Article Text

Abstract
Objective To evaluate multiparametric MRI including non-contrast and contrast-enhanced morphological and angiographic techniques for intracranial aneurysms treated with the single-layer Woven EndoBridge (WEB) embolization system applying simultaneous digital subtraction angiography (DSA) as the reference of standard.
Materials and methods We retrospectively identified all patients with incidental and acute ruptured intracranial aneurysms treated with a WEB device (WEB SL and WEB SLS) between March 2014 and June 2016 in our neurovascular center with early (within 7 days) postinterventional multiparametric MRI as well as mid-term (5–8 months) follow-up MRI and DSA available. Occlusion rates were recorded both in DSA and MR angiography (MRA). In MRI, signal intensities within the WEB as well as in the occluded dome distal to the WEB, if present, were measured by region-of-interest (ROI) analysis.
Results Twenty-five patients fulfilled the inclusion criteria. Rates of complete/adequate occlusion at mid-term follow-up were 84% with both MRA and DSA. A strong signal loss within the WEB was observed in all MR sequences at initial and follow-up examinations. ROI analysis did not reveal significant differences in non-contrast (P=0.946) and contrast-enhanced imaging (P=0.377). A T1-hyperintense thrombus in the non-WEB-carrying dome was a frequent observation.
Conclusions Signal intensity measurements in multiparametric MRI suggest that neither contrast-enhanced MRA nor morphological sequences are capable of revealing reliable information on the WEB lumen, presumably due to radio frequency shielding. MRI is therefore not suitable for confirming complete thrombus formation within the WEB.
- aneurysm
- angiography
- MRI
- standards
- brain
Statistics from Altmetric.com
Introduction
Endovascular treatment has become the favored procedure for both ruptured and unruptured intracranial aneurysms.1–3 The Woven EndoBridge (WEB; MicroVention, Tustin, California, USA) is an intrasaccular braided wire endovascular device designed to embolize intracranial aneurysms with unfavorable anatomy (large aneurysms, wide-necked aneurysms) to provide flow disruption.4–6 It is constructed of nitinol wires forming a mesh structure secured by a proximal and distal platinum marker.6 Several configurations of the WEB device are available and the optimal size for the aneurysm must be carefully chosen before treatment.6 To date, the clinical results after WEB treatment of complex, especially wide-necked, aneurysms are encouraging, demonstrating good occlusion rates also at mid-term follow-up.4 5 7 Nevertheless, a treated intracranial aneurysm can recur, and patients treated with the WEB device should receive long-term follow-up for detecting possible recurrence.4 Since there still is a risk of permanent deficit from digital subtraction angiography (DSA) examinations,8 MRI has become the preferred method for follow-up after endovascular treatment of intracranial aneurysms.4 Both time-of-flight MR angiography (TOF-MRA) and contrast-enhanced (CE)-MRA are suitable methods for detecting aneurysm recurrence.4 9
The time course of early thrombus formation within the WEB leading to aneurysm occlusion has not been thoroughly evaluated to date, mainly because early repeated DSA is not available due to its invasive character. It is known that WEB occlusion shows a wide interindividual variability.10 11 MRI might serve as a suitable alternative.
Since the WEB device is technically a closed ‘cage’ with a regular structure, leaving the inner dome of the aneurysm open for thrombus formation, a different behavior in MRI can be expected especially in comparison to coils, which normally form an irregular cast within the whole aneurysm dome.
The primary aim of this study was to evaluate whether multiparametric MRI is capable of visualizing actual thrombus formation inside the WEB device after endovascular treatment of intracranial aneurysms corresponding to aneurysm occlusion. We hypothesized that the structure of the WEB acts as a shield for radio frequencies applied in MRI scanning, nulling the signal within the device and therefore making it impossible to conclude complete thrombus formation within the WEB from MRI.
We secondarily hypothesized that, in our collective, MRA is consistent with DSA regarding mid-term follow-up after WEB embolization of intracranial aneurysms in this single-center collective, as reported previously.4 12
Methods
Study population
This retrospective evaluation was conducted in accordance with the Declaration of Helsinki in its currently applicable form, and the local ethical review committee waived the need for informed consent. We retrospectively identified all patients who had been treated with a WEB device between March 2014 and June 2016 in our university neurovascular center, either presenting with an incidental aneurysm or needing emergency treatment in the setting of subarachnoid hemorrhage due to acute rupture of an intracranial aneurysm (n=44). Patients who had initially been planned to have the WEB device but underwent change of treatment during the procedure were not included in this evaluation. Use of a permanent adjunctive device such as a stent, coil or flow diverter was an exclusion criterion in order to exclude possible sources of interfering susceptibility artifacts in MRI.
