Article Text

Abstract
Objective To describe the results in patients treated with the Surpass Evolve (SE) device, the new generation of Surpass flow diverters.
Methods Twenty-five consecutive patients (20 women, average age 58 years), with anterior or posterior circulation aneurysms treated with SEs in two early-user centers, were included. Device properties and related technical properties, imaging and clinical follow-up data, and intraprocedural, early (<30 days) and delayed (>30 days) neurological complications, further divided into minor (silent/non-permanent) and major (permanent) complications, were recorded and analyzed.
Results Twenty-nine SEs were successfully implanted in all subjects to treat 26 aneurysms using an 0.027" microcatheter with an average of 1.2 stents per patient. No intraprocedural thromboembolic or hemorrhagic complications were seen. At clinical follow-up, 24/25 (96%) patients had a modified Rankin Score of 0–2. Mortality was 0%. Imaging follow-up, available in 22/25 (88%) patients (median follow-up time 4 months), showed a complete aneurysm occlusion in 13/23 (57%) imaged lesions. Minor, transitory neurological deficits were recorded in 5/25 (20%) patients. One (4%) major complication was seen in one patient (4%) with a left-sided hemispheric stroke on postprocedural day 4 due to an acute stent thrombosis.
Conclusions Preliminary experience in patients demonstrates a good performance of the SE. This newly designed implant maintains the engineering characteristics of Surpass flow diverters, including precise placement due to its lower foreshortening and a high mesh density, yet can be deployed through a significantly lower-profile delivery system.
- aneurysm
- flow diverter
- stent
Statistics from Altmetric.com
Introduction
Flow diverters (FDs) are a well-established treatment for selected intra- or extracranial aneurysms.1 2 Their safety and efficacy have been demonstrated in large and giant anterior circulation aneurysms, sidewall aneurysms of <12 mm, distal lesions, and selected ruptured aneurysms.3–8
The Surpass Streamline (SS, Stryker Neurovascular, Kalamazoo, Michigan, USA) became the second FD to receive Food and Drug Administration approval following positive results from the SCENT trial.9 10 The implant has the unique characteristic of maintaining consistently high pore density across the aneurysm neck, irrespective of parent artery tortuosity, and within a wide range of vessel diameters. However, owing to the implant construct and number of wires used (72 or 96, depending on the device diameter), its 3.7 F microcatheter delivery system requires a triaxial access, potentially making navigation in tortuous intracranial anatomies or distal locations challenging.11 12 The Surpass Evolve (SE) represents the new generation of the Surpass FD. It has a lower profile while maintaining an important flow-diverting effect.13 Changes to the implant and a completely redesigned delivery system allow for easier navigation and deployment through a lower profile (2.7 F) microcatheter, similar to other commercially available FDs.
We describe our clinical experience and technical nuances in the first-time use of the SE in patients with aneurysms.
Methods
Patients and data collection
This prospective study, approved by local institutional review boards, involved two institutions. Adult subjects with anterior or posterior circulation wide-neck (>4 mm) saccular or fusiform aneurysms were treated using the SE FD, irrespective of prior treatments. Acutely ruptured and distal aneurysms were not treated with this device. Patients were adjudicated for FD treatment by a multidisciplinary team of neuroradiologists, neurosurgeons, and neurologists. Clinical data, aneurysm characteristics, and number and size of FDs used were recorded. Aneurysms were morphologically classified as saccular or fusiform and according to their maximum diameter, as in the SCENT study,9 into small (<10 mm), large (10–25 mm), or giant (>25 mm). Neurological complications were divided into intraprocedural, early and delayed if they occurred during, within and after 30 days of the procedure, respectively. These events were considered minor if they were silent (noticed only on imaging) or transient, and major if they resulted in a permanent neurological deficit. Clinical status was evaluated during the hospitalization and at discharge using the modified Rankin scale (mRS). Symptoms secondary to thrombosis-related inflammation of giant aneurysms or access-related complications were also recorded. Follow-up imaging was obtained with CT angiography (CTA), MR angiography (MRA), or DSA, according to institutional policies or clinical needs. A follow-up phone call was made at 7 and 30 days postprocedure and an office visit was performed at the time of follow-up imaging.
Procedural strategy
Procedures were performed under general anesthesia by three authors (VMP, TK, HR) with extensive experience with FDs and SS for the treatment of aneurysms. Dual antiplatelet therapy (aspirin and either ticagrelor or Plavix (clopidogrel)) was initiated 3 days before the procedure and continued for at least 6 months. Intravenous heparin was administered intraoperatively and titrated to maintain an activated clotting time between 250 and 300 s. For femoral access, an 0.088" guiding sheath was placed in the internal carotid or subclavian artery. A 115 cm 0.058" Catalyst 5 (Cat 5, Stryker Neurovascular, Michigan, USA) was used as intermediate catheter. For radial access, a 0.071" guiding catheter was navigated into the parent vessel and a Phenom+ (Medtronic, Irvine, California, USA) used as intermediate catheter. An 0.027" XT-27 microcatheter was placed distal to the aneurysm and used to deliver the FD. The treatment strategy was to deploy a single FD, but if multiple implants were indicated, devices were telescopically deployed from distal to proximal. Adjunctive coils were placed according to operator preference. Correct FD wall apposition was confirmed by VasoCT. Patients with no complications were discharged after 24 hours of observation.
