Article Text

Abstract
Background Interventional cardiology produced level 1 evidence recommending radial artery-first for coronary angiography given lower vascular complications. Neuroendovascular surgeons have not widely adopted the transradial approach. This prospective, single center, non-inferiority comparative effectiveness study aims to compare the transradial and transfemoral approaches for diagnostic cerebral angiography with respect to efficacy, safety and patient satisfaction.
Methods Consecutive patients presenting for diagnostic cerebral angiography were selected to undergo right radial or femoral access based on date of presentation. Primary outcome was ability to answer the predefined diagnostic goal of the cerebral angiogram using the initial access site and was assessed with a non-inferiority design. Secondary outcomes included technical success per vessel, complications, procedure times and patient satisfaction.
Results A total of 312 patients were enrolled, 158 and 154 for right radial and femoral access, respectively. The diagnostic goal of the angiogram was achieved in 152 of 154 (99%) patients who underwent attempted femoral access compared with 153 of 158 (97%) patients who underwent radial access, confirming non-inferiority of the transradial approach. Secondary outcomes showed equivalent technical success by vessel, no major complications, and similar frequency of minor complications between the two approaches. In-room time was similar between approaches, though post-procedure recovery room time was significantly shorter for transradial patients. Patient satisfaction results significantly favored the radial approach.
Conclusions In patients undergoing diagnostic cerebral angiography, transfemoral and transradial access achieve procedural goals with similar effectiveness and safety, though patients strongly prefer the radial approach. Findings support consideration of adopting a radial-first strategy for diagnostic cerebral angiography.
- angiography
- standards
- techniques
Statistics from Altmetric.com
Introduction
Interventional cardiology progressively adopted the transradial approach for coronary angiography over the past two decades, culminating in a radial-first strategy recommended by the American Heart Association due to significantly lower bleeding and vascular complications, as well as a significant mortality benefit compared with the transfemoral approach.1–13 With robust findings of improved patient safety and increased patient satisfaction14 15 demonstrated in the cardiology literature, neuroendovascular surgeons are increasingly employing transradial access for neuroendovascular procedures.16–26 However, prospective, randomized data remain lacking regarding the efficacy and safety of radial access for neuroendovascular diagnostic angiography as it directly compares to the traditional femoral approach.
In addition to the paucity of data regarding efficacy and safety, the field of neurointervention has been slow to adopt radial access for a variety of reasons. Overcoming the learning curve of an alternative surgical approach, perceived limitations of accessing a smaller artery, navigating the aortic arch from a different vector, and challenge in changing the culture among multidisciplinary staff within the angiography suite may all dissuade neurointerventionalists who have already mastered the transfemoral approach. We previously published on the early success, overcoming the learning curve, and limitations of the transradial approach for diagnostic cerebral angiography.20 21 With this established institutional baseline, a comparative effectiveness study of radial access and femoral access could be reliably conducted.
The aim of this study was to comprehensively evaluate the relative efficacy, safety and patient satisfaction of right radial access compared with femoral access for diagnostic cerebral angiography using a prospective, single-center, non-inferiority comparative effectiveness approach.
Methods
Study design
This study was a prospective, single-center, non-inferiority comparative effectiveness study in which consecutive patients referred for diagnostic cerebral angiography at a large academic quaternary care medical center were assigned to right radial access versus femoral access based on date of presentation. There is currently clinical equipoise about the femoral and radial approaches for endovascular procedures at our institution and the general endovascular procedural informed consent process encompasses both transfemoral and transradial access. Thus, our institutional review board approved this project as a quality improvement initiative and distinct research consent was waived.27 Goals of each procedure and intended supra-aortic arteries of interest were defined before the angiogram. With a non-inferiority design, α=0.05, and power=0.80, the study was powered to detect a 5% difference in ability to successfully answer the diagnostic goal of the angiogram with planned enrollment of a minimum of 135 patients in each arm.28
Patient selection
All consecutive adult inpatients and outpatients referred for diagnostic cerebral angiography were enrolled. Exclusion criteria included age <18 years, reasonable pre-angiogram likelihood of performing an endovascular intervention during the procedure, and the need for spinal angiography.
