Article Text

Abstract
Background Vascular remodeling in response to implantation of a tissue engineering scaffold such as a flow diverter (FD) leads to the cure of intracranial aneurysms. We hypothesize that the vascular response is dependent on FD design, and CD34+ progenitor cells play an important role in the endothelialization of the implant.
Methods Sixteen rabbit aneurysms were randomly treated with two different single-layer braided FDs made of cobalt–chrome alloys. The FD-48 and FD-72 devices had 48 and 72 wires, respectively. Aneurysm occlusion rate was assessed during the final digital subtraction angiogram at 10, 20, 30, and 60 days (n=2 per device per time point). Implanted vessels were analyzed with scanning electron microscopy for tissue coverage, endothelialization, and immuno-gold labeling for CD34+ cells.
Results Complete aneurysm occlusion rates were similar between the devices; however, complete or near complete occlusion was more frequently observed in aneurysms with neck ≤4.2 mm (p=0.008). Total tissue coverage at 10 days over the surface of the FD-48 and FD-72 devices was 56.4±11.6% and 76.6±3.6%, respectively. Endothelial cell growth over the surface was time-dependent for the FD-72 device (Spearman's r=0.86, p=0.013) but not for the FD-48 device (Spearman's r=−0.59, p=0.094). The endothelialization score was marginally correlated with the distance from the aneurysm neck for the FD-48 device (Spearman's r=1, p=0.083) but not for the FD-72 device (Spearman's r=0.8, p=0.33). CD34+ cells were present along the entirety of both devices at all time points.
Conclusions This study gives preliminary evidence that temporal and spatial endothelialization is dependent on FD design. Circulating CD34+ progenitor cells contribute to endothelialization throughout the healing process.
- Aneurysm
- Flow Diverter
Statistics from Altmetric.com
Introduction
There has been a paradigm shift over the past decade to reconstruct the diseased parent vessel harboring an intracranial aneurysm using flow diversion.1–6 Although coil embolization often offers prompt aneurysm occlusion, which is desirable especially in ruptured cases, large (10–25 mm) and giant (>25 mm) coiled aneurysms have recurrence rates of 35–50% and 60–85%, respectively.7 In contradistinction, high rates of complete aneurysm occlusion have been reported using flow diverter (FD) implants that lead to parent vessel reconstruction and intrasaccular aneurysm thrombosis. Progressive aneurysm thrombosis plays a critical role in the healing process; however, the newly formed endothelial coverage over the implant has a pivotal impact on permanent exclusion of the aneurysm from the circulation. The ongoing tissue engineering is partially influenced by hemodynamics due to modification of the local flow conditions; however, the structural properties and surface characteristics of the FDs may play a critical role in directing cellular differentiation, proliferation, and attachment onto the device.8 Engineering design of current FDs typically involves braiding metal alloys into high density (∼70% porosity) meshes with various wire diameters, pore densities, and braid angles.9 How these engineering parameters of the tissue engineering substrate alter the impact of parent vessel reconstruction remains unknown.
The need to understand and promote the endothelialization process has clinical significance. After the FD treatment during the vascular remodeling process, for an unknown time period, or latency, the aneurysms are not fully protected from rupture. A meta-analysis has recently shown that subarachnoid hemorrhage occurred in 3% in the first 30 days after treatment, mostly in large and giant aneurysms with a posterior circulation predominance (OR 1.89, 95% CI 0.43 to 8.21).10 Angiographically confirmed aneurysm occlusion is not necessarily conclusive evidence that parent artery reconstruction is complete, as evidenced on MRI studies that have shown persistent aneurysm size despite angiographic cure11 and autopsy studies that show incomplete neointimal growth along the surface of the device.12 Further confounding clinical management is the uncertainty regarding the duration of dual antiplatelet therapy (DAT). If the DAT is suspended prior to complete endothelialization of the FD, it might result in late thromboembolic complications such as in-stent thrombosis or distal embolism leading to ischemic stroke.13 On the other hand, prolonging administration of antiplatelet inhibitors may augment the risk of hemorrhage. According to recently published studies, distal intraparenchymal hemorrhage was revealed behind new symptoms in about 2.5% of the cases, days or weeks after the procedure.4 ,14 ,15 The other consequence of impaired/delayed endothelialization along with insufficient aneurysm thrombosis is that, at 6 months and at 1 year after treatment, 27% and 15%, respectively, of the aneurysms are still not fully occluded.3
We hypothesized that endothelialization and the consequently earlier aneurysm occlusion is determined by FD design as a tissue engineering scaffold, such as consistent low-porosity and uniformly high pore density at the neck of the aneurysm. Furthermore, we evaluated whether circulating CD34+ progenitor cells (CD34+ PCs) contribute to the FD endothelialization process. Answering these questions could support a new therapeutic approach by using optimally designed endoluminal scaffolds to facilitate the recruitment of PCs and to accelerate the endothelialization process, which may aid in avoiding late complications and at the same time achieving earlier complete aneurysm occlusion.
