Article Text

Abstract
Background Compared with males, females consistently fare worse following mechanical thrombectomy for large vessel ischemic strokes. Understanding why this gender disparity occurs may guide improvements in future treatment strategies. In this study, we aim to determine whether gender differences in cerebral arterial diameter correlate with clinical outcomes following stroke thrombectomy.
Methods We performed an observational study of consecutive acute ischemic stroke patients undergoing mechanical thrombectomy at a single, urban tertiary care medical center. Catheter angiographic images were used to manually measure proximal segment arterial diameters in a standardized fashion. Medical record review was used to obtain relevant independent and dependent variables.
Results Ninety two patients (42 females) between June 2013 and August 2016 met inclusion criteria. Internal carotid artery (ICA) terminus diameters for males and females were 3.08 mm (SD=0.46) and 2.81 mm (SD=0.45), respectively (P=0.01). M1 segment middle cerebral artery (MCA) diameters for males and females were 2.47 mm (SD=0.30) and 2.18 mm (SD=0.31), respectively (P<0.0001). 48% of patients in the upper MCA caliber tertile attained a favorable mRS 90 day value compared with 35% in each of the lower and middle tertiles (P=0.51). Larger MCA diameters correlated with favorable discharge disposition (P=0.21).
Conclusions These results provide limited evidence that males have larger cerebral arterial diameters than females and that larger arterial diameters may improve the odds for favorable clinical outcomes. If future studies validate these findings, arterial diameter may become a relevant variable in the design of improved thrombectomy strategies.
- thrombectomy
- stroke
- intervention
- angiography
Statistics from Altmetric.com
Introduction
Stroke is the leading cause of adult disability in the United States with an annual total cost of $34 billion.1 2 These costs are disproportionately driven by patients with large vessel cerebral arterial occlusions, who most often have severe disability.
Recently published level 1a evidence has proven the clinical benefit of mechanical thrombectomy for acute ischemic strokes involving proximal vessels of the anterior circulation.3–7 However, multiple studies report a gender disparity in post-thrombectomy outcomes with females faring worse than males.8–17 In a 2-year prospective cohort study of 676 consecutive ischemic stroke patients, Silva et al demonstrated that significantly more male patients attained favorable functional outcomes (males 75.4% vs females 58.7%) and were able to live independently at home 6 months after ischemic stroke (males 66.9% vs femalse 49.4%).8
Spaander et al17 evaluated 9495 patients treated with intravenous thrombolysis and found that after adjustment for baseline differences including age, female sex was still associated with poor functional outcome with an OR of 1.15; 95% CI 1.02 to 1.31. Despite much investigation, explanations for this observed disparity remain elusive. Prior studies looking at baseline patient characteristics, quality of clinical care, cardiovascular comorbidities, depression, or ischemic infarct capacity have not found convincing explanations for this gender-based outcome disparity.8 10 11 15 18
Gender differences have been reported in circle of Willis cerebral aneurysm distribution and vessel caliber.19 20 Based on the Hagen–Poiseuille equation, vascular caliber could influence ischemic stroke outcomes as the arterial diameter proportionally affects the volumetric vessel flow rate. Our study aim was to determine if gender-based differences in cerebral arterial diameter contribute to the gender disparity in acute ischemic stroke outcomes. Specifically, proximal cerebral artery diameters were manually measured using digital subtraction angiography (DSA) in a consecutive series of patients undergoing stroke thrombectomy.
Methods
Data collection
A consecutive series of patients undergoing mechanical thrombectomy at an urban, tertiary care academic medical center were reviewed. Only patients with DSA-confirmed occlusive strokes involving large vessels of the anterior circulation were included in the study population.
Independent variables including age, vascular risk factors, admission NIHSS score, IV-tPA administration, and anatomic stroke occlusion location were recorded. Procedural modifiers, specifically mechanical thrombectomy device selection(s), number of device passes to obtain recanalization, time to recanalization, post-interventional TICI score, pneumonia incidence, and DVT incidence, were obtained from the medical record. The study’s primary outcome measure, 90 day Modified Rankin Scale (mRS), was acquired via vigilant telephone contact made by trained stroke coordinators. Discharge location was a secondary outcome measure. Patients with missing primary or secondary outcome measures in their medical record were omitted from the study sample.
