Article Text

Abstract
Background Acute large vessel occlusion (LVO) can result from thromboemboli or underlying intracranial atherosclerotic disease (ICAD). Although the technique for revascularization differs significantly for these two lesions (simple thrombectomy for thromboemboli and balloon angioplasty and stenting for ICAD), the underlying etiology is often unknown in acute ischemic stroke (AIS).
Objective To evaluate whether procedural complications, revascularization rates, and functional outcomes differ among patients with LVO from ICAD or thromboembolism.
Methods A retrospective review of thrombectomy cases from 2008 to 2015 was carried out for cases of AIS due to underlying ICAD. Thirty-six patients were identified. A chart and imaging review was performed to determine revascularization rates, periprocedural complications, and functional outcomes. Patients with ICAD and acute LVO were compared with those with underlying thromboemboli.
Results Among patients with ICAD and LVO, mean National Institutes of Health Stroke Scale (NIHSS) score on admission was 12.9±8.5, revascularization (Thrombolysis In Cerebral Infarction, TICI ≥2b) was achieved in 22/34 (64.7%) patients, 11% had postprocedural intracerebral hemorrhage (PH2), and 14/33 (42.4%) had achieved a modified Rankin Scale (mRS) score of 0–2 at the 3-month follow-up. Compared with patients without underlying ICAD, there was no difference in NIHSS on presentation, or in the postprocedural complication rate. However, procedure times for ICAD were longer (98.5±59.8 vs 37.1±34.2 min), there was significant difference in successful revascularization rate between the groups (p=0.001), and a trend towards difference in functional outcome at 3 months (p=0.07).
Conclusions Despite AIS with underlying ICAD requiring a more complex, technically demanding recanalization strategy than traditional thromboembolic AIS, it appears safe, and good outcomes are obtainable.
- Angioplasty
- Atherosclerosis
- Balloon
- Stroke
- Thrombectomy
Statistics from Altmetric.com
Introduction
Atherosclerotic intracranial arterial disease (ICAD) is one of the most common causes of stroke worldwide1 ,2 ,3–5 and is associated with a high risk of recurrent stroke. Multiple studies have evaluated the significance of ICAD as a cause of acute and recurrent stroke,6–8 but few studies have investigated its importance in patients with acute ischemic stroke (AIS) receiving emergent endovascular therapy for large vessel occlusion (LVO).9
Unlike patients with ICAD presenting with a transient ischemic attack (TIA) and stroke beyond 6 hours, the optimal treatment of AIS with underlying ICAD in LVO remains unclear. ICAD can be an occult cause of refractory occlusion following mechanical thrombectomy. Several case series10–14 and one prospective trial evaluated the use of angioplasty in patients with AIS, demonstrating that angioplasty with or without stenting is safe and yields a high rate of revascularization and favorable outcome.9 However, that trial was performed in Asia which limits its applicability to the Western hemisphere, as outcomes of ICAD in people with TIA and ischemic stroke have been shown to be different between Asian and Western countries.15 ,16 Thus, further analysis of acute endovascular intervention in patients with ICAD with AIS in the USA population may be of benefit.
Patients and methods
Patient population
The institutional review board approved this retrospective study. A total of 36 consecutive patients who presented to a comprehensive stroke center with AIS between August 2008 and March 2015 and were treated with mechanical thrombectomy and found to have underlying ICAD, requiring treatment with angioplasty with or without stenting, were included. ICAD was defined as significant fixed focal stenosis at the occlusion site that became evident during the thrombectomy procedure or on final angiography.
Thrombectomy protocol
All patients were evaluated by a stroke neurologist. Initial evaluation included non-contrasted CT of the brain and CT angiography and perfusion imaging. All eligible patients received IV tissue plasminogen activator. Candidacy for thrombectomy was determined by CT perfusion irrespective of time of onset. Mechanical thrombectomy was performed using different approved modalities, including aspiration with separators, stent retrievers, and aspiration thrombectomy. Intracranial angioplasty was performed following the initial diagnostic angiography or during the initial thrombectomy attempt if an ICAD lesion was apparent. A stent was used when the lesion was refractory to balloon angioplasty. Stent and balloon size were usually undersized by 10–20% or sized to vessel caliber. All patients undergoing stent placement were loaded with abciximab intraprocedurally then received aspirin and clopidogrel after the procedure. All patients underwent routine brain imaging (CT or MRI) 24 hours after the procedure.
