Article Text

Abstract
Background Malignant brain edema (MBE) is a devastating complication in ischemic stroke. Data on MBE in patients who have had mechanical thrombectomy (MT) are relatively scarce.
Objective To investigate the incidence, predictors, and clinical outcomes of MBE in patients after MT.
Methods We included 130 consecutive patients after MT caused by anterior circulation large vessel occlusion stroke, treated with MT. MBE was defined as a midline shift of ≥5 mm on the follow-up imaging within 72 hours after MT. Characteristics of patients at admission and details of treatment were collected. The 90-day modified Rankin scale score was used as a measure of functional outcomes.
Results Of the 130 patients (age, 68.6±10.9 years; male, 50%), 35 (26.9%) patients developed MBE. The patients with MBE had a lower rate of functional independence (OR=7.831; 95% CI 1.731 to 35.427; p=0.008) and significantly higher mortality at 90 days (OR=7.958; 95% CI 2.274 to 27.848; p=0.001) than patients without MBE. In 104 (80%) patients with successful recanalization (modified Thrombolysis in Cerebral Infarction score of 2b–3), 24 (23.1%) patients exhibited MBE. After adjustment for confounding, ICA occlusion (OR=3.746; 95% CI 1.169 to 12.006; p=0.026) and worse collateral score (grade 1 vs grade 0: OR=0.727; 95% CI 0.192 to 2.753; p=0.638; grade 2 vs grade 0: OR=0.130; 95% CI 0.021 to 0.819; p=0.030) were significantly associated with the development of MBE, despite successful recanalization.
Conclusions MBE after MT is not uncommon and was related to poor functional outcomes. Localization of a vessel occlusion and collateral status may play a role in the development of MBE.
- stroke
- thrombectomy
- complication
Statistics from Altmetric.com
Introduction
Recent landmark randomized controlled trials1–3 have validated the efficacy and safety of mechanical thrombectomy (MT) over medical treatment in patients with anterior circulation large vessel occlusion stroke (LVOS). However, a substantial proportion of patients still may not experience functional improvement in the real world.4 Several risk factors, including patients’ factors5 (older age, sex, or chronic brain damage) and periprocedural factors6 (anesthesia, intraprocedural vasospasm, or vessel injury), may contribute to poor functional outcomes despite successful recanalization of the occluded artery with MT. However, postprocedural malignant brain edema (MBE) may also play an important role in reducing the benefit of MT.
MBE after ischemic stroke is a serious condition.7 It can result in increased intracranial pressure, rapid neurologic deterioration, and cerebral herniation. MBE accounts for 10–78% of patients with all types of ischemic stroke, and the mortality rate in patients with MBE is nearly 80%.8 9 Although early studies10 11 showed that reperfusion can promote the development of brain edema, recent studies12 13 have indicated that successful recanalization might attenuate brain edema. However, to our knowledge, there is a paucity of data on the incidence and clinical outcomes of MBE in patients after MT.
Several randomized controlled studies14–16 have confirmed that early decompressive craniectomy (DC) is an effective treatment to reduce morbidity and mortality. Accordingly, early identification of patients at highest risk for development of MBE is important in therapeutic decisions. Prior studies17–19 have identified several predictive factors for the development of MBE in large hemispheric infarction with conservation treatments. These factors include the baseline National Institutes of Health Stroke Scale (NIHSS) score, hyperdense middle cerebral artery (MCA) sign, Alberta Stroke Program Early CT (ASPECT) score, and collateral score. However, whether there are independent clinical risk factors affecting the occurrence of MBE in patients after MT is unclear.
Therefore, in this study, we preliminarily investigated the incidence, predictors, and clinical outcomes of MBE caused by anterior circulation LVOS in MT-treated patients.
Methods
Participants
We enrolled patients who had undergone emergency endovascular treatment in Yijishan Hospital, Wannan Medical College between July 2014 and August 2018. The local ethics committee approved the study protocol. Patients were included if they fulfilled the following inclusion criteria: (1) time from onset to groin puncture (OTP) ≤8 hours; (2) baseline ASPECT score ≥6; (3) baseline NIHSS score ≥6 and pre-stroke modified Rankin Scale (mRS) score <2; (4) an LVOS in the internal carotid artery (ICA) or the M1 segment of the MCA, confirmed by computed tomographic angiography/magnetic resonance angiography/digital subtraction angiography (DSA); and (5) undergoing MT with stent retriever devices (Solitaire, Covidien, Irvine, California, USA). In line with previous studies,13 we excluded patients with parenchymal hemorrhage (PH).