DSA offers the highest cerebrovascular spatial resolution available.21 As such, DSA images obtained during thrombectomy were used to measure cerebral arterial diameter. A consistent imaging protocol was used for all DSA image acquisitions. Specifically, images were obtained on an Artis interventional angiography biplane system (Siemens AG; Munich, Germany) with iopamidol contrast. DSA series sets were retrieved and viewed on a Syngo workstation (Siemens AG; Munich, Germany). Coronal image calibrations were made using the manufacturer-recommended table object distance (TOD) methodology. All measurements were made from the anterior-posterior image perspective in a standardized fashion, perpendicular to the vessel walls (figure 1). Using a previously described method, ICA diameters were measured 3 mm proximal to the ICA terminus and M1 segment measurements were made 3 mm distal to the MCA origin, past the carotid terminus.22 Prethrombectomy images were preferred, however if the arterial occlusion precluded arterial diameter measurement, then the arterial diameter after revascularization was used. Any patients without an anterior-posterior DSA contrast image series that allowed for accurate ICA and MCA measurement were omitted from the study sample.
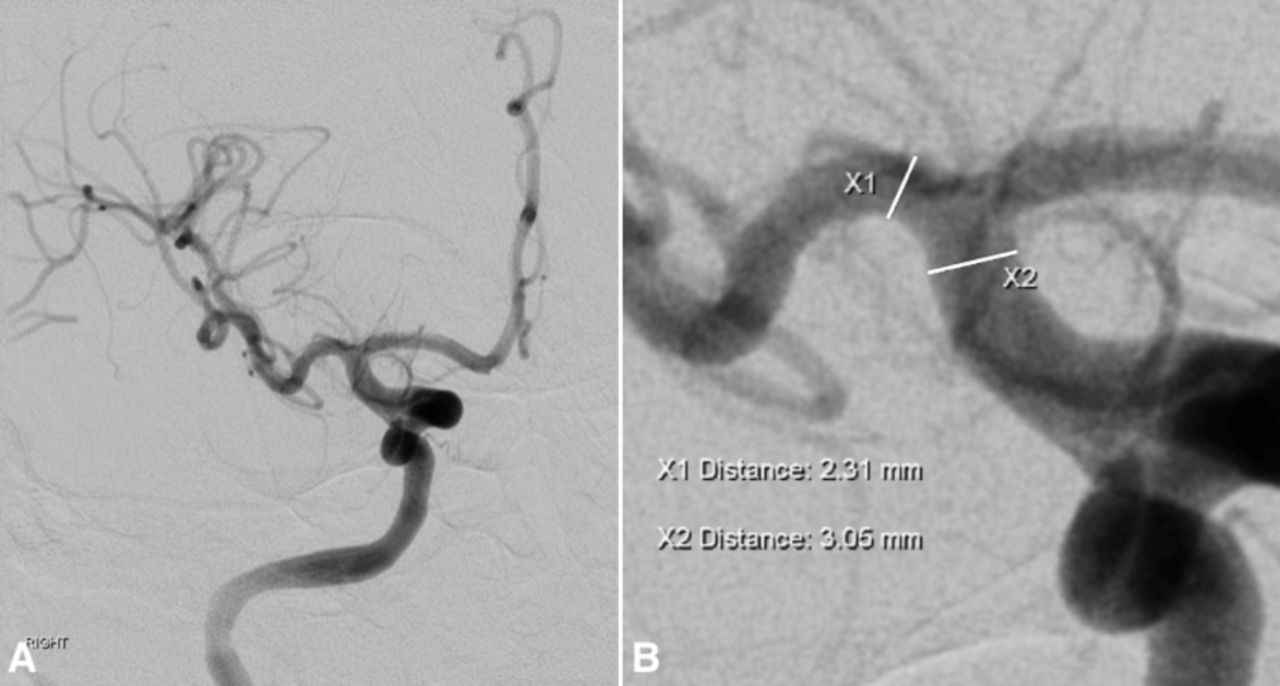
Anterior-posterior DSA image of a recanalized right anterior cerebral circulation (A); A magnified view was used to obtain MCA and ICA diameters (X1 and X2, respectively) perpendicular to the vessel wall (B).
