1±0.3×10−1 vs 2.9×10−1±0.3×10−1, p=0.46; 3.0×10−1±0.4×10−1 vs 2.9×10−1±0.4×10−1; p=0.6) (figure 3).

Medial area (A) and intimal area (B) for the Solitaire 4 mm versus the Trevo samples. All values are expressed as means±SD. The p value was calculated using the Mann–Whitney test: *p<0.05.
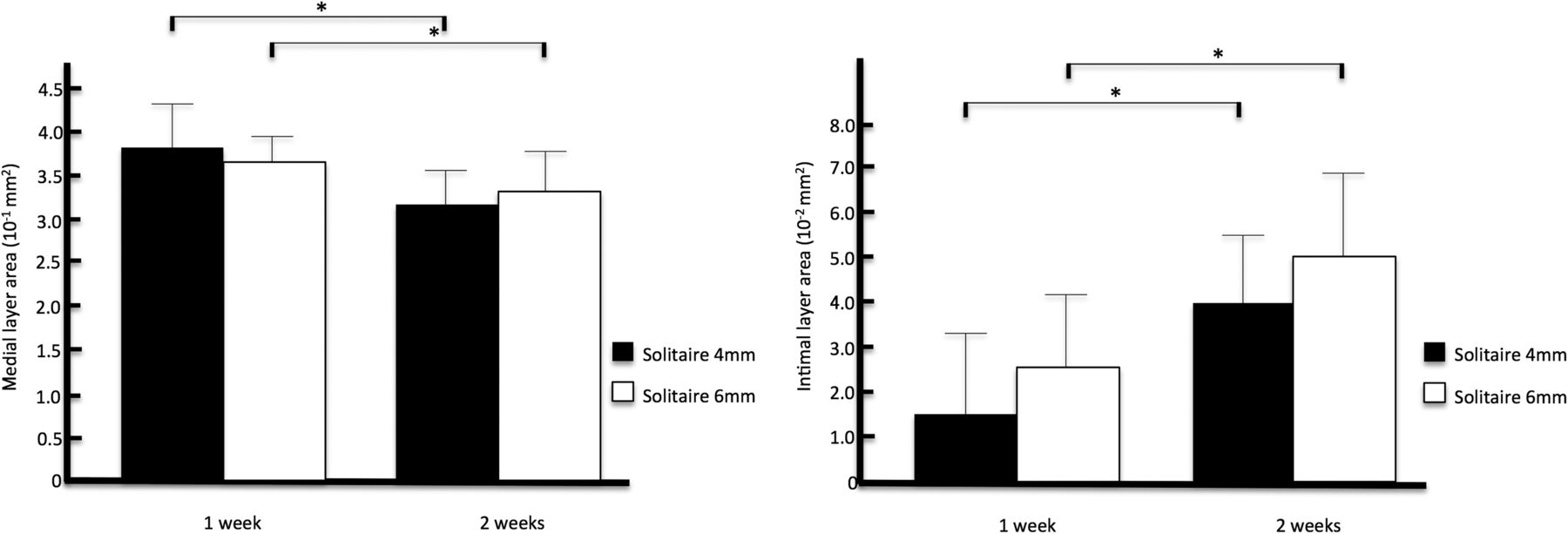
With the Solitaire FR 4 mm and the Solitaire FR 6 mm, intimal area increased significantly at 2 weeks compared with 1 week postoperatively (1.5×10−2±1.7×10−2 vs 4.0×10−2±1.4×10−2, p<0.05; 2.6×10−2±1.6×10−2 vs 5.1×10−2±1.6×10−2, p<0.05). However, there were no significant differences between the two devices at both the 1 and 2 week time points (1.5×10−2±1.7×10−2 vs 2.6×10−2±1.6×10−2, p=0.35; 4.0×10−2±1.4×10−2 vs 5.1×10−2±1.6×10−2, p=0.35) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Medial area (A) and intimal area (B) for the Solitaire 4 mm versus the Solitaire 6 mm samples. All values are expressed as means±SD. The p value was calculated using the Mann–Whitney test: *p<0.05.
In the comparisons between devices, no clear findings of disrupted internal elastic lamina or mural thrombus were observed. Intimal thickening was localized rather than appearing around the entire circumference, and it was not to the degree at which stenosis of the vessel lumen would occur.
Discussion
Mechanical thrombectomy has attracted attention as a firstline proven therapy for emergent large vessel occlusion, regardless of whether intravenous thrombolytics are given. In particular, stent retriever thrombectomy devices have been highly anticipated as effective treatment due to their high recanalization rates and favorable clinical outcomes.1 ,2 On the other hand, the effects on the vessel wall from intravascular maneuvers by the Merci retriever and Penumbra System have been reported in several autopsy cases.16 With the stent retriever thrombectomy device, it has also been a concern that vascular injuries could occur because the stent is pulled back in the expanded state; however, clinical studies have demonstrated that bleeding complications are not largely different between stent retrievers versus existing devices.1 ,2 On the other hand, Kurre et al11 reported a 26.0% occurrence of angiospasm due to stent retriever use, and Gascou et al17 pointed out that intracranial stenosis linked with a high mortality (50%) may be due to disruption of unstable plaque and irreversible damage to the vessel wall. Leishangthem and Satti18 reported vessel perforation during withdrawal of the Trevo.