Materials and methods
Sixteen New Zealand White rabbits (female, weight range 3.5–5.5 kg) with elastase-induced aneurysms16 were used in accordance with an approved protocol by our university's Institutional Animal Care and Use Committee. All procedures were performed under general anesthesia and using strict aseptic technique. Prior to all surgical or imaging procedures, the animals were pre-anesthetized by a subcuticular injection of atropine (0.01 mg/kg). Anesthesia was induced by an intramuscular injection of ketamine (35 mg/kg) and xylazine (5 mg/kg) and maintained with mechanical ventilation of 1–3% isoflurane. The physiologic status of the animal was assessed using continuous monitoring of the respiration rate, heart rate, oxygen saturation level, end-tidal CO2 level, and temperature.
Device implantation
Prior to device implantation, 16 aneurysms were imaged non-invasively and paired based on dimensions and morphology. In each paired block, animals were randomly assigned to one of two different types of single-layer braided FDs made of cobalt–chrome alloys. The FD-48 device was manufactured using 48 wires with a 33 μm diameter and 145° braid angle. The FD-72 device had 72 wires with a 32 μm diameter and 115° braid angle. Each device had interwoven platinum wires for radio-opacity. Two paired blocks of animals (n=4) were randomly assigned to terminal follow-up angiography at 10, 20, 30, and 60 days.
Five days prior to device implantation and until the designated end point the rabbits were placed on DAT (aspirin 1 mg/kg and clopidogrel 10 mg/kg once daily) and during the implant procedure were anticoagulated with heparin (100 mg/kg). After implantation, control angiography was performed to assess successful placement of the device covering the aneurysm neck and apposition. If the device was poorly apposed, angioplasty was performed (Hyperform 4 mm×10 mm, Medtronic Neurovascular, Irvine, California, USA).
Sacrifice, tissue harvest, and scanning electron microscope analysis
Blood samples were collected at the final imaging procedure to record the level of antiplatelet drug effectiveness (aspirin reaction units (ARU) and P2Y12 reaction units (PRU); VerifyNow, Accumetrics, San Diego, California, USA). Follow-up digital subtraction angiography (DSA) was performed under general anesthesia through left femoral artery access. Acquired DSA and VasoCT17 images were analyzed and stored. The aneurysm occlusion rate was graded using a scale of 0–4 where a score of 0 indicated no change, 1 indicated volume reduction of ≤50%, 2 indicated volume reduction of >50%, 3 indicated aneurysm filling was confined to the neck, and 4 indicated complete occlusion.18 Following the final angiography procedure, IV heparin (500 U/kg) was administered prior to euthanasia by an overdose of sodium pentobarbital (150 mg/kg). Transcardiac perfusion fixation was performed using heparinized saline (5000 U/L) followed by 4% paraformaldehyde under physiological pressure. The subclavian and innominate arteries were explanted and a suture was placed at the distal aspect of the artery for identification.