Procedural complication and functional endpoints
Details of the location of the occlusion, use of stent, type of stent, and procedure complications, including post-treatment intracerebral hemorrhage (ICH), were collected. Revascularization was assessed using the Thrombolysis In Cerebral Infarction (TICI)17 ,18 scale by a blinded reviewer. Significant ICH was defined as PH2 with CT-based classification of the European Cooperative Acute Stroke Study.19 ,20 Functional outcome was assessed by modified Rankin Scale (mRS) at 3 months after discharge.
Postprocedural complications and functional outcomes were compared between patients with underlying ICAD and those with non-ICAD (thrombosis only) who underwent thrombectomy with the ADAPT (A Direct Aspiration first-Pass Thrombectomy) technique.21–23 A total of 184 patients with AIS due to thromboembolism who received thrombectomy alone (no balloon angioplasty or stenting) were evaluated and compared with the ICAD group.
Statistical analysis
Descriptive statistics are presented as mean±SD and N (%), and differences between the neurointerventional groups were tested using a two-sample t-test and χ2 test for continuous and categorical data, respectively. To assess the relationships between ICAD, linear and logistic multivariable models were used. All tests were performed using SAS V.9.4 (c). Statistical significance was assessed at α=0.05.
Results
Patient characteristics
Between August 2008 and August 2015, 435 patients received thrombectomy, of whom 36 (8.3%) were found to have underlying ICAD during the thrombectomy procedure. Preoperative metrics and outcome are presented in tables 1 and 2. Twenty-four were male (67%) and the mean age was 63.5±13.7 years. Twenty-four (66.7%) ischemic strokes occurred in the anterior circulation and 12 (33%) in the posterior circulation. Of the patients with ICAD, 89% had hypertension, 92% had hyperlipidemia (defined by low-density lipoprotein >70 mg/dL), 42% had diabetes mellitus (DM), and 38% had coronary artery disease.
Baseline characteristics in treatment groups
Summary of the site of occlusion and outcomes among patients with a large vessel occlusion from intracranial atherosclerotic disease (ICAD)
Patients presented with a mean National Institutes of Health Stroke Scale (NIHSS) score of 12.9±8.5 (range 1–33). The Alberta Stroke Program Early CT Score (ASPECTS) score was ≥6 in 23/24 patients with anterior circulation strokes, and one had an ASPECTS of 4 but with significant mismatch in addition to the core infarct. Underlying ICAD was most frequently seen in the internal carotid artery (16/36) with the most common location being the supraclinoid segment (8/16). The second most common location was the middle cerebral artery (8/36), most occurring at the distal M1 segment (7/8). The third most common location was the basilar artery (9/36), with most occurring at the level of the proximal basilar artery (5/9). One patient had a posterior cerebral artery occlusion and two had vertebral artery occlusions (figures 1⇓–3).
Illustrative case of an elderly patient who presented with aphasia and right hemiparesis (National Institutes of Health Stroke Scale (NIHSS) score 8) with left M1 occlusion (A). Thrombolysis In Cerebral Infarction (TICI) 3 revascularization was obtained after A Direct Aspiration first-Pass Thrombectomy (ADAPT) followed by angioplasty and stenting with a wingspan stent (B). The 90-day modified Rankin Scale (mRS) score was 1.