Surpass Evolve device
As for the SS,11 12 the SE is a single-layer, self-expanding, braided implant made of a cobalt–chromium alloy with 12 platinum–tungsten wires for visualization. The SS is made of 48, 72, and 96 wires for its 2.5, 3 or 4, and 5 mm diameters, respectively, whereas the SE is manufactured with 48 and 64 wires for its 2.5 and 3.25–5 mm diameters, respectively. This generates a lower-profile implant and allows deployment through a 0.027" microcatheter, similarly to other available FDs. The device maintains its high mesh density of 15–30 pores/mm2 and a uniform rhomboid cell shape, independent of its postdeployment state, through optimization of the braid angle. The delivery system has been completely redesigned. The FD comes premounted on a stainless-steel delivery wire and packaged preloaded into an introducer sheath. Operators experienced some difficulty in flushing sheaths of 5 mm implants. The distal end of the FD is protected by a Teflon 'petal' that opens once the implant is released from the XT-27. Two markers on the delivery wire indicate the ends of the device, and a third marker allows the operator to visualize the resheathing limit. Resheathing is possible until 90% of the implant has been deployed. There is a soft, radio-opaque 15 mm long distal tip wire. The FD comes in 2.5–5 mm sizes, with a maximum expansion up to 0.2 mm beyond its nominal diameter (figure 1). Maximum length is 40 mm, and the implant foreshortens more than the SS but less than the Pipeline Flex (Medtronic, Irvine, California, USA).

New Surpass Evolve (SE) flow diverter implant. (Reproduced with permission from Stryker Neurovascular.) (A) Artist’s rendition of the SE device in the introducer sheath (left) and deployed (right). (B) Schematic drawing of the SE delivery system and its components: (1) delivery wire; (2) proximal marker; (3) resheath pad; (4) resheath marker; (5) SE; (6) petal; (7) distal marker; (8) distal tip; (9) introducer sheath.
Technical nuances
The SE is a self-expandable FD with high radial pressure (6 mm Hg). The distal end starts expanding as soon as it exits the microcatheter and is freed from the petal, which is identified by the distal marker. The distal part of the implant expands to its nominal diameter after unsheathing approximately 10–15 mm. Operators noted excellent pushability within the introducer sheath and ease of device expansion, which required only minimal forward pressure on the pusher wire. If expansion was incomplete at first attempt, the device could be recaptured and then partially redeployed in order to ensure a complete separation of its distal end from the petal. This feature allows the operator to accurately place the implant and anchor it to the vessel wall. At this point, further unsheathing of the SE is obtained by combining a forward push of the delivery wire and unsheathing of the microcatheter. During deployment, the delivery system needs to be adjusted and kept in the center of the artery. To ensure appropriate wall apposition, especially when about half of the FD has been deployed, operators 'loaded' the system—that is, concurrently pushed the wire and microcatheter gently to facilitate full expansion of the device. This constant forward force could potentially lead to an unwanted advancement of the implant past its intended distal landing zone. This could be challenging, particularly in tortuous anatomies and short distal landing zones with adjacent branching arteries. If the device had not been deployed past the recapture pad (second radio-opaque marker), it could easily be resheathed by advancing the XT-27 while keeping a very gentle traction on the wire. This maneuver can be performed up to three times according to the manufacturer's specifications. Once satisfactory positioning and expansion have been accomplished, the SE can be fully deployed by unsheathing the delivery wire. Vessel wall apposition can be improved by advancing the microcatheter over the delivery wire, or both as a system, within the deployed implant or by balloon-plasty. If placement of a second device in a telescoping fashion is needed, the delivery wire can be used to maintain access through the implant, allowing advancement of the microcatheter to deploy further devices. The wire demonstrated excellent stability for both FD resheathing and microcatheter readvancement.
Results
Our study included 25 subjects treated for 26 aneurysms between April and October, 2019. Patient and aneurysm characteristics are detailed in table 1. Twenty of 25 (80%) subjects were women and the average age was 58 years (range 36–86 years). Twenty-four aneurysms (24/26, 92%) were in the internal carotid artery (ICA): one (4%) in the cervical segment, 4/26 (15%) in the cavernous segment, 17/26 (65%) in the paraophthalmic segment, and 2/26 (8%) in the communicating segment. One lesion (4%) was in the A1 portion of the right anterior cerebral artery and one (4%) involved the right vertebrobasilar junction. Fifteen of 26 aneurysms (58%) were small, 8/26 (31%) were large, 2/26 (8%) were giant, and one (4%) was fusiform and partially thrombosed. Mean aneurysm diameter was 11 mm (range 3–30 mm). One aneurysm had previously ruptured and was partially coiled in the acute phase, and one had been previously coiled electively without complete neck coverage.