The parent vessels were cut longitudinally into two parts to expose the luminal surface, with one half being processed for conventional scanning electron microscopy (SEM) (see online supplementary material) and the remaining half processed for immuno-SEM (see online supplementary material). Conventional SEM was used to determine the degree of endothelial coverage. Immuno-gold labeling was applied in order to identify CD34+ PCs on the surface of the FD to determine the rate of stem cell recruitment during the healing process. Primary biotinylated CD34+ antibodies (Biorbyt, San Francisco, California, USA) were used in conjunction with streptavidin gold conjugated nanoparticles (60 nm) for indirect immunolabeling (Cytodiagnostics, Burlington, Ontario, Canada). The immuno-gold SEM technique was applied to both negative and positive controls (see online supplementary methods).
supplementary data
For accurate and reproducible scanning, a grid was created and centered on the aneurysm neck for semi-quantitation of CD34+ PCs. Data were collected from 1, 2, 5, and 10 mm from the center of the aneurysm neck and studied at a very high magnification (up to 12 000×). At each location, cells were scored as follows: 0=no CD34+ PCs; 1=<5 immuno-gold positive PCs; 2=>5 immuno-gold positive PCs. A quantitative evaluation of the percentage coverage of the luminal basement membrane and endothelialization was assessed with Image-J software (National Institutes of Health, USA). To quantify the advancement of ongoing tissue remodeling, a grid overlay with 40 µm×40 µm spacing was applied at the neck of the aneurysm and distally at 3, 6, and 9 mm to identify and count the endothelial cells. The percentage of the endothelial cells was characterized by three different morphological appearances and transformed to a 0–5 scoring system where a score of 0 was given if no endothelial cells were present and a score of 5 if a completely mature endothelial layer covered the surface (for details see online supplementary methods).
Results