Data collection
All consecutive patients were prospectively documented. This included demographics, medical history (hypertension, diabetes mellitus, and atrial fibrillation), laboratory measures, NIHSS score, the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification, procedural factors (ASPECT score, leptomeningeal collaterals, and occlusion site) and outcomes.
For all enrolled subjects, the imaging characteristics were evaluated by two neurologists/interventionalists, who were blinded to the clinical information. According to previous studies, patients with MBE were defined as those with: (1) parenchymal hypodensity of at least 50% of the MCA territory and signs of local brain swelling such as sulcal effacement and compression of the lateral ventricle and (2) midline shift of ≥5 mm at the septum pellucidum or pineal gland with obliteration of the basal cisterns.13 In these patients, midline shift was measured on the follow-up imaging within 72 hours after MT. Patients with MBE were assessed as dichotomous (present or absent). In the present study, collateral circulation was assessed based on retrograde contrast opacification of vessels within the occluded territory on delayed DSA images. The collateral score was classified as follows20: grade 0 was assigned if there was little or no significant reconstitution in the territory of the occluded vessel or less than one-third of the occluded territory, grade 1 was assigned if the collaterals reached less than two-thirds of the occluded territory, and grade 2 was assigned if the collateralization reached more than two-thirds of the territory or the proximal main stem.
Procedural characteristics, including OTP, time from onset to recanalization, and passes of the retriever, were recorded by the operators for patients undergoing MT. Vessel recanalization was graded according to the modified Thrombolysis in Cerebral Infarction grading system. Successful recanalization was defined as a score of 2b or 3.
Functional outcomes were assessed with mRS at 90 days after onset, with a good functional outcome being defined as an mRS score of 0–2 and a poor functional outcome as an mRS score of ≥3. A 90-day mRS score of ≤2 was considered to be functional independence.
Statistical analysis
Patients were divided into the MBE and non-MBE groups, or good and poor outcomes. Continuous variables (age, blood pressure, NIHSS score, ASPECT score, OTP, onset to recanalization, and laboratory measures) are presented as the mean ±SD or as the median (IQR). Categorical variables (gender, occluded site, collateral score, and vessel recanalization) are presented as percentages. Continuous variables were analyzed using the Mann-Whitney U test. Categorical variables were analyzed using the χ2 test and the Fisher exact test, as appropriate. The association between MBE and clinical outcome or mortality at 90 days was analyzed with a binary logistic regression analysis. In addition, a binary logistic regression analysis was performed to analyze the association of the factors and the presence of MBE. Variables with a p value <0.1 from the univariate analysis were entered into the logistic regression analysis. ORs and 95% CIs were calculated. For all analyses, a two-tailed value of p≤0.05 was considered significant. All statistical analyses were performed using the SPSS software package.
Results
Baseline characteristics
Mean age of the 130 included patients was 68.6±10.9 years, 65 (50%) were men, the mean OTP was 258.7±74.9 min, the median baseline ASPECT score was 8 (IQR 8–9), and the baseline NIHSS score was 16 (IQR 14–20). Successful recanalization was achieved in 104 (80%) patients. All eligible patients underwent a 90-day follow-up. Of them, 61 (46.9%) patients had 90 day functional independence and 27 (20.8%) died. The baseline characteristics of the patients with MBE and without MBE are listed in table 1.