Patients, aneurysms, and implant characteristics
The SE could be advanced easily in the XT-27 in all cases, including long devices (5×40 mm), and there was no device twisting. Twenty-nine stents were deployed in 25 patients (average 1.2 stents/case). Resheathing and repositioning were performed successfully in 12/29 (41%) SEs and all FDs were successfully deployed in the desired location. In one patient, with two adjacent small paraclinoid aneurysms, one implant was used to treat two lesions. A fusiform, partially thrombosed vertebrobasilar aneurysm required treatment for increasing mass effect on the pons and worsening neurological status despite a functioning shunt; the patient was not a candidate for vessel sacrifice (single ectatic vertebral artery) or surgery. The SE was chosen for its long lengths and large sizes and for the need to perform the procedure transradially owing to pre-existing iliofemoral occlusion (figure 2).

Patient in their sixties with a partially thrombosed fusiform aneurysm of the right vertebrobasilar junction. (A) Non-enhanced head CT demonstrates a large, partially thrombosed aneurysm in the posterior fossa (arrow) exerting significant mass effect on the medulla. (B) Maximum intensity projection (MIP) reconstruction of a 3D rotational DSA of the right vertebral artery (VA) demonstrates the perfused lumen of the aneurysm. Note the small amount of contrast present in the superior aspect of the lesion within the thrombus (arrowhead). (C) Single shot acquisition shows the first Surpass Evolve (SE) after deployment. Note the excellent expansion of the distal (arrowheads) and proximal (arrows) ends of the implant. (D) Right VA road map demonstrates advancement of a second SE through the XT-27 (arrowhead: tip) that had been readvanced over the delivery wire of the previous SE; seen as a subtracted image (arrow). (E) Single shot acquisition after deployment of the four SEs used to bridge healthy segments of the basilar artery and right VA, entirely covering the aneurysm lumen. The XT-27 has been removed and the aneurysm is easily recatheterized with an SL-10 microcatheter over a hybrid microwire (arrow). (F) Single shot acquisition demonstrates a deployed Atlas laser-cut stent (arrow), used to ensure a good apposition of the distal SE scaffold. (G) MIP reconstruction of a VasoCT of the right VA. The SE scaffold covers the entire aneurysm. Note the Atlas stent within the proximal basilar trunk (arrowheads: Atlas markers). (H) Right VA DSA. Note the patent flow diverter construct and significant flow-diverting effect within the aneurysm through the venous phase (arrow).