Imaging
Our standard follow-up for intracranial aneurysms treated with the WEB device comprises initial MRI within the first 7 days after the procedure and follow-up MRI and DSA 6 months after initial treatment.
All MRI scans were performed on a 1.5 T scanner (Avanto; Siemens, Erlangen, Germany) using an eight-element, phased-array, receive only, head coil. The standard MRI protocol included conventional morphological pulse sequences, time-of-flight MRA as well as CE-MRA and additional high-resolution fat-suppressed T1-weighted sequences before and after contrast administration (table 1). All DSA examinations were performed on a biplane angiographic system (Allura Clarity FD 20/20; Philips Healthcare, Best, The Netherlands). In the standard follow-up setting, using transfemoral catheterization, we obtained selective series of the respective artery (internal carotid artery or vertebral artery) in anteroposterior and lateral projections, a three-dimensional rotational angiography, and an additional optimized working view projection.
Standard MRI protocol
Image analysis
Region-of-interest (ROI) analyses were performed in both early and mid-term MRI. We compared coronal fat-suppressed T1-weighted images before and after contrast media application by placing ROI in the center of the WEB within each aneurysm, respectively. Average signal intensity values were divided by a reference ROI located in the lateral ventricle to obtain a quantitative statement.
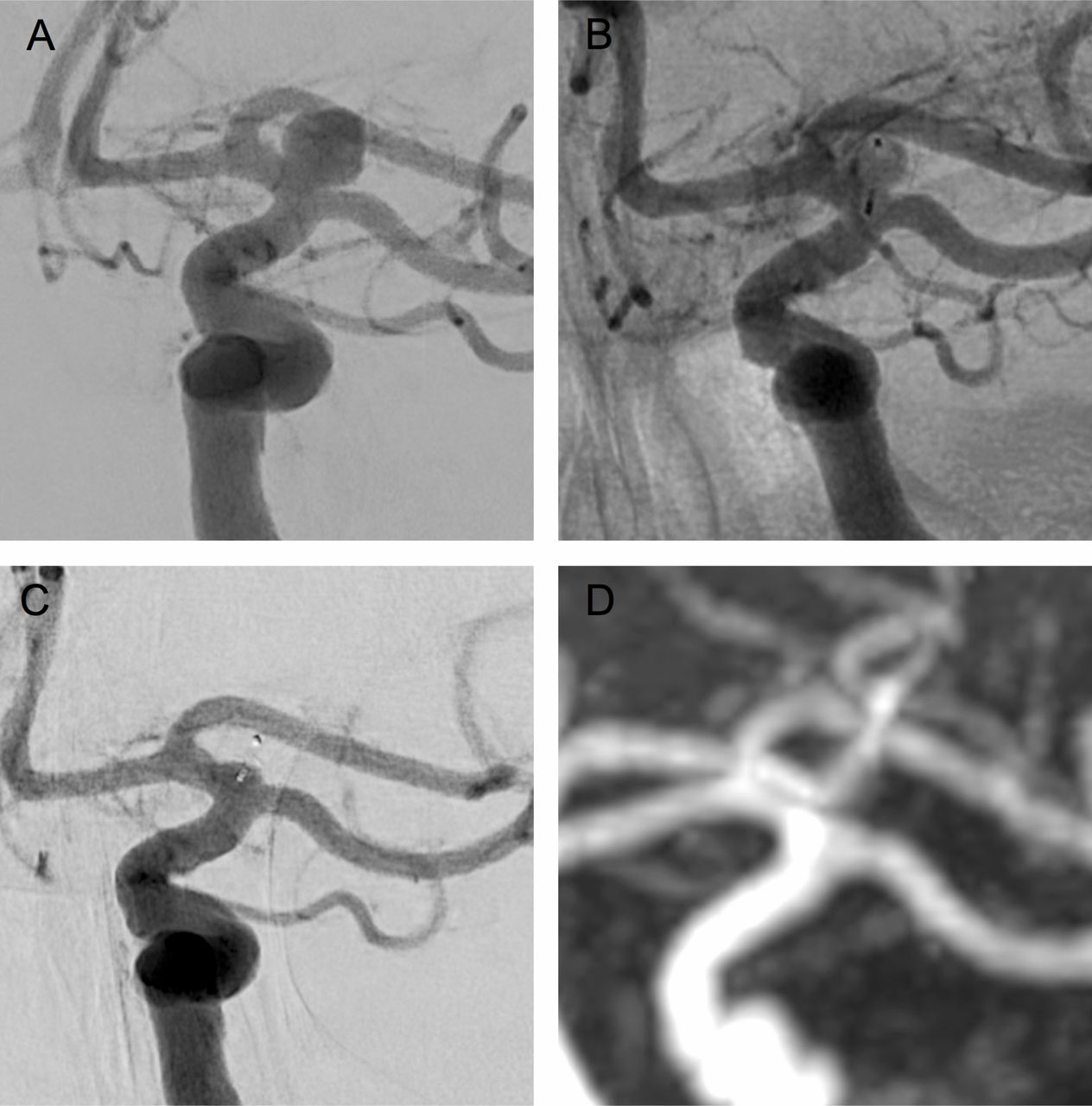
Aneurysm occlusion rates were assessed for both MRA and DSA, graded as complete occlusion (grade A), neck remnant (grade B), and residual aneurysm (grade C) according to the classification scale proposed by Lubicz et al.1 13 Grading was performed as a consensus reading by the two most experienced operators (JB and MB; WEB experience >3 years, respectively). Residual recess, inherent to the WEB device, was considered as complete occlusion (grade A).1 14 An example of concordance between CE-MRA and DSA is shown in figure 1.

Comparison of initial and follow-up digital subtraction angiogram (DSA) and contrast-enhanced MR angiogram (CE-MRA) of a left carotid-T aneurysm showing good intermodal correlation. (A) Pretreatment DSA working view. (B) Immediate post-treatment DSA. (C) Follow-up DSA showing complete occlusion of the aneurysm. (D) Follow-up CE-MRA also showing complete occlusion.
In vitro experiment