Demographics and baseline characteristics stratified by the presence of malignant brain edema
Incidence and factors associated with malignant brain edema
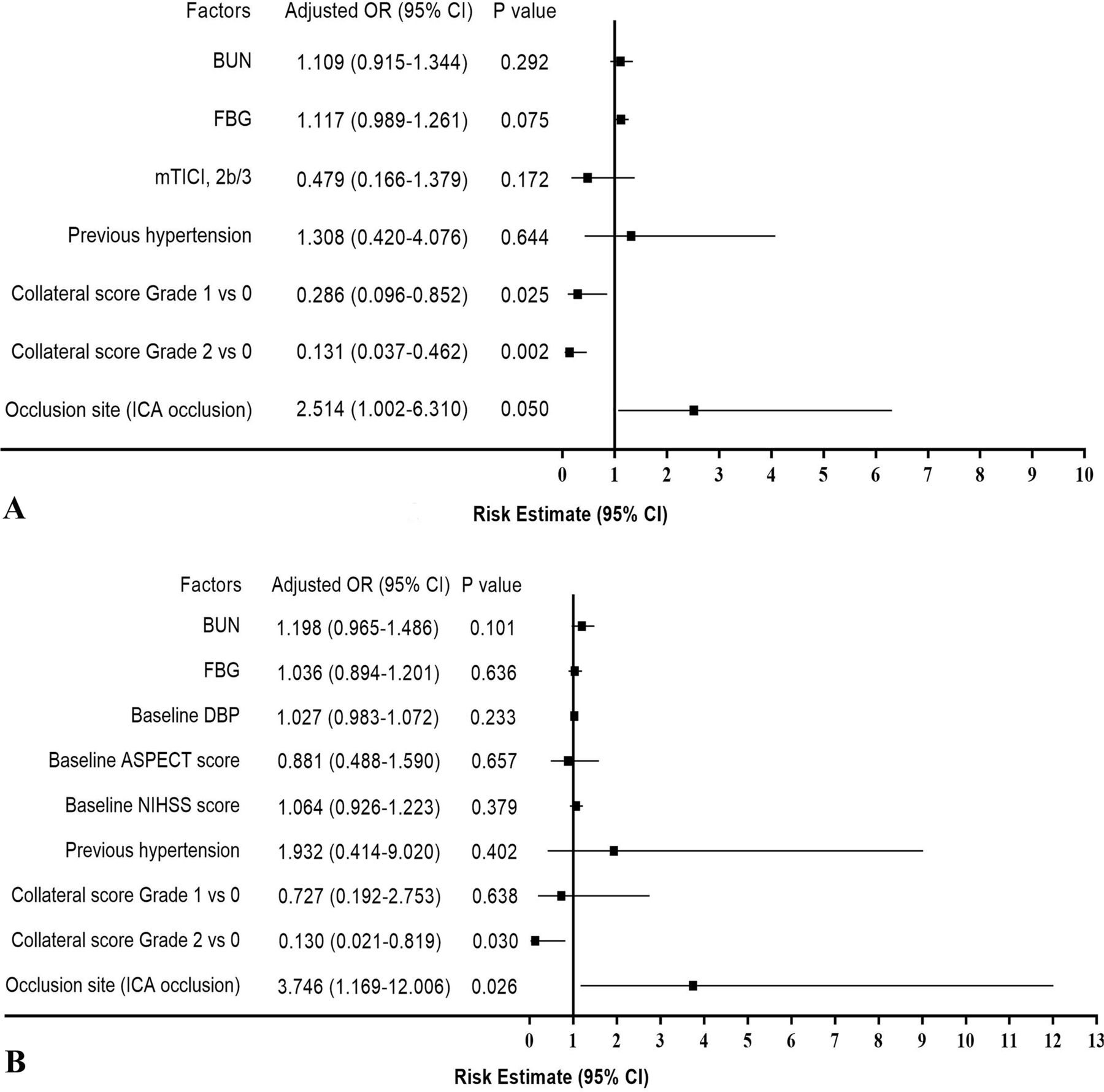
Among the enrolled patients, 35 (26.9%) developed MBE. A study of the baseline characteristics (table 1) shows that patients with MBE had significantly higher rates of ICA occlusion (62.9% vs 32.6%, p=0.002), a lower rate of recanalization (68.6% vs 84.2%, p=0.048), a worse collateral score (grade 0, 48.6% vs 13.7%; grade 1, 37.1% vs 41.1%; grade 2, 14.3% vs 45.3%; p<0.001), and higher levels of admission fasting blood glucose (FBG; 8.70±4.17 mmol/L vs 6.87±3.23 mmol/L; p=0.001) and blood urea nitrogen (BUN; 6.92±2.84 mmol/L vs 5.84±2.03 mmol/L; p=0.034) than non-MBE patients. After adjustment for confounding factors (the history of hypertension, collateral score, recanalization, occlusion site, FBG, and BUN), we found that the site of occluded vessels and collateral score may be associated with the presence of MBE in patients after MT. Compared with the proximal MCA occlusion, ICA occlusion (OR=2.514; 95% CI 1.002 to 6.310; p=0.050; figure 1A) was associated with an increased likelihood of having MBE. However, the statistical significance is borderline. In addition, good collateral circulation was associated with a reduced likelihood of having MBE (grade 1 vs grade 0: OR=0.286; 95% CI 0.096 to 0.852; p=0.025; grade 2 vs grade 0: OR=0.131; 95% CI 0.037 to 0.462; p=0.002; figure 1A).