There were no differences in the baseline characteristics (eg, aneurysm height, neck size, parent vessel diameter) between the two groups (p>0.1, table 1). The PRU values were therapeutic in all cases (mean 94±36, range 36–174) and not different between the device groups (p=0.16). In all 16 cases, appropriate FD deployment was recorded, covering the entire aneurysm neck. There was no vessel perforation, parent vessel dissection, or thromboembolic complication. DSA and VasoCT revealed incomplete vessel wall apposition in seven cases (43%) following FD deployment; after angioplasty complete apposition was seen in four of the seven cases and improvement in the remaining three cases. There was no significant difference in aneurysm occlusion rates at follow-up between the two devices (p>0.1), with a median of 2 in both groups. However, complete or near complete occlusion was more frequently observed in aneurysms with neck ≤4.2 mm (p=0.008) in both groups. A total of 46 branches were covered with an FD and all were patent on the follow-up DSAs (mean diameter of covered vessel was 2.4 mm for the vertebral artery and ranged between 1.2 and 1.5 mm for the internal thoracic and cervical arteries). There was no in-stent thrombosis or stenosis (defined as vessel lumen narrowing of ≥10%) on the DSA or VasoCT.
Baseline aneurysm characteristics
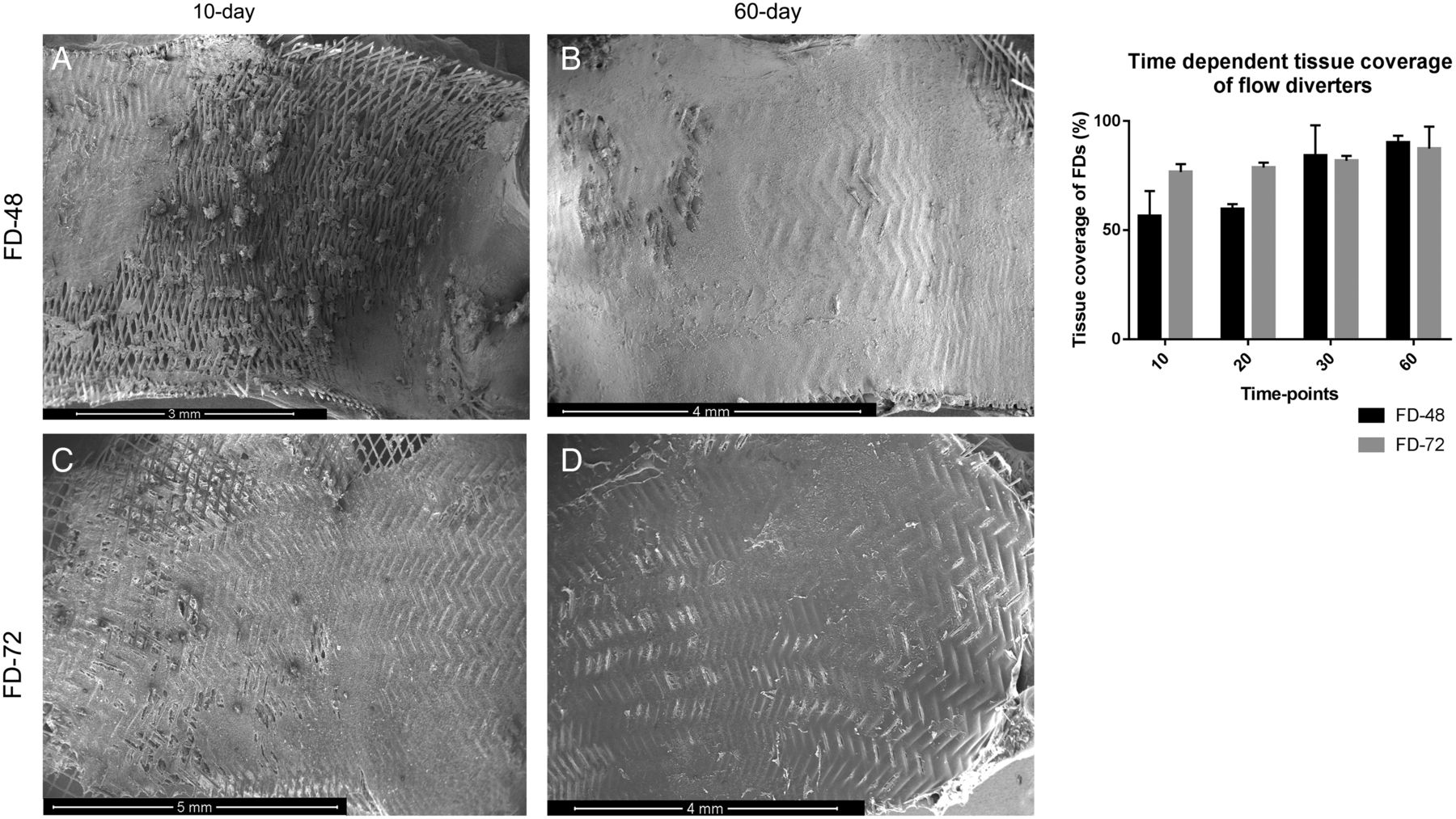
Total tissue coverage (including both endothelium and basement membrane) over the surface of the FD-48 and FD-72 devices was 72±17.4% and 76.9±13.5%, respectively (p>0.05). At the earliest time point (10 days) the FD-48 device was less covered than the FD-72 device (56.4% vs 76.6%; figure 1). However, at the later time points this difference was diminished (90.2% and 87.4% at 60 days for the FD-48 and FD-72 devices, respectively).

Time-dependent tissue coverage patterns over the inner surface of flow diverters (FDs). Tissue coverage of the FDs reveals different patterns at the 10-day time point (A and C) but not at the 60-day time point (B, D and graph). (A) shows multiple micro-clot formations mostly located over the intersections of the struts of the FD-48 device and distal to that partially covered segment. In (C) the surface of the FD-72 device is more evenly covered with a thin layer of tissue.
CD34+ PCs were present on both devices at the center of the aneurysm neck and along the entirety of the devices at all time points (figure 2). The median score for PCs ranged from 1 to 2 for both devices across the evaluated regions.