To support the hypothesis that radio frequency shielding is characteristic of the WEB device itself and not due to other reasons, an example in vitro experiment was added. One WEB SLS 9 was placed within an elastic aneurysm model, which was completely perfused with water containing a minimal amount of contrast medium (1.5 mL Dotarem; Guerbet, Roissy CDG, France) solution. The same imaging protocol as described in table 1 was performed on the model.
Statistical analysis
Quantitative variables are described as mean±SD while qualitative variables (e.g gender) are shown as number and percentage. The collected data did not follow a normal distribution so p-values were calculated using the Mann–Whitney U test. Analyses were performed using IBM SPSS Statistics 24 (SPSS Statistical Software, IBM, Armonk, USA) and MS Excel 2016 (Microsoft; Redmond, USA).
Results
Patient and aneurysm data
Twenty-five patients including 21 women (84%) and four men (16%) were finally enrolled in the study. Nineteen of 44 treated patients were excluded because of the following: in 10 patients the MRI protocol was incompletely acquired, five patients were lost for follow-up MRI at the time of data collection, and four died in the period after treatment (all initially presented with subarachnoid hemorrhage Hunt and Hess grade IV or V). Five patients from the collective evaluated have also been enrolled in the WEBCAST 2 study.15 Twenty-one patients were treated with a WEB SL and four patients received a WEB SLS. Patients were aged 45–81 years at the time of treatment (mean 56.6±8.9 years). WEB placement was performed electively in 16 cases and emergently in eight cases. One patient treated with the WEB device presented with aneurysm recurrence after previous coiling. Aneurysm locations were as follows: middle cerebral artery, 2 (8%); anterior communicating artery, 9 (36%); basilar artery, 7 (28%); posterior inferior cerebellar artery, 1 (4%); internal carotid artery/posterior communicating artery, 3 (12%); and internal carotid artery terminus, 3 (12%). Intraoperative adverse events occurred in one patient (4%) who suffered a periprocedural M2 occlusion. This patient was treated by intravenous administration of abciximab and dual antiplatelet treatment for 3 months and no clinical deficit occurred. No allergic reactions to contrast media or periprocedural ischemia were observed.
Early MR angiographic outcome
Early MRI was performed within 7 days after the day of treatment. In MRA, complete aneurysm occlusion (grade A) was obtained in 21/25 patients (84%), neck remnant (grade B) in 3/25 patients (12%), and aneurysm remnant (grade C) in 1/25 patients (4%).