Odds ratios (OR) for the development of malignant brain edema (A) in all enrolled patients (n=130), and (B) in patients with successful reperfusion (n=104). ASPECT, Alberta Stroke Progam Early CT; BUN, blood urea nitrogen; DBP, diastolic blood pressure; FBG, fasting blood glucose; ICA, internal carotid artery; mTICI modified Thrombolysis in Cerebral Infarction; NIHSS, National Institutes of Health Stroke Scale.
Then, we investigated the occurrence of MBE in patients with successful recanalization after MT (n=104). Of these patients, 24 (23.1%) exhibited MBE. Significant variables in the univariate analysis were entered into the multivariate logistic model (details are provided in online-only supplementary table 1). After adjustment for confounding factors (history of hypertension, collateral score, occlusion site, baseline diastolic blood pressure, baseline NIHSS score, baseline ASPECT score, FBG, and BUN), we found that the localization of occluded vessels (ICA occlusion vs MCA occlusion: OR=3.746; 95% CI 1.169 to 12.006; p=0.026) and collateral score (grade 1 vs grade 0: OR=0.727; 95% CI 0.192 to 2.753; p=0.638; grade 2 vs grade 0: OR=0.130; 95% CI 0.021 to 0.819; p=0.030; figure 1B) were associated with the presence of MBE.
Supplemental material
Malignant brain edema and functional outcomes
In the univariate analysis, patients with MBE had functional independence less often than patients without MBE (20% vs 56.8%, p<0.001). Moreover, there was a significantly higher mortality rate in the MBE group than in the non-MBE group (48.6% vs 10.5%, p<0.001). The distribution of mRS scores of 0–6 at 90 days is shown in figure 2.

{kind=link}
{kind=link}
Distribution of modified Rankin Scale (mRS) scores at 90 days according to the presence of malignant brain edema (MBE).
In addition, of the 35 MBE patients, DC was performed in 5 (14.3%) patients. Significant variables in the univariate analysis were entered into the multivariate logistic model (details are provided in online-only supplementary tables 2–5. The presence of MBE (OR=7.831; 95% CI 1.731 to 35.427; p=0.008; table 2) was inversely associated with good 90-day functional outcomes after adjusting for the age, history of atrial fibrillation, baseline NIHSS score, baseline ASPECT score, stroke cause, occlusion site, collateral score, passes of retriever, DC, and degree of recanalization. Furthermore, there was a significant correlation between the presence of MBE (OR=7.958; 95% CI 2.274 to 27.848; p=0.001; table 2) and 90-day mortality after adjusting for age, the history of atrial fibrillation and hypertension, baseline ASPECT score, stroke cause, occlusion site, collateral score, DC, and degree of recanalization.
Multivariable analyses between malignant brain edema and 90-day outcomes
Discussion
In this study, we investigated the incidence, risk factors, and related outcomes of MBE in patients after MT caused by anterior circulation LVOS. The main findings were as follows. First, MBE was not uncommon in patients after MT. But successful recanalization may reduce the occurrence of postprocedural MBE. Second, ICA occlusion and worse collateral score may be independent predictors of the development of MBE, despite successful recanalization after MT. Third, the presence of MBE indicated a reduced chance of good functional outcomes and an increased mortality rate at 90 days.
According to previous studies, MBE occurs in approximately 10–78% of all patients with hemispheric stroke.8 9 In addition, several studies also investigated the incidence of MBE in patients after intravenous thrombolysis (IVT). Strbian et al 21 reported that cerebral edema accounts for 28% of thrombolysis-treated patients with ischemic stroke. Research into a large sample of patients after IVT showed that 22.7% (9579/42 187) patients developed cerebral edema.22 In the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) cohort, the rates of midline shift were nearly 50% of patients in the IVT group.13 However, the data concerning MBE in patients after MT is limited. Initially, Davoli et al reported that in patients with LVOS undergoing MT, 35.7% (35/98) patients developed malignant MCA infarction.23 Then, Kimberly et al indicated that almost 44% of patients in the MT group developed midline shift.13 Our results showed that 26.9% of patients developed MBE after MT. At first glance, our results seem to differ from previous studies. However, an important reason for this is the heterogeneity of the enrolled patients and the evaluated methods of cerebral edema in different studies. Although the incidence of MBE after MT was unclear, we considered that MBE may be a common condition in patients who have undergone MT.