Statistical methodology
Demographic variables, procedural modifiers, as well as ICA terminus and M1 origin measurements were compared using student t-test, χ2 test, or Fisher’s exact test where appropriate. Patient mRS values at 90 days following thrombectomy were dichotomized into either favorable (mRS ≤2) or unfavorable (mRS >2) scores. Primary and secondary outcome measures were contrasted among gender groups using χ2 tests. A multi-variable regression analysis looking at the relation between cerebral vessel diameter (ICA or MCA) and mRS 90 day score was also performed. Covariates included age, time to recanalization, NIHSS admission score, passes to recanalization, and vascular risk factors.
Among patients with TICI 2b/3 recanalization, the relationship between MCA diameter and clinical outcome in male and female patients were distributed into an upper, middle, and lower tertile grouping according to MCA diameter. 90 day mRS and discharge location were compared between the upper, middle, and lower MCA diameter tertiles with χ2 tests. All statistical analyses were performed with SAS 9.3 (SAS Institute Inc, Cary NC, USA), and a P value <0.05 was considered significant.
Results
From June 2013 through August 2016, 121 patients presented with a DSA-confirmed anterior circulation large vessel occlusion and underwent thrombectomy. Seventeen patients with posterior circulation occlusions and two patients with inadequate imaging were omitted. Ten patients (three females, seven males) were unreachable for mRS 90 day evaluation, yielding a 90.2% follow-up rate. Ninety-two patients (42 females, 50 males) satisfied the pre-specified inclusion criteria.
Female patients were older (66.6±13.2 vs 60.8±14.7, P=0.049). ICA terminus diameters for males and females were 3.08 mm±0.46 mm and 2.81 mm±0.45 mm, respectively. MCA diameters for males and females were 2.47 mm±0.30 mm and 2.18 mm±0.31 mm, respectively. Male ICA terminus and MCA measurements were larger than female (P=0.01 and P<0.0001, respectively). The remaining independent variables and procedural modifiers were statistically similar between the gender cohorts (table 1).
Summary of patient demographics, vessel caliber measurements, and procedural modifiers
90 day mRS ≤2 for males and females were 44% and 28.6%, respectively (table 2). While not statistically significant (P=0.13), there appears to be a trend suggesting worse functional outcomes in female patients. No gender differences were identified in the discharge location distribution. Multi-variable regression analysis yielded no significant correlation between 90 day mRS ≤2 values and ICA or MCA vessel diameter after controlling for covariates (P=0.80 and P=0.67, respectively).
Summary of primary and secondary outcome measures
Seventy nine patients (37 females, 42 males) who achieved TICI 2b/3 recanalization underwent MCA caliber tertile analysis. MCA diameter tertile ranges were: lower (1.58–2.22 mm), middle (2.23–2.55 mm), and upper (2.56–3.06 mm). Female patients comprised 22% of the upper, 46% of the middle, and 73% of the lower tertile. Within the lower and middle MCA diametric tertiles, 35% of the patients achieved 90 day mRS ≤2 compared with 48% of patients in the upper tertile (figure 2). χ2 analysis demonstrated no difference between tertile groupings (P=0.51). A power analysis indicated that 571 patients would have been required to provide 80% power to detect this difference found in our data.

MCA diametric tertile analysis depicting the relationship between mRS 90 day value and MCA caliber in recanalized patients.