Mid-term angiographic outcome
Mid-term MRI and first DSA were performed 5–8 months after treatment. One of the mid-term DSA examinations was performed 1 year after treatment due to patient delay. Complete aneurysm occlusion (grade A) was stable in 19/25 patients (76%). In 2/25 patients (8%), initial complete aneurysm occlusion turned into neck remnant (grade B), and in 1/25 patients (4%) with prior neck remnant a worsening of the aneurysm occlusion was observed at mid-term follow-up, developing an aneurysm remnant (grade C). The grading over time is shown in figure 2. In two patients (numbers 1 and 18 in tables 2 and 3), partial opacification of the inner WEB lumen was still visible on DSA at 6-month follow-up; there was no correlating finding on TOF/CE-MRA or morphological MRI.
Imaging findings and results of region-of-interest (ROI) analysis at early MRI
Imaging findings and results of region-of-interest (ROI) analysis at 6-month MRI
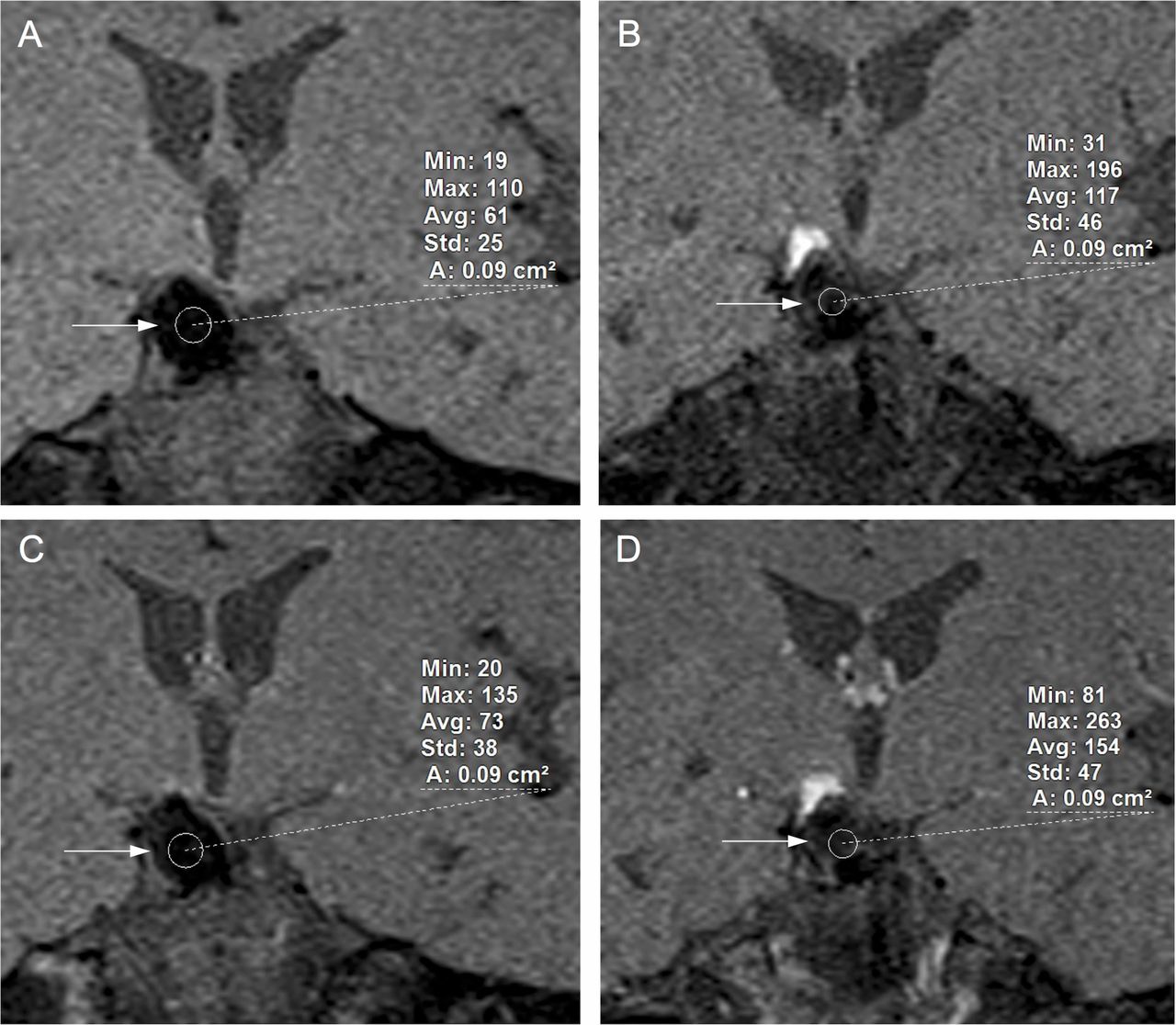
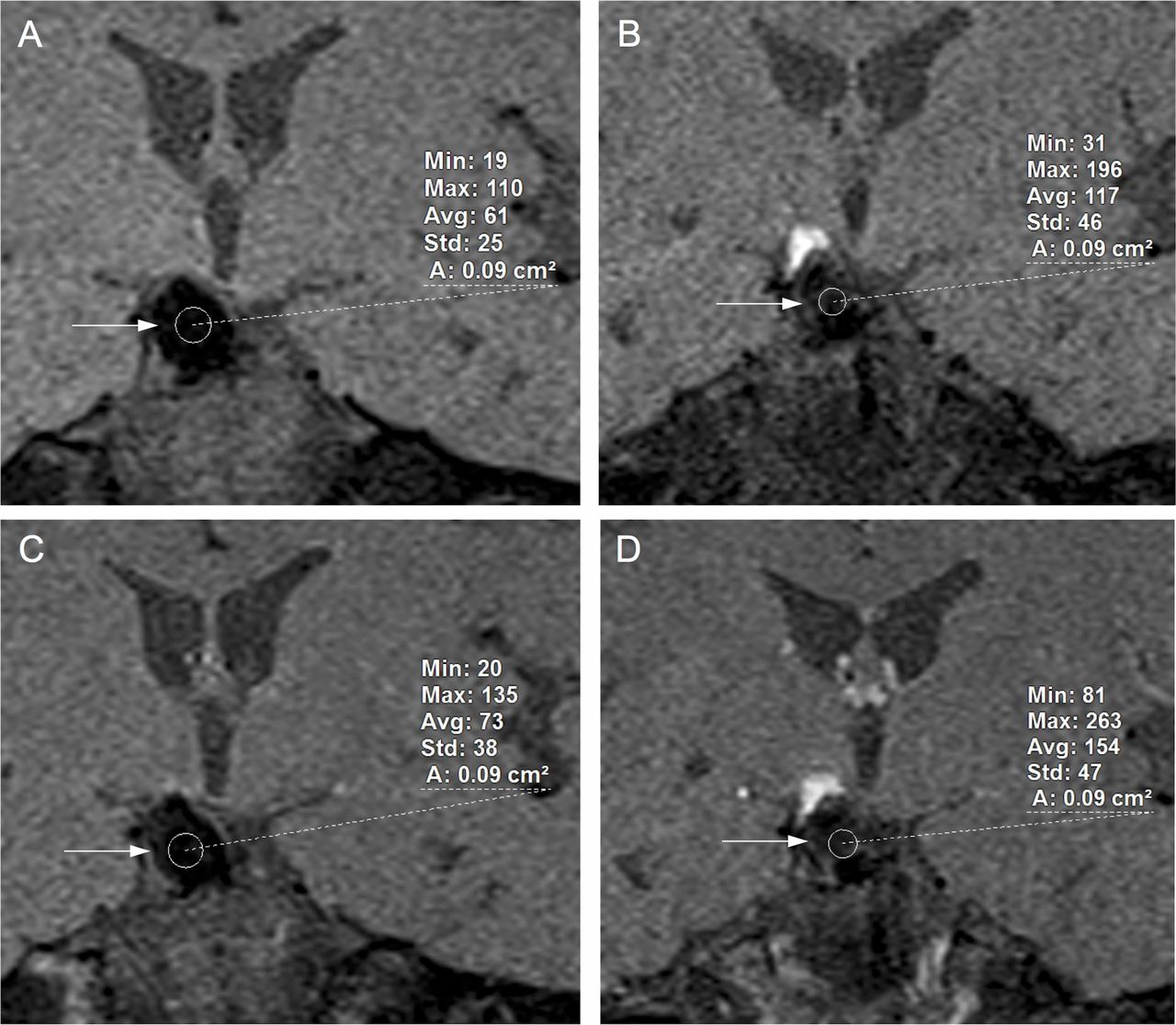
Example of region of interest (ROI) inside the WEB device between initial and follow-up imaging, both non-contrast and contrast-enhanced T1-weighted MRI applying spectral fat suppression: incidental basilar tip aneurysm in a 57-year-old women treated with a WEB SL device. (A) Early non-contrast MRI. (B) Mid-term non-contrast MRI. (C) Early contrast-enhanced MRI. (D) Mid-term contrast-enhanced MRI. Note the occurrence of a hyperintense thrombus in the non-WEB-carrying dome but only slight signal increase inside the WEB.