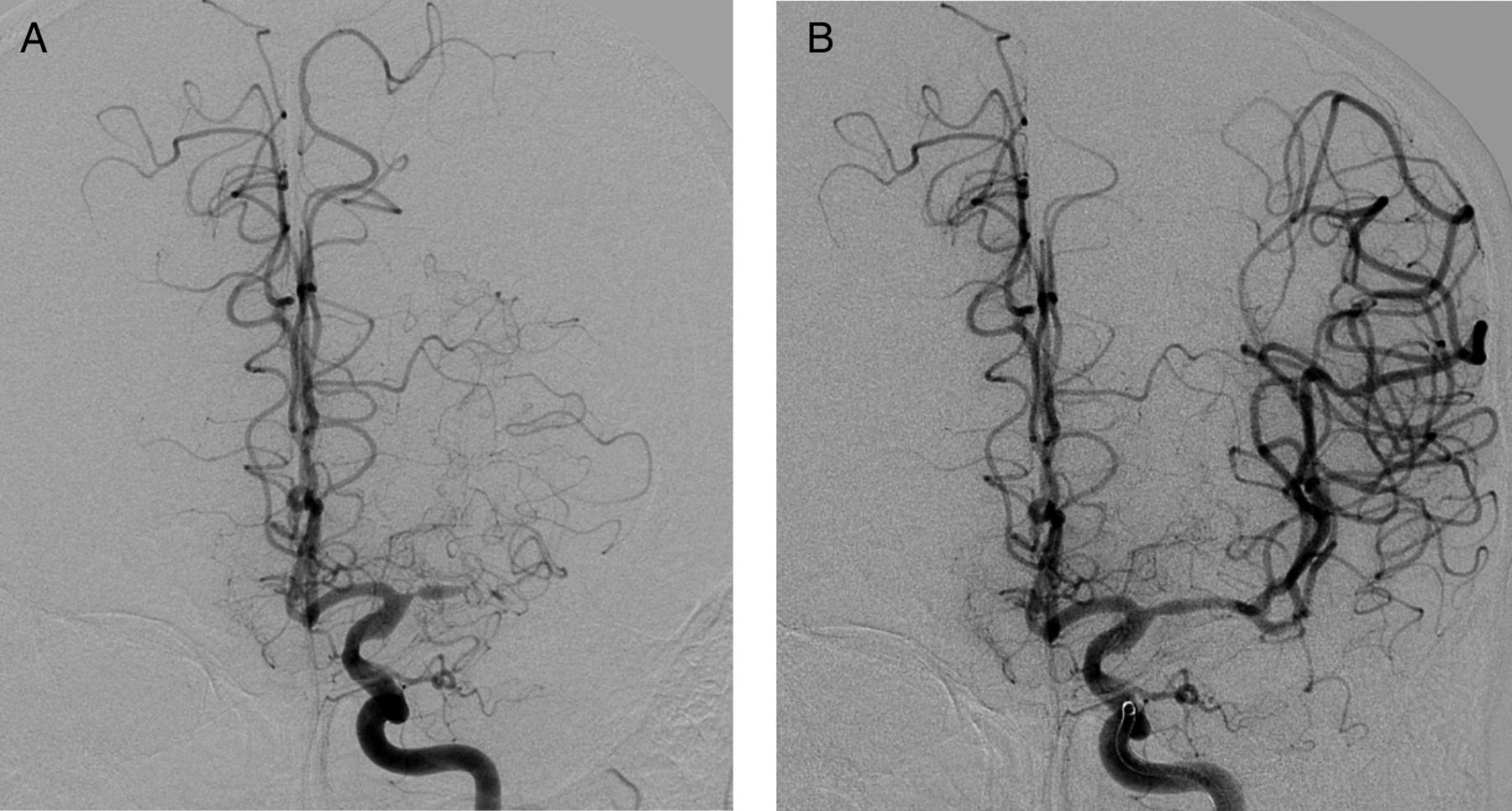
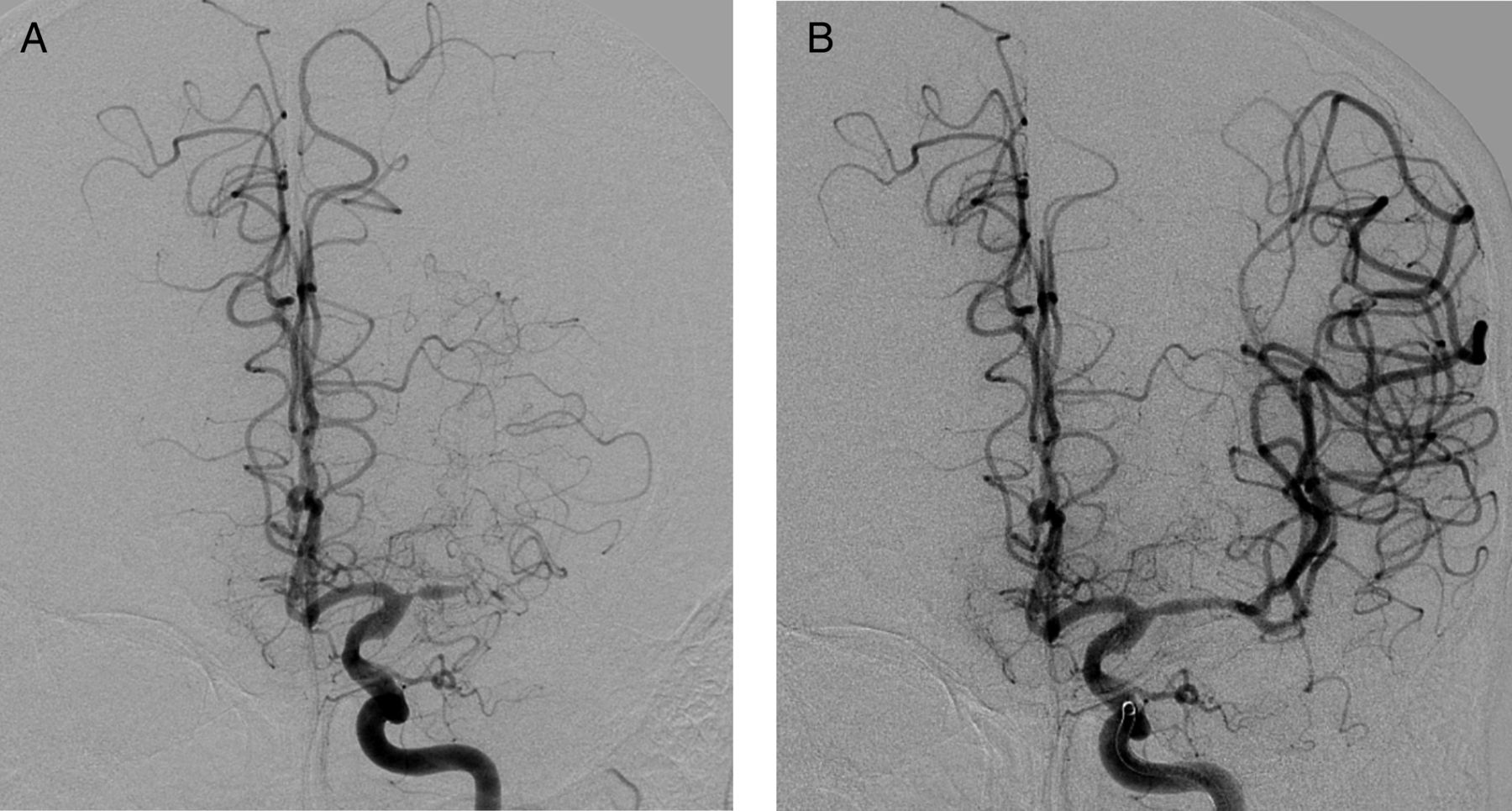
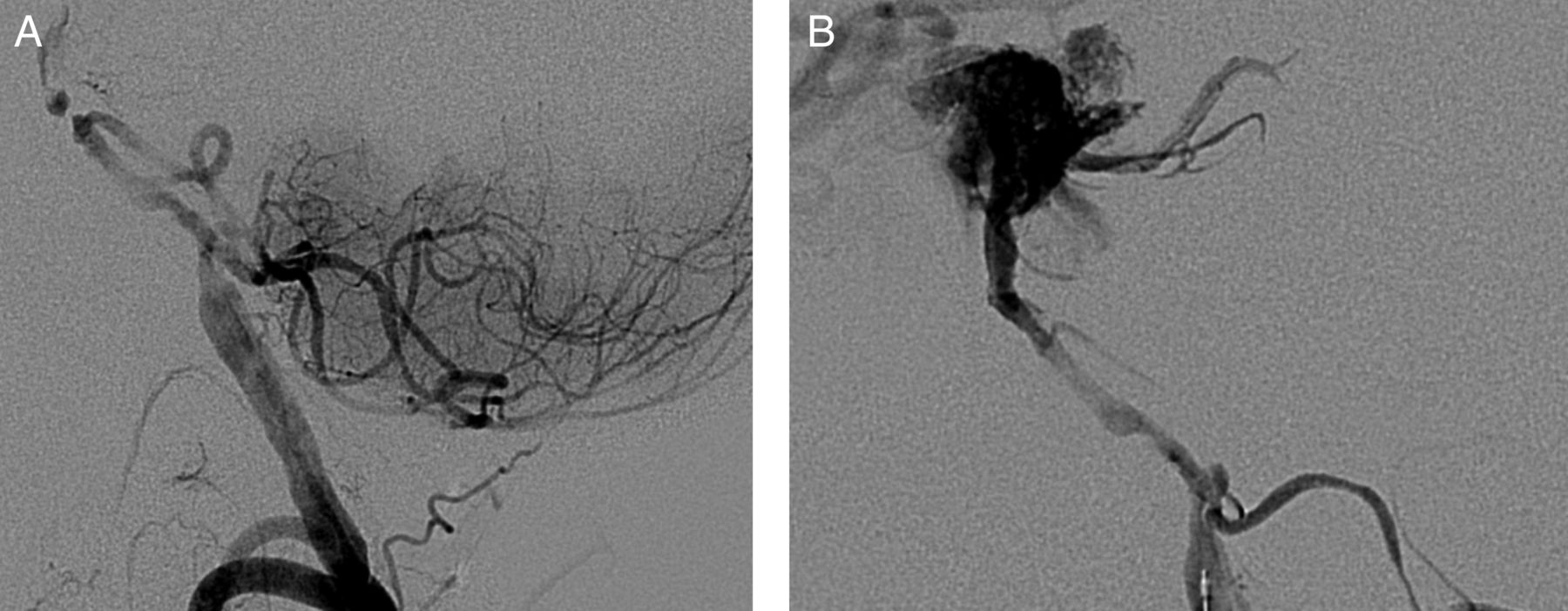
An elderly patient who presented with acute basilar artery occlusion and National Institutes of Health Stroke Scale (NIHSS) score 17 (A). The patient received A Direct Aspiration first-Pass Thrombectomy (ADAPT), angioplasty, and wingspan stent placement with Thrombolysis In Cerebral Infarction (TICI) 3 revascularization (B) and achieved a modified Rankin Scale (mRS) of 0 at 90 days.

{kind=link}
{kind=link}
{kind=link}
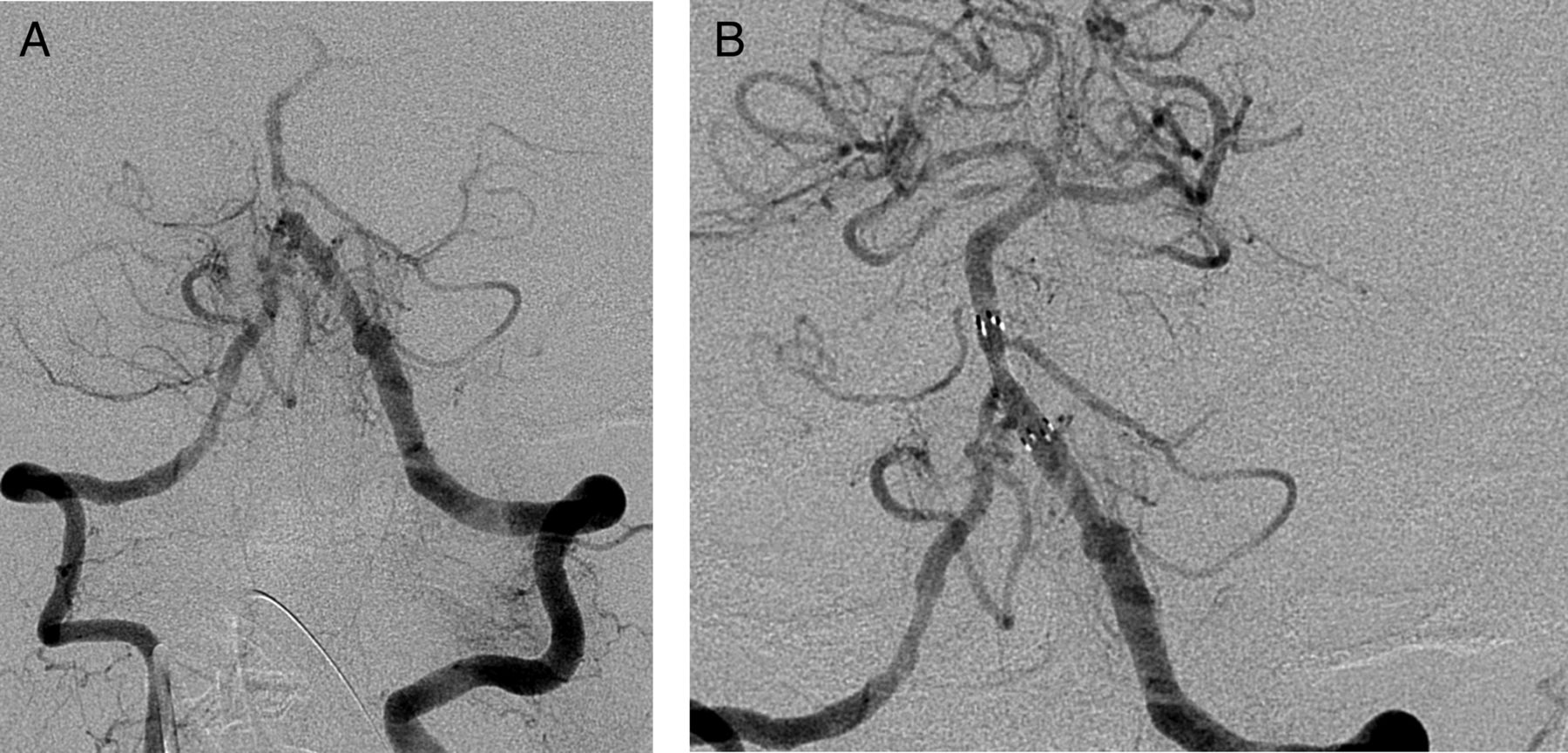
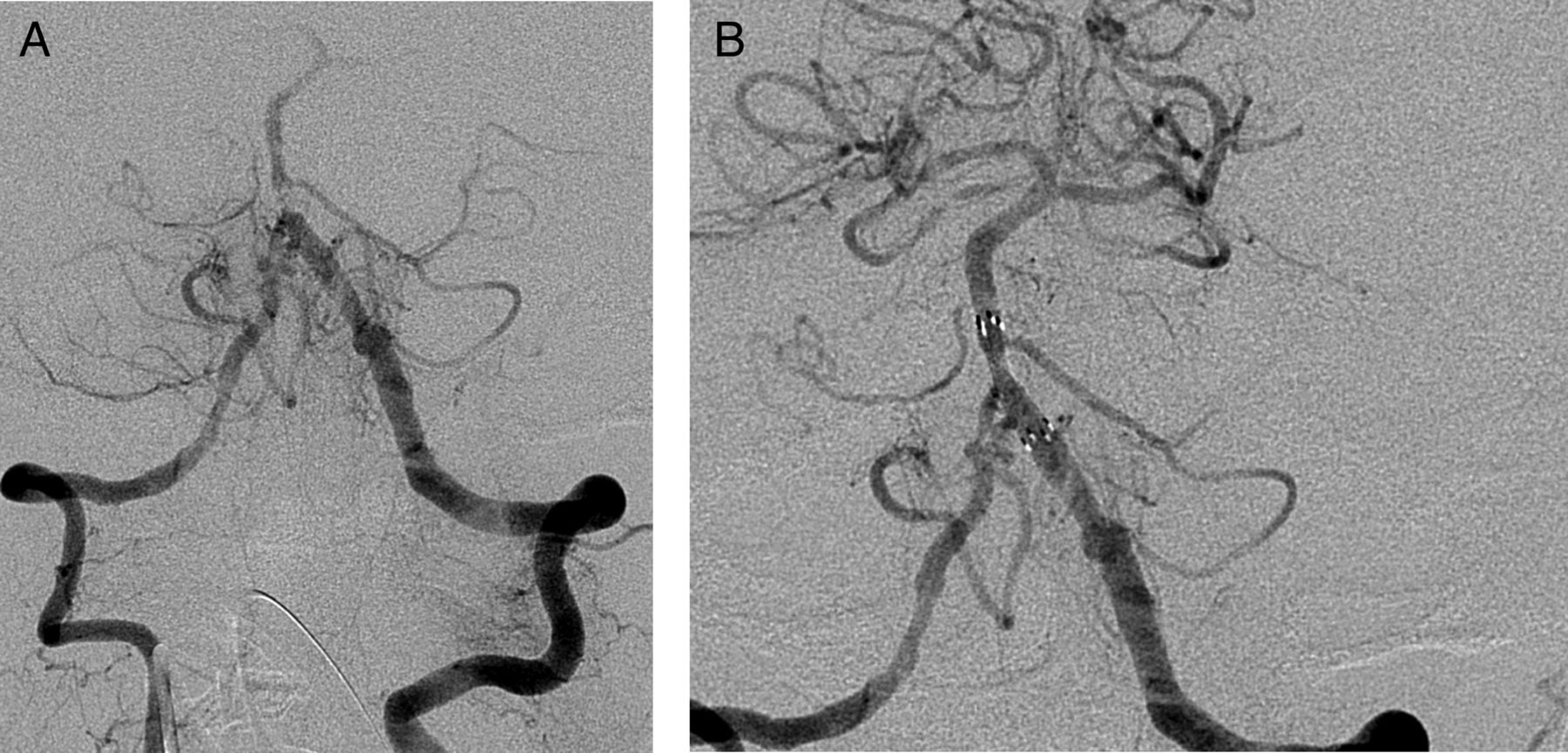