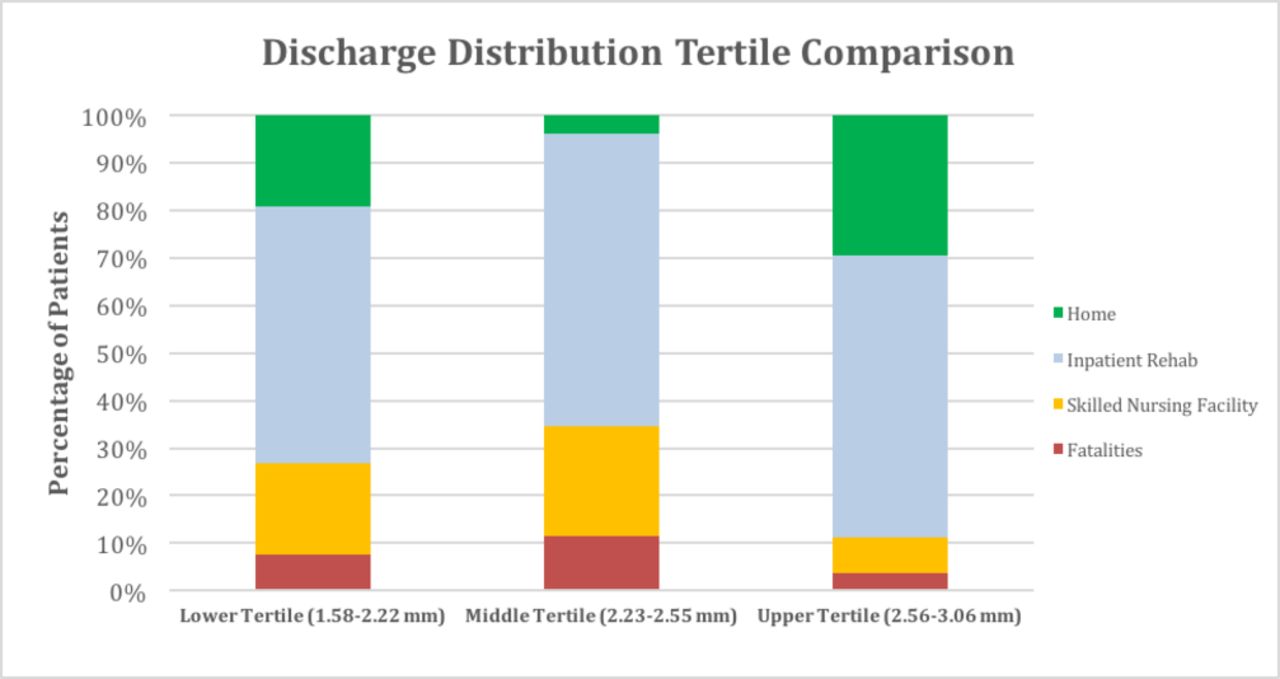
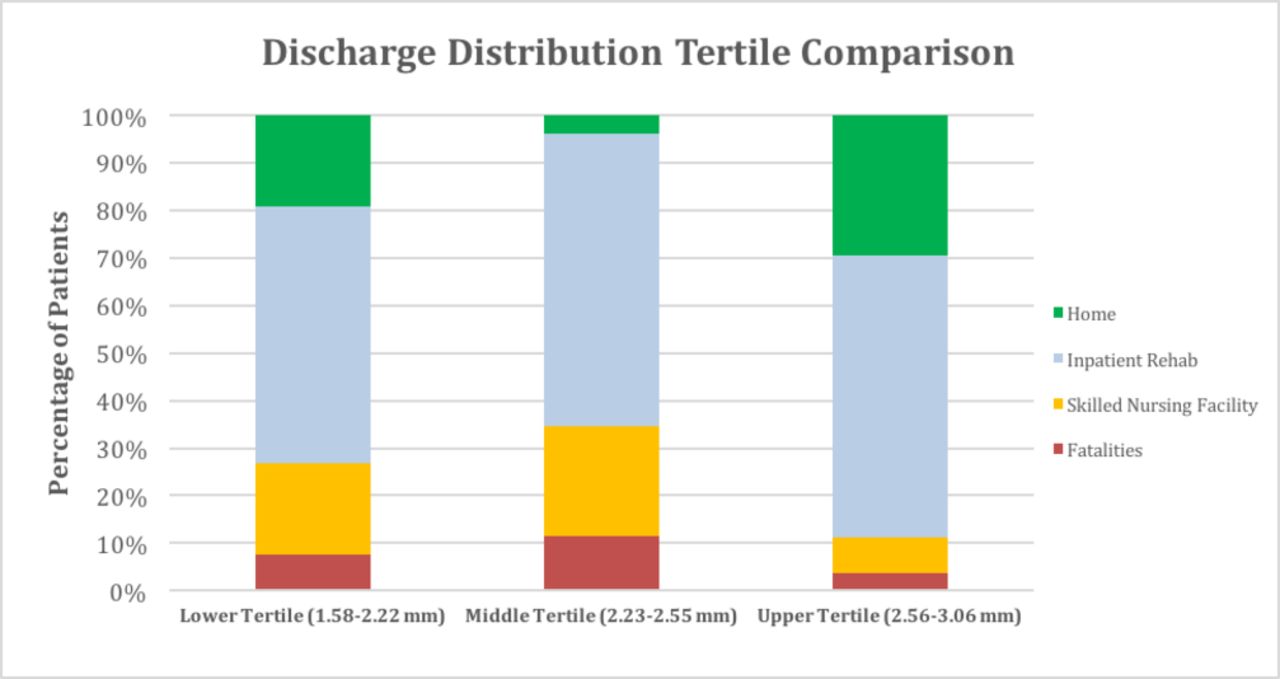
When evaluating discharge location, 29.6% of patients in the upper tertile were discharged home compared with 3.8% and 19.2% of patients in the middle and lower tertiles, respectively. Moreover, 7.4% of upper tertile patients were discharged to a skilled nursing facility, compared with 23.1% and 19.2% of patients in middle and lower tertiles, respectively (figure 3). χ2 analysis demonstrated no difference between tertile grouping discharge disposition (P = 0.21).