In 7/25 (28%) patients postdeployment balloon-plasty was performed with a super-compliant balloon. In 2/25 (8%) patients with particularly tortuous anatomies, a laser-cut stent (Neuroform Atlas, Stryker, Kalamazoo, Michigan, USA) was deployed across the distal end of the SE to ensure optimal wall apposition. Postoperative VasoCT showed excellent wall apposition in all cases. Two patients (8%) received adjunctive coiling for a large and a giant supraclinoid ICA aneurysm. Average fluoroscopy time was 28.8 min (range 7.7–91 min). After FD deployment, one aneurysm (4%) showed no contrast filling (O’Kelly-Marotta (OKM) grade D), 12/26 (46%) showed persistent filling (OKM grade B), and 13/26 (50%) showed complete filling (OKM grade A), with 12 of these lesions showing contrast stasis in the venous phase (OKM grade A3, figure 3).
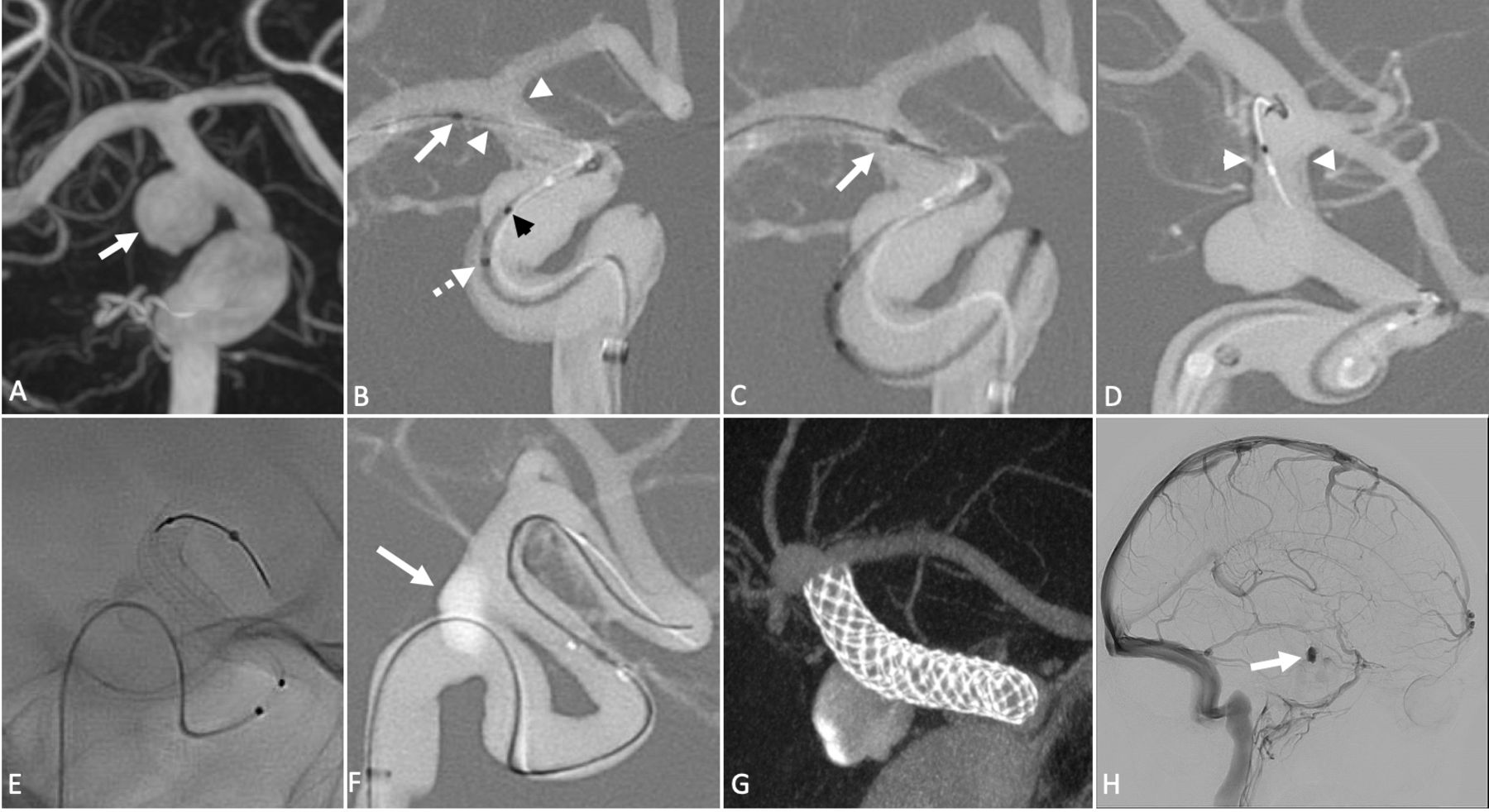
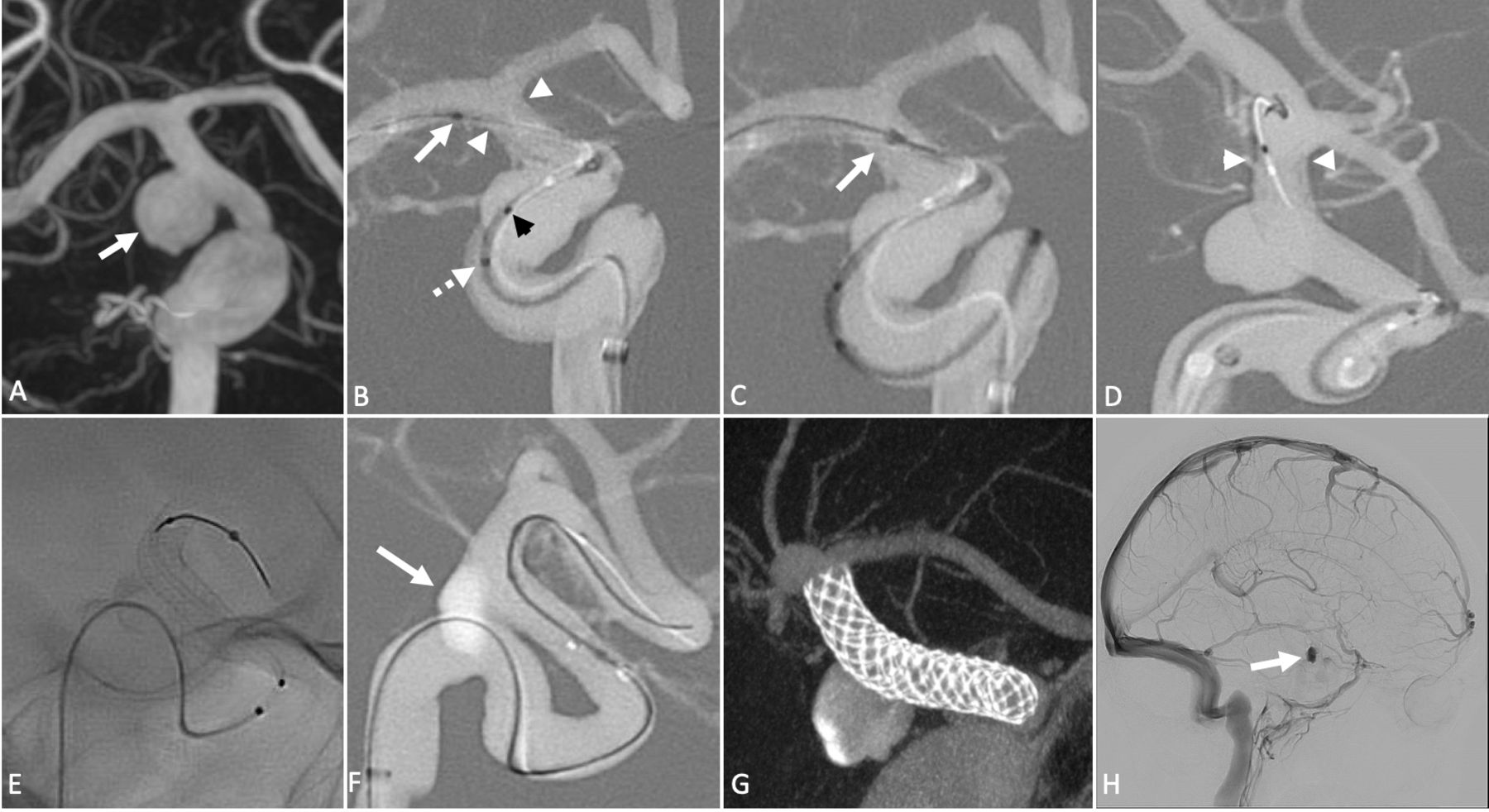
Septuagenarian patient with a right paraclinoid internal carotid artery (ICA) aneurysm. (A) Maximum intensity projection (MIP) reconstruction of a 3D rotational DSA of the right ICA demonstrates a laterally projecting wide-necked supraclinoid ICA aneurysm (arrow). (B) Right ICA road map during deployment of the Surpass Evolve (SE). Note the petal (arrow), the opened distal end of the SE (arrowheads), the resheath marker (black arrowhead), and the proximal marker (dotted arrow). (C) Resheathing of the SE for repositioning. The entire implant is recaptured past the petal (arrow). (D) Further unsheathing of the flow diverter (FD). Note the well-apposed distal end (arrowheads) and mild bulging of implant within the aneurysm. (E) Single-shot acquisition demonstrates a completely deployed SE The delivery wire is kept within the implant, to maintain access. (F) Recatheterization of the FD with a balloon over a microwire for postdilatation and to ensure complete wall apposition. Note significant contrast stagnation after SE deployment (arrow). (G) MIP reconstruction of a VasoCT of the right ICA. The SE is fully expanded and well apposed to the vessel wall, with minimal bulging at the aneurysm neck. (H) Right ICA DSA, lateral projection. Note significant flow-diverting effect with contrast stasis through late venous phase.