Early morphological outcome
Table 2 summarizes the morphological data of all patients included in our study, showing the ROI data for pre- and post-contrast media application and the accompanying relative quantitative signal intensity values. The signal intensities within the WEB were very low and increased slightly after contrast administration. The signal intensities in the compartment of the aneurysm dome distal to the WEB implanted (if present) are also shown. In the early phase only one examination revealed a native T1-weighted hyperintensity here (1/25, 4%). In almost all patients (24/25, 96%) additional wall enhancement of the WEB-treated aneurysm in the post-contrast images was observed.
Mid-term morphological outcome
Table 3 summarizes the mid-term follow-up data for all patients included in our study, showing data concordant to table 2. In 3/25 cases (12%) with a residual dome distal to the WEB a hyperintense thrombus occurred; an example is shown in figure 2. The signal intensity within the WEB remained equally low and showed a faint increase after administration of contrast media. The initially observed wall enhancement of the WEB-treated aneurysms had disappeared in the majority of cases.
In vitro imaging results
The ROI within the WEB lumen placed in the aneurysm model perfused with gadolinium-containing water showed signal intensities similar to values measured for air, consistent with a near-complete signal loss. There were normal signal values even in the direct vicinity of the WEB, which had been chosen to be undersized with regard to aneurysm size and therefore had the surrounding dome also filled with contrast medium/water. This is consistent with minimal local artifacts due to the nitinol mesh itself. Details are shown in figure 3.

(A) Thin slice multiplanar reformation of flat-panel CT (Vaso-CT) showing a WEB SLS 9 in an elastic aneurysm model filled with water (arrow indicates the aneurysm wall). (B) T1 TSE image of the elastic aneurysm model with region-of-interest measurements inside the WEB lumen (thick arrow), in the surrounding fluid (water containing gadolinium), and in the air outside the model box. Thin arrow indicates the aneurysm wall.
Evaluation of MRI signal intensity
At both imaging time points the MRI signal intensity within the WEB was very low overall and showed a slight increase after contrast administration. Non-parametric statistical testing using contrast media as the variable in initial and follow-up MRI showed no significant difference between ROI inside the WEB device at initial and follow-up MRI in either non-contrast (P=0.946) or contrast-enhanced imaging (P=0.377). In the initial MRI, comparison of ROIs prior to and after contrast application displayed a significant difference (P=0.008) whereas, in the follow-up MRI, the same comparison no longer showed a significant difference (P=0.107). The results are shown in table 4.
Data analysis applying a non-parametric test (Mann–Whitney U test)
Wall enhancement of the treated aneurysm occurred significantly more frequently in the initial MRI examinations (P<0.001; see tables 2 and 3). In cases where the WEB did not completely fill the aneurysm, a T1-hyperintense thrombus in the distal dome was a frequent observation in the mid-term MRI (see tables 2 and 3).
Discussion
This retrospective study analysed the short- and mid-term results of 25 WEB-treated patients with wide-neck intracranial aneurysms with multiparametric MRI. Special focus was on evaluating the value of MRI for assessment of early thrombus formation inside the WEB and to describe other valuable MRI findings beyond MRA. To verify intermodal correlation between CE-MRA and DSA prior to applying quantitative MRI measurements, aneurysm occlusion rates after WEB embolization were assessed separately for both initial and 6-month follow-up CE-MRA and DSA. Overall short- and mid-term follow-up showed complete occlusion rates of 84% initially and 76% at mid-term follow-up, which is consistent with previous publications, as is the agreement between the modalities.4 12 Since our objective in evaluating occlusion rates was not to reproduce the work of Timsit et al,12 inter-rater reliability testing was not performed.
No significant difference between the initial and follow-up MRI signal inside the WEB lumen was detected in either non-contrast or contrast-enhanced imaging using ROI analysis. To compare the values, structural ROIs were placed systematically in the center of the WEB device on identical slices of coronal fat-suppressed T1-weighted images. Since MRI images cannot be quantitatively compared absolutely, we used signal intensity of cerebrospinal fluid as a reference for normalization. Sizing of the ROI was dependent on the aneurysm dome size and chosen similarly for both non-contrast and contrast-enhanced images in all cases (see figure 2).