{kind=link}
{kind=link}
{kind=link}
MCA diametric tertile analysis depicting the relationship between discharge location and MCA caliber in recanalized patients.
We found no difference between TICI 2b/3 scores (male-84% female-88.1%, P=0.57) or number of passes (1 Pass: male-42.5% female-49%;>1 Pass male-57.5% female-51%; P=0.60) between males and females. While there is a numerical trend here that would portend a more favorable outcome for females, these findings were not statistically significant. Additionally, a greater percentage of male patients had carotid or ICA terminus occlusions (table 1).
Discussion
The study objective was to investigate for ICA and M1 arterial diameter differences as an explanation for the observed gender disparity in functional outcomes following stroke thrombectomy. Consistent with prior cohort studies, the female group mean age was significantly older than male, and may very well contribute to the observed differences in functional outcome as seen in prior studies.8 However, significant differences in mean cerebral arterial diameter between males and females were also identified. The tertile analysis indicated a correlation between the M1 segment diameter and favorable 90 day mRS outcomes. Likewise, the MCA tertile discharge location distribution profile demonstrated a similar correlation with diameter in males and females. Collectively, these results suggest that differences in cerebral arterial diameter may contribute to the gender disparity seen in stroke outcomes.
Previous research evaluating cerebral vascular diameters to explore flow patterns of cerebral emboli and the effects of physiologic stimuli on vessel dimensions relied on non-invasive imaging modalities including computed tomographic angiography (CTA) and magnetic resonance angiography (MRA).22–24 Unique to the current study was the use of DSA, which is fortunately inherent to thrombectomy, and allows for highly precise vessel diameter measurements. This technique has been previously used to measure and compare the ICA and MCA diameters in children and adults to guide neurointerventional device selection.25 DSA provides the spatial resolution necessary for more precise measurements which were necessary to most accurately evaluate our study hypothesis.21 26
Prior observational studies report that female stroke patients have worse functional outcomes and are less likely to live independently compared with males, despite controlling for age and other comorbidities.8–17 The current study similarly found that only 28.6% of females compared with 44% of males had a mRS 90 day value of 0–2. While this result was not statistically significant (P=0.13), a power calculation indicates that this finding is likely attributed to insufficient sample size. More specifically, a study sample of 304 patients (152 females) would have provided 80% power to detect a difference (15.4%) at 0.05 significant level.
Despite evaluating for several potential explanations, no compelling findings have yet been published to explain this gender disparity.8 10 11 15 18 Prior investigations have considered quality of clinical care, differences in baseline clinical characteristics, cardiovascular comorbidities, and depression: however none of these factors have been shown to have a definitive correlation. Silva et al compared male and female ischemic infarct volumes following acute stroke but was unable to demonstrate a significant difference between genders (female 23.73 cm3 vs male 13.21 cm3, P=0.21).8
Our study’s findings are consistent with the vessel flow rate principles defined in the Hagen–Poiseuille equation. Specifically, the equation asserts that the volumetric flow rate through a cylindrical conduit is proportional to its radius to the fourth power. Consequently, small increases in arterial caliber permit substantial increases in volumetric flow rates and subsequent improvements in tissue perfusion. Despite our average female MCA diameter being only 0.29 mm less than males, this actually correlates to a female volumetric flow rate that is 60.7% of the male flow rate, based on the Hagen– Poiseuille equation.