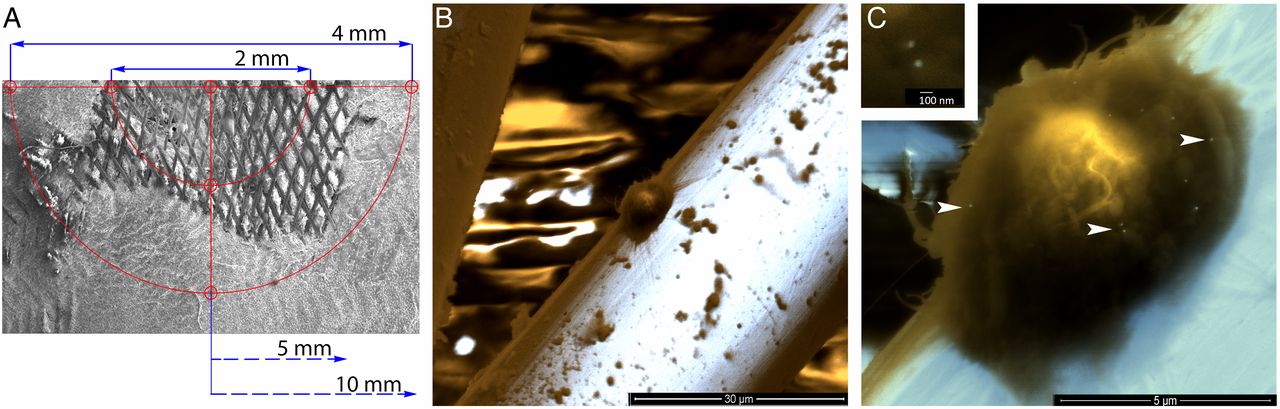
Representative case: scanning electron microscopy (SEM) images with immuno-gold labeling 10 days after implantation of the flow diverter (FD)-72 device. (A) SEM map used as guidance for identifying CD34+ progenitor cells. (B) A progenitor cell is found attached to the strut of the FD 2 mm distal to the aneurysm neck. (C) The same cell as in (B) showing bright spots on the cell surface corresponding to CD-34 antigen and 60 nm gold particle conjugate (white arrowheads). Area of interest digitally zoomed in the left upper corner for better visualization of the gold nanoparticles.
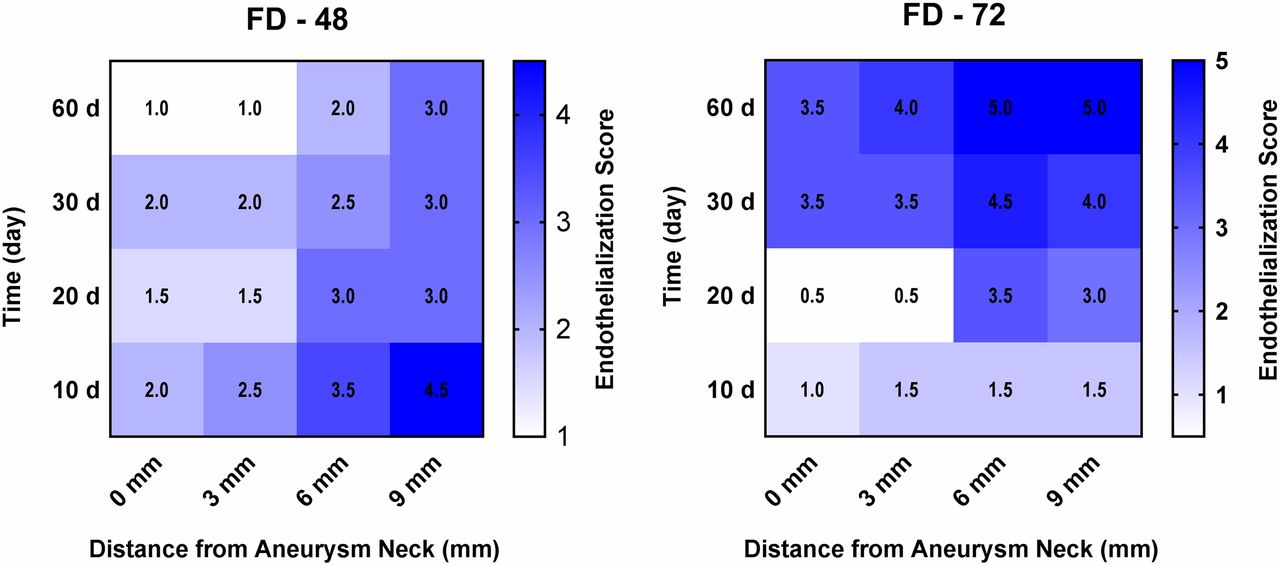
Inhomogeneous coverage was found at all time points where malapposition was seen. Endothelial cell growth over the surface was time-dependent for the FD-72 device (Spearman's r=0.86, p=0.013) but not for the FD-48 device (Spearman's r=−0.59, p=0.094). The endothelialization score was marginally correlated with the distance from the aneurysm neck for the FD-48 device (Spearman's r=1, p=0.083) but not for the FD-72 device (Spearman's r=0.8, p=0.33) (figure 3). Regardless of device, at 10 days continuous basement membrane was seen with an inhomogeneous spread of CD34+ PCs and partially matured endothelial cells. The endothelial layer became more evenly distributed at the 20-day, 30-day, and 60-day follow-up time points.