An elderly patient who presented with acute basilar artery occlusion and National Institutes of Health Stroke Scale (NIHSS) score 13. (A) Thrombectomy was complicated by rupture of the basilar artery and catastrophic neurological injury (B). The patient's family withdrew care.
Procedural details
Ninety-four per cent (34/36) of patients received non-compliant balloon angioplasty and 89% (32/36) required stenting. The Wingspan stent (Stryker Neurovascular, Fremont, CA, USA) was used in all but two cases where precise and enterprise stents were used. Successful revascularization (TICI≥2b) was achieved in 64.7% (22/34) of patients.
Complications and outcomes
Four patients had postprocedural PH2 ICH, three of whom died during their hospitalization. In-hospital mortality was 22% (n=8). Favorable mRS (0–2) at 3 months was found in 14/33 patients (42%) while 19/33 patients had mRS (3–6) at 3 months. Three patients were lost to follow-up.
Comparison of revascularization experience: ICAD versus thromboemboli
Baseline characteristics of patients with LVO due to underlying ICAD were compared with patients with LVO due to thromboemboli (table 1). There was no difference in the presenting age, gender, or race between treatment groups. Patients with underlying ICAD had a higher rate of hypertension (p≤0.001), and diabetes mellitus (p=0.004).
Presenting NIHSS scores and rates of postprocedural ICH were similar in patients with LVO from underlying thromboemboli and in those with ICAD (table 3). However, the thromboemboli patients had a significantly higher rate of TICI ≥2b (95.3%) revascularization than the patients with ICAD (64.7%; p=0.001). There was a trend (p=0.07) towards improved outcome at 90 days among thrombosis only patients. Mean procedure time (groin access to final revascularization time) in the ICAD group was significantly longer than in the thromboemboli group (98.5±59.8 vs 37.1±34.2 min, p<0.001).
Comparison of symptom severity on presentation, recanalization rates, postprocedural bleeding rates, and functional outcome at 3 months
Discussion
The main finding of this report is that emergent intracranial angioplasty with or without stenting is safe and has a good functional outcome in patients with AIS and underlying ICAD. While the procedure is more complex and more time consuming, with a lower revascularization rate, the postprocedural ICH rate, and functional outcome is comparable to that of patients with LVO due to thromboemboli receiving endovascular revascularization.