No intraprocedural complications occurred and 23/25 patients (92%) were discharged the day after the procedure. The patient with the fusiform vertebrobasilar aneurysm was kept in hospital for 5 days for shunt management, and a morbidly obese patient treated for a large cavernous ICA aneurysm required several days in the intensive care unit owing to the development of laryngeal cysts that made a safe extubation challenging. This patient was eventually discharged with mRS score 2. All other patients were discharged at baseline mRS score.
Follow-up
Clinical follow-up was available for all patients, and imaging follow-up was available in 22/25 (88%) patients, for 23 aneurysms. Median follow-up time was 4 months (range 5 days – 6 months). Imaging consisted of MRA and DSA (6/22, 27%), MRA alone (10/22, 45%), or CTA (6/22, 27%). table 2 summarizes follow-up data. At imaging, 13/23 aneurysms (57%) were completely thrombosed, 9/23 (39%) were partially thrombosed, and one lesion remained unchanged. All nine aneurysms that had follow-up at 6 months showed complete thrombosis (figure 4). At clinical follow-up, 24/25 patients presented with mRS score 0–2. Three patients (3/25, 12%) had early (<30 days) minor neurological complications. One patient with a previously coiled A1 aneurysmal remnant who had been treated with an SE deployed across the origin of the A1 had an episode of transient aphasia 4 days after the procedure and had a right caudate infarct on MRI. The patient who could not be extubated, treated for a large paraophthalmic aneurysm, had a silent internal capsule infarction detected with an MRI scan performed during hospitalization. Another patient treated for a large cavernous ICA aneurysm had a single, transient episode of monocular vision loss on the affected side. None of these patients had permanent neurological sequelae. One early major complication was seen in one patient (4%). The patient, who had been treated for a small saccular aneurysm, presented with a left-sided hemispheric stroke on postprocedural day 4 due to an acute FD thrombosis despite optimal dual antiplatelet therapy. This was the only complication with a long-term sequela as the patient required rehabilitation and continued to have an mRS score of 4. Mortality was 0%. One patient treated for a large cavernous ICA aneurysm had transient worsening of a pre-existing third nerve palsy, and a patient treated for a giant cavernous ICA aneurysm developed complete cavernous sinus syndrome. Both patients were treated with steroids and improved.