{kind=link}
{kind=link}
{kind=link}
Endothelialization matrix of flow diverter (FD)-48 and FD-72 devices. On the left side of the figure the color coded matrix suggests a location-dependent endothelialization pattern characteristic of the FD-48 device. On the right the ongoing endothelialization of the FD-72 device is mainly time-dependent, resulting in higher scores at the later time points.
Discussion
In this study we applied the SEM immuno-gold labeling technique in order to identify the PCs contributing to the healing process. At the same time we used standard SEM to analyze the morphological patterns of tissue coverage over the FDs. This technique showed that the group of cells located at the intersection of the struts (mostly seen at the aneurysm neck) contained CD34+ PCs in large numbers. Interestingly, distal to the neck at 5–10 mm where the device was in contact with the parent vessel wall the PCs were still present at the 60-day time point, but in fewer numbers. At that location and at 60 days, the FDs were completely covered with tissue and advanced endothelialization was found. Our results are in agreement with Li et al19 regarding the role of CD34+ PCs in the FD endothelialization process. They transfused fluorescent labeled PCs after FD implantation and were later able to identify them on the surface of the FDs. On the other hand, in another rabbit study Kadirvel et al suggested that the contributing cells in neointima formation were coming exclusively from the parent vessel wall but not from circulating PCs.20 Since acetylsalicylic acid (ASA) was administered in different doses in these studies, one possible explanation of this contradiction may be related to a potential side effect of ASA. Low-dose ASA (1 mg/kg) can potentiate the antithrombotic activity of clopidogrel while promoting the migration and adhesion of PCs needed for re-endothelialization.21–23 If ASA is given at a high dose, then both PC mobilization and differentiation may be limited. In a clinical study where the patients were treated with ASA (300 mg/day), they had a 50% decrease in the number of circulating CD34+/KDR+ PCs.24 To avoid this potential effect, we gave only 1 mg/kg ASA during the study. The platelet inhibition test (ARU) showed a mean value of 653±12, similar to the baseline value (prior to ASA treatment). It is important to mention that giving ASA in a very low dose, even when the inhibition is not measured, has a synergic effect on clopidogrel.21 Despite using a very low dose of ASA perioperatively, there was no in-stent thrombosis or periprocedural thromboembolic complication. These results may support the existing unfavorable relationship between ASA and PCs; however, more research is clearly needed to study this hypothesis.
These preliminary data offer insight into endothelial growth pattern as a function of device design. Although the total tissue coverage (regardless of endothelialization) over the surface of the FD-48 and FD-72 devices was quite similar at the latest time point (90.2±3.2% vs 87.4±10.1%), the maturation of endothelial cells over the basement membrane showed different patterns in the two device groups. Termination of the healing process over the implanted device along with permanent exclusion of the aneurysm from the circulation occurs when a continuous neointima is present over the entire surface of the device. The anti-thrombogenic endothelial cell coverage may be important to termination of DAT. Interestingly, in our study the endothelial cell growth was time-dependent for the FD-72 device over the surface but not for the FD-48 device. However, the endothelialization score was marginally correlated with the distance from the aneurysm neck for the FD-48 device but not for the FD-72 device. This could mean that the design of the FD-72 device can offer more consistent endothelialization with less dependence on the location.