Imaging limitations in MRI are often caused by magnetic susceptibility artifacts and radio frequency shielding effects.12 16–18 The Faraday cage effect describes the phenomenon of blocking electromagnetic waves by a closed wire mesh capable of induction currents.12 19 Since the WEB device is constructed of electrically conductive material (braided nitinol mesh), it is likely to have some effect on the MRI signal, maybe even resulting in signal loss from the interior due to radio frequency shielding.12 20 A different phenomenon has been described for tubular neuroendovascular devices such as stents and flow diverters, in which the signal loss is mainly an effect of local susceptibility of the material itself.12
The occurrence of a hyperintense signal inside the aneurysm dome distal to the WEB on mid-term follow-up MRI as shown in figure 2 can be interpreted as a sign of methemoglobin-rich organized thrombus. In our cohort, this phenomenon did not occur within the WEB device, although one would expect a similar thrombus development here. This may be a strong hint for radio frequency shielding due to the WEB itself. This finding is confirmed by our in vitro experiment, which showed nearly complete signal loss from inside the WEB. On the other hand, the susceptibility artifacts due to the WEB material itself seem to be limited, which is supported by the in vitro experiment, but even more by the clinical data showing a transient enhancement of the aneurysm wall in the direct vicinity of the WEB. This enhancement might be an early sign of thrombus organization, which goes together with local inflammation and contrast enhancement. Contrast enhancement of early thrombus could serve as an explanation for the measured but fairly visible increase in signal intensity within the WEB, which was statistically significant in the early MRI. However, this observation does not indicate whether it represents residual flow within the WEB or early thrombus formation.
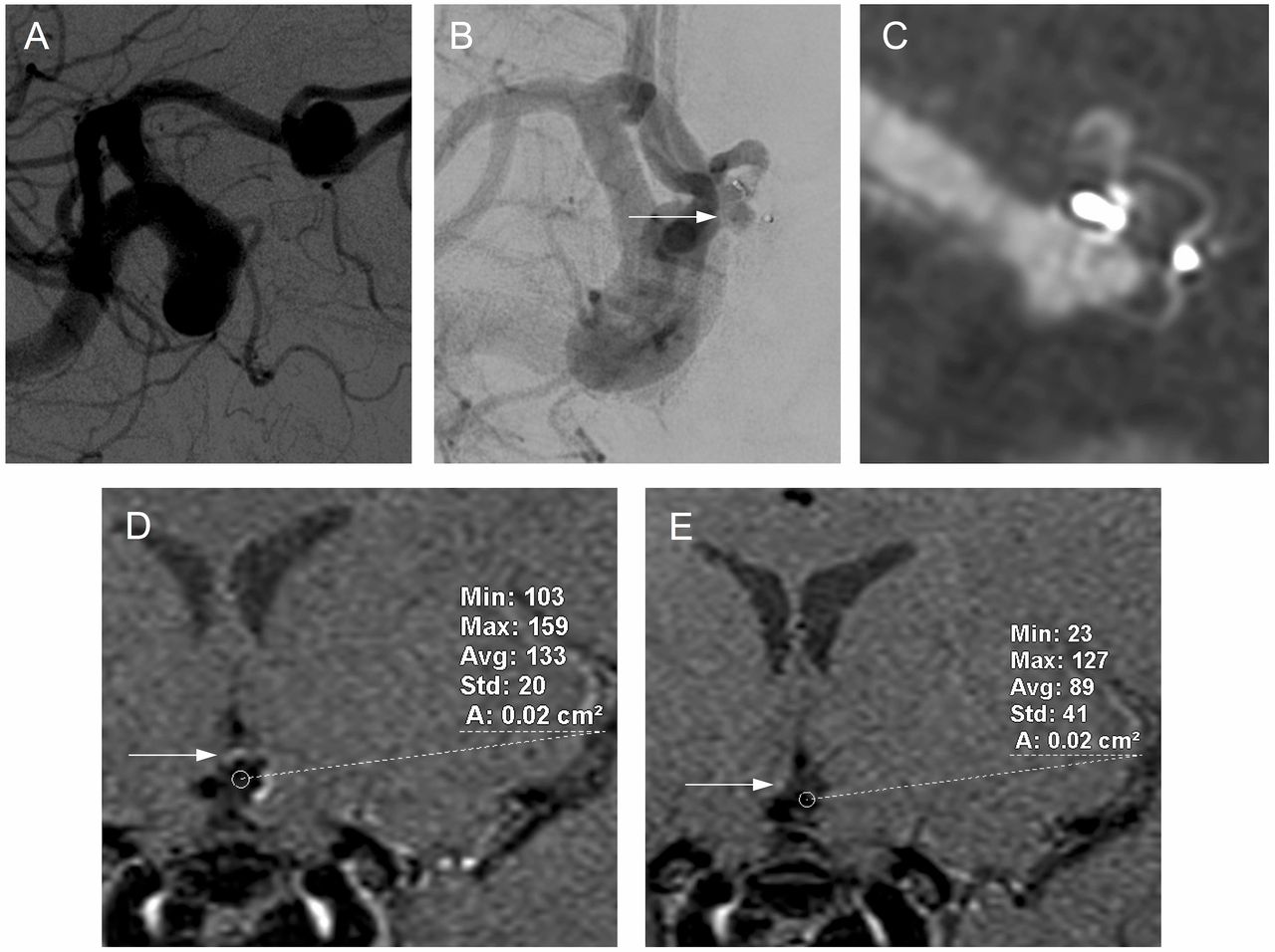
Based on our evaluation using ROI analysis in an elastic aneurysm model and in the patient series, we consider the WEB to be a device capable of strong radio frequency shielding, making it impossible to evaluate the conditions inside the device by angiographic or morphological MRI techniques. As shown above (figure 4), changes inside the WEB lumen, which are clearly visible on DSA, become undetectable on CE-MRA and morphological MRI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidental anterior communicating artery (Acom) aneurysm in a 47-year-old woman treated with a WEB SL 6×4. (A) Pretreatment digital subtraction angiogram (DSA) showing a regular shaped wide-necked Acom aneurysm. (B) Six-month follow-up DSA showing complete occlusion of the intracranial aneurysm with opacification of the proximal recess of the device (arrow), confirmed by multiplanar reformation of the three-dimensional rotational angiogram, additionally showing inflow in the slightly tilted WEB at the level of the aneurysm neck (C). (D) Early contrast-enhanced MRI showing region of interest (ROI) inside the WEB lumen and wall enhancement (arrow). (E) Mid-term contrast-enhanced MRI showing ROI inside the WEB lumen and almost no wall enhancement (arrow). The partial opacification of the WEB was not visible on MR angiography or in morphological MRI.