Intracranial atherosclerosis is more prevalent in the Eastern than in the Western hemisphere, and most large-scale studies investigating ICAD in stroke have included Asian populations. Studies in Western countries have shown that aggressive medical management is better than the use of a Wingspan stent among patients with severe (70–99%) symptomatic intracranial atherosclerotic disease causing a stroke or TIA within 30 days of presentation.15 ,24 The negative results in the Stenting and Aggressive Medical Management for the Prevention of Recurrent Ischemic Stroke (SAMMPRIS) trial were primarily associated with a higher than expected periprocedural stroke rate in the stenting group and improvements in medical management and lifestyle factor modifications. On the other hand, studies in the Eastern hemisphere suggest that stenting for symptomatic ICAD is safe with lower rate of periprocedural complications16 ,25 and may be better than medical management. The stark differences probably reflect genetic, socioeconomic, and dietary differences between the populations in the two hemispheres, which alter their natural histories.
Many studies have evaluated emergent stenting of extracranial internal carotid artery occlusion in AIS and shown that the procedure is safe, with a low ICH rate, and yields a high revascularization rate, and good functional outcome, these results are similar in the Eastern and Western hemispheres.6 ,26
Studies examining emergent intracranial angioplasty with or without stenting showed that the procedure is safe, with favorable outcome in patients with AIS and underlying ICAD.9 However, similar studies have not been done in the USA.
While SAMMPRIS enrolled patients with severe ICAD and a TIA or stroke within 30 days of symptom onset, the patients in our study presented with an acute LVO. Since the results of the SAMMPRIS study, and the relatively rare incidence of LVO due to ICAD, there has not been a drive to improve the technology involved, requiring many steps to complete and having to cross the lesion many times. On the other hand, techniques and catheters for thrombectomy have evolved dramatically over the same period, yielding faster and more streamlined procedures.27 For this reason, we chose to compare our results for ICAD with LVO (constant over time) with our results using the ADAPT technique (most recent and most effective thrombectomy iteration). Our findings demonstrate that there is no difference in stroke severity on presentation between patients with AIS with underlying ICAD and those with thromboemboli. Importantly, rates of postprocedural ICH are also the same, indicating that angioplasty and stenting an LVO in the AIS setting is safe even though the procedure is more involved and dual antiplatelet therapy is required. The more technically demanding nature of the revascularization for ICAD is reflected in the significantly longer procedure times (nearly three times longer than for thrombectomy alone) and lower rate of TICI ≥2b recanalization. However, the outcomes among patients with ICAD are comparable to recanalization in thrombus alone and certainly more favorable than the natural history of an LVO.
Study limitations
The limitations of our study are largely due to its retrospective nature. In addition, we compared patients who received endovascular revascularization using ADAPT technique between 2012 and 2015 with patients with ICAD receiving emergent endovascular revascularization between 2008 and 2015.
Conclusion
Despite the complexity of treating AIS with underlying ICAD in the setting of an LVO, these procedures are safe and the outcomes are comparable to recanalization in thrombus alone. Patients with AIS and underlying ICAD should continue to be considered candidates for thrombectomy.
Acknowledgments
Alyssa Pierce assisted with the editing and revision of this manuscript.
References
Footnotes
Contributors Each author listed above should receive authorship credit based on the material contribution to this article, their revision of this article, and their final approval of this article for submission to this journal.
Competing interests AMS: Penumbra—consulting, honorarium, speaker bureau; Pulsar Vascular—consulting, honorarium, speaker bureau; Microvention—consulting, honorarium, speaker bureau, research; Stryker—consulting, honorarium, speaker bureau. AST, RDT, and MIC: Codman—consulting, honorarium, speaker bureau, research funding; Covidien—consulting, honorarium, speaker bureau; Penumbra—consulting, honorarium, speaker bureau, research grants; Microvention—consulting, honorarium, speaker bureau, research grants; Blockade—stock, consulting, honorarium, speaker bureau; Pulsar Vascular—stock, consulting, honorarium, speaker bureau, research; Medtronic—consulting, honorarium, speaker bureau.
Ethics approval Medical University of South Carolina institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.