Regardless of the device used, evenly covered struts were found where the device was in contact with the vessel wall. Delayed incomplete coverage was present at the fusiform segments and where malapposition was identified on the final DSA. Because most of the aneurysms treated in our study had a complex morphology with a partially fusiform distal parent vessel, we could evaluate the ongoing healing process in challenging, clinically relevant circumstances. Large-necked complex aneurysms along with varying parent vessel diameters is a recurrent scenario in clinical practice and needs case-by-case decisions in order to accurately deploy the device.
Trends in these preliminary data, such as the slightly improved endothelialization at the earliest time point for the FD-48 device with decreased endothelialization at 60 days, require further study. Our observations indicate that apposition of the device to the vessel wall is critical for effective tissue engineering of the device, which is supported by independent reports of aneurysm occlusion rates in this model that are dependent on proper FD apposition.25 Apposition is not only a function of FD design but also of parent vessel anatomy where, in certain cases in the rabbit model, there can be dilation of the parent artery due to elastase leakage during model creation.26 Additionally, we observed that aneurysms with smaller necks experienced rapid endothelialization, which is supported by an analysis of aneurysm occlusion rates in this model.27 To determine the relative contributions of these variables, further study in a larger number of animals is required. Notably, in our study, aneurysm size and morphology were matched for each block (pairing device type for a prospectively determined follow-up time point) in an effort to reduce confounding variables.
Our study has several limitations. Although the aneurysm thrombosis rate was indirectly evaluated by occlusion rate seen on follow-up angiography, this was not affirmed by histological analysis since our hypothesis required en face preparation of the specimens. Furthermore, we were able to identify endothelialization patterns in the two groups but, due to the small sample size, the results should be interpreted with care. These exploratory findings require additional confirmatory studies. Future work should not only confirm our results but should also explore different FD designs.
Conclusion
The presented data support the hypothesis that circulating CD34+ PCs contribute to FD endothelialization and that PCs are present throughout the healing process up to 60 days. Although there was no difference in complete aneurysm occlusion, we have preliminary evidence of temporal and spatial dependence of endothelialization on FD design. Future FD designs can incorporate these analyses during development to accelerate the in situ tissue response to the scaffold.
References
Footnotes
Contributors Study design: MJG, ASP, AKW, GMH, JA and MM. Data acquisition: MM, ETL, LS, KvdM and IRL. Literature research: MM, MJG and AKW. Data analysis and interpretation: MM, AKW, MJG, ASP and SV. Manuscript preparation: MM and MJG. Revision of manuscript for important intellectual content: LS, SV, JA, SL, GMH, ASP, IS, AKW and MJG. Approval of final version of manuscript: all authors.
Funding This work was supported by Stryker Neurovascular.
Competing interests MJG has been a consultant on a fee-per-hour basis for Codman Neurovascular and Stryker Neurovascular; holds stock in InNeuroCo; and has received research support from the National Institutes of Health (NIH), Codman Neurovascular, Stryker Neurovascular, Microvention, Medtronic Neurovascular, Philips Healthcare, InNeuroCo, Neuronal Protection Systems, the Wyss Institute and Silk Road. ASP has received research grants from Medtronic Neurovascular and Stryker Neurovascular. AKW: Consultant for Codman Neurovascular and Stryker Neurovascular; research grant: NIH, Philips Healthcare, Wyss Institute; speaker: Harvard Postgraduate Course, Miami Cardiovascular Institute; co-founder of InNeuroCo and major stockholder; stocks in EpiEB and Pulsar Medical. IS: Consultant for Stryker Neurovascular and ev3/ Covidien, Chestnut Medical. JA and SL are employed by Stryker Neurovascular.
Ethics approval Ethics approval was obtained from the university's Institutional Animal Care and Use Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement For access to the raw images obtained in this study, please contact the corresponding author.