Several animal studies have also shown angiographic changes in blood vessels following mechanical thrombectomy device use.19–21 In order to compare the extent of vascular damage induced by different mechanical thrombectomy devices (Merci retriever, Penumbra System, Solitaire Flow Restoration System, and Catch thromboembolectomy system), Gory et al22 not only examined angiographic changes, but they also performed histological comparisons, and found that all devices induced endothelial denudation as well as medial layer edema. Nogueira et al10 reported similar results with the Trevo. However, these changes were assessed during the acute phase, and how the condition progresses in the subacute to chronic phases was not evaluated.
The present experimental results with the Solitaire FR 4 mm showed that intimal and medial thickening was observed 1 week postoperatively, and that progression of intimal thickening was observed 2 weeks postoperatively. However, the thickening observed was not to the extent at which significant stenosis of the vessel lumen would occur. The morphological changes found were likely remodeling that occurred after the vascular endothelium was damaged when removing the stent, as sustained radial force is applied during this maneuver by the stent to the vascular wall.
Kurre et al11 retrospectively evaluated 265 vessels in 261 patients who were successfully recanalized using a mechanical thrombectomy device, and they found that vasospasm occurred in 26.0% and arterial dissection in 0.4% in the acute phase. Of the 116 patients who were available for follow-up, 0.9% developed vascular occlusion and 3.4% developed vascular stenosis. The authors postulated that endothelial damage occurred, albeit in a small number of vessels, due to the use of the device, and that this led to intimal thickening and then vascular occlusion or stenosis.11 In the present study, none of the animals showed significant stenosis of the vascular lumen; nonetheless, the present findings support the view that intimal thickening can occur due to endothelial damage after using stent retriever thrombectomy devices.
In the comparison between the Solitaire FR 4 mm and the Solitaire FR 6 mm, greater intimal thickening tended to occur with the 6 mm device, but the difference was not significant. In contrast, the area of intimal thickening was significantly smaller with the Trevo than with the Solitaire FR 4 mm. According to a previous study, although mild intimal thickening is observed with injury to the intimal layer alone, the extent of intimal thickening increases when intimal injury is accompanied by medial injury.23 This observation is consistent with reports that demonstrated that the proliferative capacity of smooth muscle cells increases when there is vascular injury that penetrates to the medial layer.24 Based on these reports, the extent of intimal thickening after vascular injury is dependent not only on intimal injury but also on the depth of injury, or specifically, the extent of injury to the vascular smooth muscle. Therefore, it is considered that the extent of intimal thickening becomes magnified with greater radial force of the stent.
The Solitaire FR is a stent with a closed cell design that was originally developed to assist in the embolization of aneurysms.25 Unlike other intracranial stents, this stent can be pulled into the microcatheter without detaching itself, even in the expanded state, and it has therefore become useful for thrombus retrieval in acute cerebral infarction.26 ,27 Given this, a new category of device, the stent retriever thrombectomy device, appeared. Since then, intensive development of new products has taken place at various manufacturing companies. Trevo is a wire mounted, non-detachable, laser cut stent that facilitates the process of capturing thrombus and has a unique strut form, cut surface, and radial force, such that the effects on the vascular walls are minimized; it has achieved favorable outcomes in a clinical study.2
Differences in intimal thickening between devices evaluated in the present study were thought to be due to differences in the structure of the stent. From the perspective of vascular injury, we believe the safety ranking of the devices are in the following order: Trevo>Solitaire FR 4 mm≥Solitaire FR 6 mm.
In the present study, rabbit carotid arteries were used to investigate vascular damage caused by stent retriever thrombectomy devices. The diameter of the rabbit carotid artery is approximately 2.0 mm, which is nearly equivalent to that of the M1 segment of the human middle cerebral artery. However, rabbit carotid arteries are less tortuous. Moreover, the experiment was performed and the stent was unfolded without an actual thrombus in the artery. For these reasons, the current results cannot be applied directly to clinical cases.
Although the present results do not necessarily indicate the superiority of either the Solitaire FR or Trevo, we believe the results are important in understanding the characteristics of stent retriever thrombectomy devices and in performing appropriate and safe treatments.
Conclusion
The present results showed that while there are some differences among devices, stent retriever thrombectomy devices can induce vascular injury to the medial layer. Compared with the Solitaire FR, the Trevo appeared to induce less vascular damage.
References
Footnotes
Contributors DA: planning, conduct, and reporting of the work described in the article. AI, HC, HI, and SM: reporting of the work described in the article.
Competing interests None declared.
Ethics approval All procedures were performed in accordance with international guidelines, and were approved by the ethics review board.
Provenance and peer review Not commissioned; externally peer reviewed.