In order to obtain stable anatomical/clinical results and continuous technical improvement,6 20 21 the WEB device needs a suitable method for follow-up examinations in daily clinical use.15 22 Some recommendations in this regard have already been published—for example, Mine et al compared DSA and CE-MRA for the follow-up of intracranial aneurysms treated with the WEB-DL. They found that CE-MRA alone is not sufficient for detection of inadequately occluded intracranial aneurysms, however the examined cohort comprised only 15 patients.4 Timsit et al 12 also postulated that follow-up with CE-MRA and 3D-TOF MRA after WEB device treatment is not satisfactory for the detection of aneurysm remnant due to signal loss in MRA, and DSA remains the criterion standard for follow-up. All these methods seem sufficient to depict a relevant relapse but none of the methods—apart from DSA—would be suitable to confirm stable early thrombus formation within the WEB. Since MRI seems incapable, the one option left is flat-panel computed tomography (FP-CT). Caroff et al 10 reported on the use of low-contrast FP-CT for displaying the structure of the implant as well as the central filling. This examination can either be performed acutely on the table using diluted intra-arterial contrast or, similar to conventional CT angiography, applying intravenous contrast injection. It is also feasible on an outpatient basis. Image quality with current systems can be expected to be sufficient to reliably confirm persistent opacification or show occlusion of the lumen of the WEB device.
Study limitations
A ROI-based evaluation may always be considered as susceptible to heterogeneities to the measured structure and imaging artifacts.23 This might have caused errors, especially with regard to the smaller aneurysms included in the evaluation.
Unfortunately, we did not systematically perform FP-CT on the day of the baseline MRI. This might be an issue for a prospective follow-up study. However, in addition to the work by Caroff et al,10 our in vitro experiment provides an impression of how FP-CT performs.
Conclusion
Signal intensity measurements in multiparametric MRI suggest that neither CE-MRA nor morphological sequences are capable of revealing reliable information on the WEB lumen, presumably due to radio frequency shielding. MRI is therefore not suitable for confirming complete thrombus formation within the WEB.
References
Footnotes
Contributors Conception/design of work: J-HB. Data collection: J-HB. Data analysis and interpretation: J-HB, AF, JS. Drafting the article: J-HB. Critical revision of the article: J-HB, JS, AF, MB, JF. Final approval of the version to be published: J-HB, JS, AF, JF. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: J-HB, JS, AF, JF, MB.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.