Follow-up data
{kind=link}
{kind=link}
{kind=link}
{kind=link}
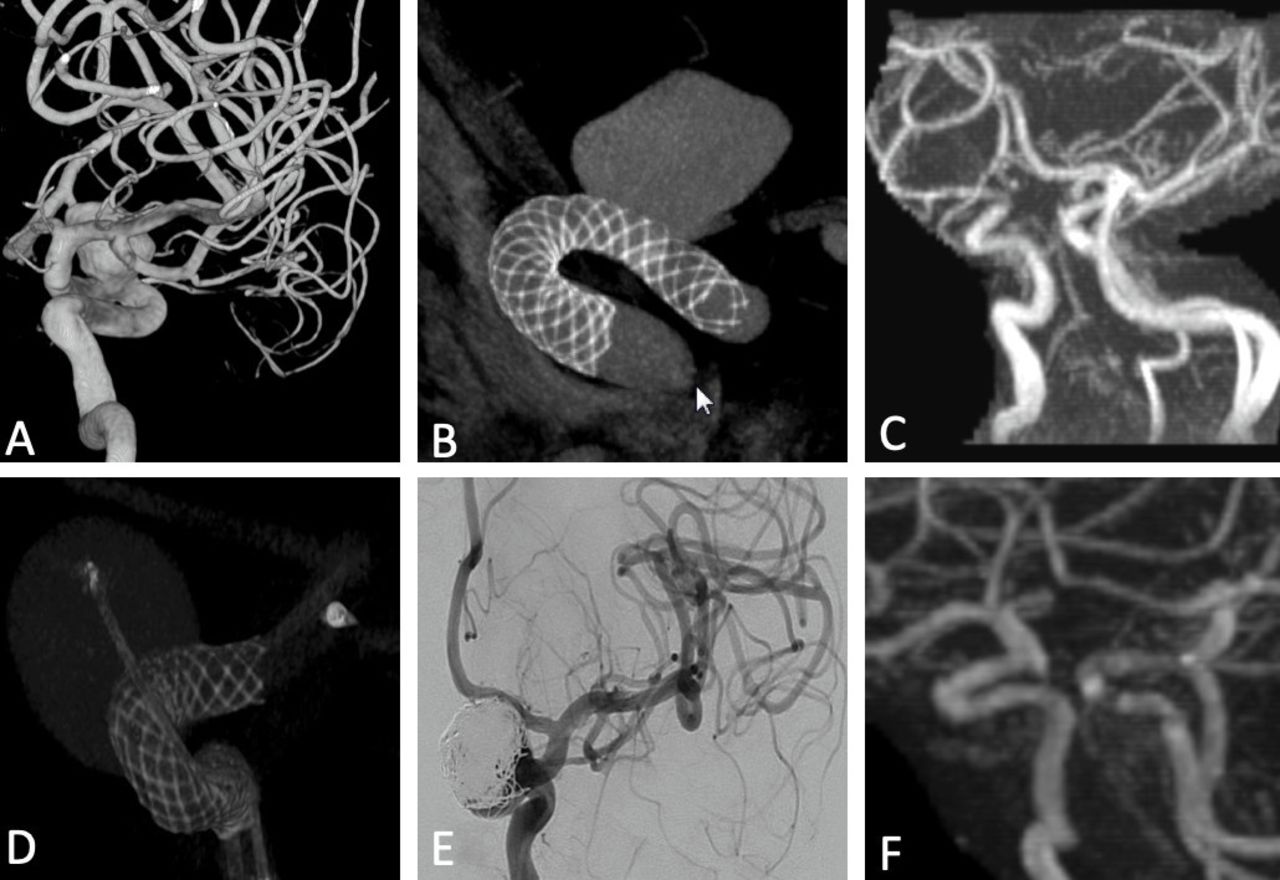
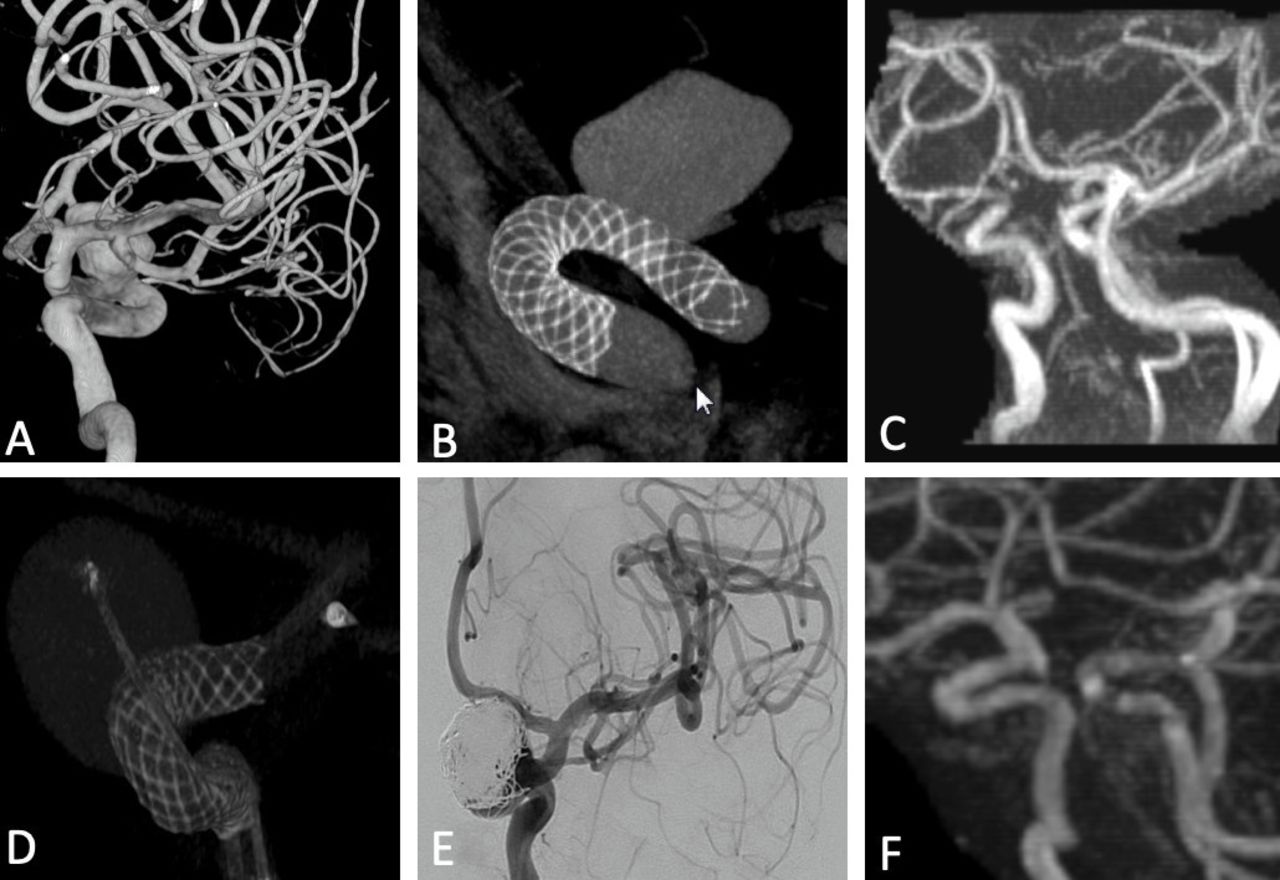
Examples of imaging at 6-month follow-up. (A) 3D DSA of the right internal carotid artery (ICA) in a patient in their 60s with an incidentally found paraophthalmic segment aneurysm and strong family history of subarachnoid hemorrhage. (B) VasoCT acquisition of the right ICA after positioning of a 5×20 mm Surpass Evolve (SE) across the aneurysm. Note the excellent wall apposition of the implant. (C) Six-month follow-up MRI. Note the complete thrombosis of the aneurysm with normal appearance of the vessel. (D) VasoCT of the right ICA after positioning of two SEs (4.5×20 mm; 4×25 mm) across the neck of an incidentally found paraophthalmic aneurysm in a patient in their 40s. Note the jailed microcatheter for adjunctive coiling of the lesion. (E) Right ICA DSA after deployment of six coils in the aneurysmal sac. Note the filling at the level of the aneurysm neck and base. (F) Six-month follow-up MRI. The aneurysm is completely thrombosed.
Two (8%) minor delayed neurological complications were seen in the 25 patients. One patient treated for a small paraophthalmic aneurysm noticed scotomas when ticagrelor was discontinued 6 months after treatment. These symptoms did not occur again after reinstating dual antiplatelet therapy. Another patient treated for a giant cavernous aneurysm with SE plus coiling had an asymptomatic ICA occlusion on follow-up imaging. Overall, 5/25 patients (20%) had minor neurological complications without permanent deficits. At follow-up imaging, covered side branches were widely patent in all but one patient.