Persistent large vessel occlusion is related to a higher risk of MBE. Thus, early restoration of blood flow to ischemic tissue might prevent the development of MBE. However, several studies have shown that revascularization may cause secondary reperfusion brain edema.10 11 Contrary to these studies, we found that patients with MBE had a significantly a lower rate of recanalization (84.2% vs 68.6%, p=0.048; table 1), which implies that successful recanalization may attenuate the development of MBE. These results are consistent with the results of recent studies.12 13 An investigation,12 based on the Echoplanar Imaging Thrombolysis Evaluation Trial (EPITHET) and Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy (MR RESCUE) cohorts, showed that a greater reperfusion percentage was associated with decreased brain edema. Kimberly et al found that successful recanalization was related to a reduced midline shift.13 In addition, a large systematic review, including 38 studies (3278 patients), indicated that successful recanalization could reduce the risk of MBE.8 Taken together, we speculated that the benefits of vessels recanalization after MT were associated with the rescue of hypoperfused brain tissue at risk of infarction, and also related to limiting edema-associated brain injury.12 13
However, it should be noted that even in patients with successful recanalization, more than 20% of patients still developed MBE. Although the specific mechanisms of MBE in these patients are unclear, identification of associated clinical variables is important to identify potential therapeutic targets for treatment development. Our results showed that ICA occlusion and worse collateral score may be independent risk factors for the development of MBE after MT, especially in patients with successful reperfusion.
Several mechanisms could explain the results. First, collateral circulation plays a pivotal role in the pathophysiology of ischemic stroke.24 Poor collateral blood vessels are known to augment the progression of the infarct core, which is associated with brain edema.25 26 Second, ICA occlusion may predict less collateral flow supplied by the anterior cerebral artery (ACA) or anterior communication artery. Therefore, even in patients with successful reperfusion, the rate of developing MBE in ICA occlusion was higher than in MCA occlusion. Walcott et al reported that in MCA infarction, ACA involvement contributes to mortality as a mediator of collateral circulation.27 Similarly, Shimoyama et al found that imaging ACA territory involvement was a reliable predictor of the risk of fatal brain edema in MCA ischemic stroke.19 Third, ICA occlusion was an independent predictor of ACA emboli during thrombectomy,28 which resulted in extensive infarction and collateral flow damage. Therefore, the site of occluded vessels and collateral circulation may play a crucial role in determining the development of MBE after MT.29 Notably, in patients with MT, regardless of the recanalization levels, our results showed that ICA occlusion (OR=2.514; 95% CI 1.002 to 6.310; p=0.050) may be associated with an increased likelihood of developing MBE. However, the statistical significance is borderline. We considered that this might be related to our small sample size.
The association of cerebral edema with poor clinical outcomes or death in stroke has been well established.9 Similarly, this study indicated that approximately 50% of patients with MBE died. Furthermore, multivariate analysis showed that the presence of MBE predicts a reduced chance of good functional outcomes and an increased mortality rate at 90 days. Fortunately, several randomized controlled studies14 15 have confirmed that early DC is an effective treatment to reduce morbidity and mortality for patients with MBE. Accordingly, understanding the mechanism and finding interventional predictors of MBE after thrombectomy may improve the benefits of MT. Our results may assist in the selection of patients to prevent the development of MBE.
This study also has some limitations. First, similar to previous studies,13 we excluded patients with PH (PH1 and PH2). Thus, selection biases might have occurred, because of coexisting edema and hemorrhage in some patients. Second, it is an observational study based on retrospective analysis. Missing and unknown data might have influenced the results. Third, our study included only a subset of patients who were eligible for MT according to current guidelines. Hence, the results cannot be generalized to other patients, such as patients with lower ASPECT scores. Finally, this study was a single-center, small sample size study, so the validity of our results cannot be categorically confirmed. A multicenter prospective study including more clinical risk factors will be required to confirm our results. However, to our knowledge, we are the first group to investigate the course of MBE in patients after MT.
Conclusions
In patients undergoing MT owing to anterior circulation LVOS, the presence of MBE indicated a reduced chance of good functional outcomes and an increased mortality rate at 90 days. Localization of a vessel occlusion and collateral status may be important predictors for MBE in patients with successful reperfusion. This study may assist in the selection of patients to prevent the development of MBE.
References
Footnotes
XH and QY contributed equally.
Contributors XH, QY, and ZZ: study design. XS and XX: data acquisition. LG and XD: image analysis. XH and QY: primary manuscript writing. ZZ: critical revision and final approval of the manuscript.
Funding This work was supported by the National Natural Science Foundation of China grant number 81701061.
Competing interests None declared.
Ethics approval The study was approved by the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.