Patients with greater intracranial arterial diameters may therefore benefit from superior immediate post-recanalization flow and vessel patency during the recovery period. Marks et al27 are among many who have demonstrated that improved angiographic reperfusion positively correlates with functional outcomes and less infarct growth. Specifically, 57% of patients with TICI 2b/3 scores following endovascular recanalization for ischemic stroke experienced favorable mRS scores compared with only 24% of TICI 0-2a patients.
Larger cerebral arteries may increase the probability of first-pass recanalization or overall recanalization success. Our findings however, did not reflect these hypothesized mechanisms. As mentioned previously, TICI 2b/3 scores and number of passes were similar between males and females. Although variations in vessel size may more closely affect recanalization rates rather than 90 day mRS ≤2, another mechanism whereby vessel size could influence outcomes is via greater collateral flow. We therefore chose 90 day mRS ≤2 as our primary outcome measure to reflect the variety of mechanisms by which vessel size could affect clinical outcomes. Arterial diameter hence represents a discrete anatomic feature that may serve not only as a target in designing future ischemic stroke therapies but also to specifically evaluate mechanisms such as first pass success rate, number of passes, and collateral flow in future larger studies.
The relationship between arterial diameter and clinical outcomes have been previously studied in extracranial vascular disease. A study by Hong et al28 found during endovascular treatment for common and external iliac artery disease, smaller target lesion artery diameters, as determined via CTA, were independent predictors of procedural failure. Similar findings were demonstrated in patients with peripheral artery disease undergoing lower extremity bypass whereby great saphenous graft conduit diameter <3.5 mm was a primary technical determinant of graft failure.29 A more recent study by Lagergren et al30 noted that females have worse outcomes following lower extremity bypass grafting, hypothesizing differences in arterial diameter of the great saphenous vein graft as the cause. They found that graft diameter taper (difference between above- and below-knee diameters) was greater in females resulting in inferior patency when compared with male patients.30
If larger vessel caliber correlates with more favorable stroke outcomes, several clinical treatment modifications could potentially exploit this concept. Vasodilators may increase vessel diameter and increase blood flow through the affected vessels. Calcium channel blockers, acetazolamide, and hypoventilation have been shown to have this effect on cerebral vessels and may serve as future therapeutic targets.
A variety of recanalization techniques and devices were used for thrombectomy. Despite this variability, the overall recanalization rate, time to recanalization, and first pass success rate between males and females were comparable, further emphasizing the role of arterial diameter on outcomes (table 1).
This study has several limitations inherent to an unfunded, investigator-initiated clinical study relying on detailed anatomic measurements. First is the sample size. Given the potential for numerous confounders, including social, demographic, genetic, and hormonal factors, a larger sample size would have increased statistical power. Second, the sample was from a single tertiary care, urban academic medical center, which may introduce a degree of selection bias or increase the risk of random error. Multicenter collaboration could have mitigated this limitation, but given the standardized, manual measurements needed to ensure consistency in the measurement of arterial diameter, data precision and accuracy were valued over scale.
Since the current study relied on catheter angiographic imaging during the thrombectomy procedure, only the cerebral arterial anatomy of the affected hemisphere could be reliably measured. Contralateral vascular images were not consistently available. Bilateral measurements could have been obtained from many of the patients who underwent CTAs, but image resolution and measurement precision would have been inferior. Lastly, despite attempts to standardize the arterial diameter measurement approach, it was difficult to reliably measure the exact same anatomic segment in every patient given the inherent inter-individual anatomic variability and subtle deviations in anterior-posterior DSA image acquisition angles. Consequently, the results and implications of the present study must be assessed in the context of these limitations.
Conclusions
These results provide limited evidence that males have larger cerebral arterial diameters than females and that larger arterial diameters may improve the odds for favorable clinical outcomes following stroke thrombectomy. If future studies validate these findings, arterial diameter may become a relevant variable in designing improved thrombectomy strategies.
References
Footnotes
Contributors MAD: study design, literature review, data collection, statistical analysis, drafting and revising of the manuscript; guarantor. BO: statistical analysis and revising of the manuscript. KMK: data collection and study design. MC: study design, monitored data collection, revising manuscript; guarantor.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Rush University Medical Center Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.