Discussion
We report the first-in-human experience with the second generation of the Surpass FD, the SE. The device demonstrated excellent technical success rates in all cases, and good safety and efficacy. These results are promising and suggest that the FD will perform similarly to the SS, as reported previously in the SCENT trial and by Taschner et al, who showed a 98% technical success rate in both the anterior and posterior circulation, with a 62.8% 12-month aneurysm occlusion rate.9 14 The PUFS study demonstrated a 180-day aneurysm occlusion rate of 73.6%.15 We reported a 28% rate of postdeployment angioplasty, higher than that recently reported for Pipeline (5.6%).16 This probably reflects our extremely low threshold for performing angioplasty whenever suspecting incomplete FD apposition on VasoCT, given the demonstrated role of malapposition in delayed aneurysm healing.17 Rates of major neurological complications in the SCENT and PUFS trials were 8.3% and 5.6%, respectively. In our study, we recorded a 20% rate of minor complications without persistent morbidity and a 4% rate of major neurological complications. It needs to be specified that our results are not completely comparable to those of the above-mentioned trials because our patient population was more heterogeneous, as it included small wide-necked aneurysms following the positive results of the PREMIER study.3 The SCENT trial showed the need for fewer FDs to obliterate an aneurysm, with an average number of 1.1 SS/aneurysm, similar to our results (1.2 SE/aneurysm), whereas the average number of FDs employed in the PUFS trial was 3.1. The smaller number of FDs needed was probably secondary to the higher mesh density of the SS and to the availability of longer lengths and larger diameters than with the Pipeline. This, in contrast, results in a more complex delivery system. Owing to the high stiffness of the SS, many operators navigate a Cat 5 distal to the aneurysmal neck, frequently up to the M1 segment of the middle cerebral artery, in order to navigate the SS delivery system smoothly to the desired site.18 The main originality of the SE lies in the considerably smaller number of wires than with its predecessor (64 in the largest version vs 96 in a similarly sized SS). The lower profile of the implant when compressed and improvements in the delivery wire translate into the ability to deliver the device through a 2.7 F microcatheter, avoiding the need for distal navigation of the intermediate catheter. Despite the lower profile, the SE maintains its typical rhomboid-shaped cell design and constant high mesh density (15–32 pores per mm2) across the aneurysm neck. As previously shown in a rabbit aneurysm model, mesh density is the single most important engineering determinant of the efficacy of flow-diverting devices.19 The smaller number of wires compared with the SS also theoretically decreases the risk for perforator infarctions, both when single or multiple implants are used.20 The combination of constant mesh density and optimized braid angle with a high number of wires (64 maximum in the SE vs 48 maximum in the Pipeline) demonstrated, in a recent in vitro study, that the SE has a higher flow-diverting effect than the Pipeline Flex.13 Furthermore, the length of the SE (up to 40 mm vs 35 mm for maximum length of the Pipeline Flex) facilitates use of a single implant for the treatment of most brain aneurysms.11
The SS has an over-the-wire deployment system that allows the use of an independent 0.014" microwire, whereas the SE does not. However, based on our experience, the XT-27 can easily be readvanced over the implant’s delivery wire, thus maintaining access for use of an appropriate regular microwire. Deployment of the SE does not particularly differ from that of a Pipeline. As many operators have considerable experience with the Pipeline Flex, we believe that the learning curve for deployment of this device will be shorter than that for the SS.
Chen et al reported a series of 39 successful transradial Pipeline placements commenting that the SS was not used owing to its larger and stiffer delivery system.21 In our limited experience, we showed that delivery through a 2.7 F microcatheter allows deployment through a 6 F guiding catheter if a transradial approach is preferred.
Our study has some limitations: (1) patients were not randomized, thus potentially there was a selection bias; (2) the population was heterogeneous because it includes wide-necked aneurysms of all sizes, thus limiting a comparison with the major trials, which targeted mostly more difficult large and giant aneurysms; (3) imaging follow-up was not available for all patients at 6 months.
Our first-in-human experience with the next generation of the Surpass FD, the SE, shows that the device is effective and has a good safety profile. The implant has excellent navigability and resistance to twisting, irrespective of device size or width. The smaller-profile delivery system and easier deployment, while maintaining a high flow diverting effect and precise positioning, would make it appropriate for aneurysms proximal and potentially distal to the circle of Willis, especially in cases of tortuous anatomies. Operators noticed difficulty in flushing larger implants and there is a theoretical risk of implant compaction due to smaller braid size if renavigation of the implant is needed. Multicenter prospective studies are needed to assess accurately the safety and efficacy of this new promising FD in the treatment of both proximal and more distal aneurysms.
References
Footnotes
Twitter @dralexandercoon
Contributors Contributorship Statement: Conception: EO, VMP, AKW, TK, HR; clinical data: EO, VMP, TK, HR, LDV, JMK, IR, KDB, HK; imaging review and follow up: EO, VMP, TK, JKM, HR, KDB, HK, AKW, ALC; writing: EO, VMP, AKW; review: EO, JMK, AKW, ALC, HR, LDV, HK, KDB, TK, VMP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests VMP is a consultant for Stryker, Balt, Medtronic, and Cerenovous and holds a grant from Philips Healthcare.TK is a consultant for Medtronic, Stryker, and Penumbra and is a stockholder in Marblehead Inc. AKW has research grant from Philips Medical; serves as a consultant for Stryker and Phenox; is a stockholder of InNeuroCo, EpiEP, Neural Analytics, Rist, Analytics 4 Life, and ThrombX; and is on the Speakers’ Bureau for SCENT trial (Surpass Intracranial Aneurysm Embolization System Pivotal Trial to Treat Large or Giant Wide Neck Aneurysms) presentations. ALC is consultant and proctor for Stryker, Medtronic, and Microvention and is on the Medical Advisory Board for InNeuroCo. HR is a consultant and proctor for, and receives educational support from, Stryker, Medtronic, Philips, Microvention, and Penumbra. All other Authors have no disclosures.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data from this study are included in the manuscript.