Approach selection and screening crossovers
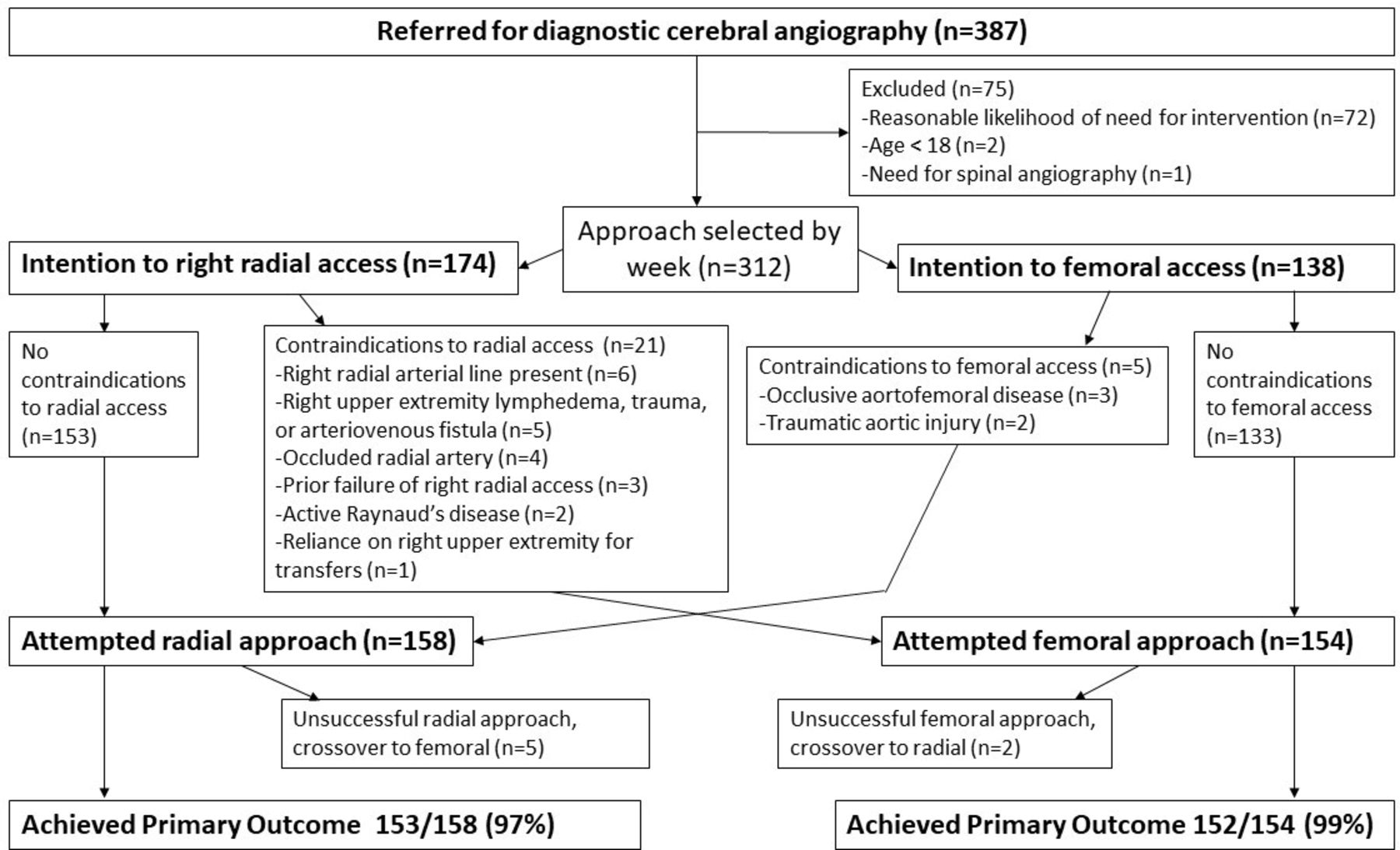
The approach selection algorithm is shown in figure 1 and was performed as follows: (1) patients were assigned to the intention-to-femoral approach or intention-to-radial approach on an alternating weekly basis; (2) patients assigned to the femoral approach were screened for pre-defined contraindications to femoral access; similarly, patients assigned to the radial approach were screened for pre-defined contraindications to radial access; (3) patients with noted contraindications to their assigned approach were crossed over to the alternative approach before the procedure. In this manner, patients were ultimately assigned to an “as-treated” approach that could practically be attempted.

{kind=link}
Patient selection and primary outcome.
Operator experience
Our institution is an academic cerebrovascular center that performs approximately 2000 neuroendovascular cases annually. Before involvement in this study, each operator had independently completed at least 30 (range 30–158) radial access angiograms and 100 femoral access angiograms—experience consistent with having overcome the basic transradial learning curve.21
Procedural protocol
Right transradial access was completed using a standardized procedure as previously described.20 21 No preprocedural upper extremity collateral blood supply testing was completed.5 29 Groins were not prepped. Although operators accessed the right radial artery in the majority of cases, the right ulnar artery was permitted to be accessed in patients with a diminutive radial artery and when the operator was unable to advance the 0.021 inch wire into the radial artery. All right arms were secured in fully supine position to allow access to both radial and ulnar arteries. Distal radial access within the anatomic snuffbox was not utilized for any patients. Ultrasound was used in every case. At the conclusion of radial access procedures, an inflatable transradial tourniquet was applied and air inflation titrated to attain patent hemostasis.30 Deflation of tourniquets was completed with standard protocol by recovery nurses starting 1 hour after placement with 3 mL air removed every 15 min until complete deflation. Neurovascular checks including assessment of radial artery pulse before discharge were completed by trained recovery nurses.
Femoral access was completed in a standard manner. Although operators accessed the right femoral artery in the majority of cases, the left femoral artery was permitted to be primarily accessed in patients with contraindications to right femoral artery access and whenever right femoral artery access failed. Ultrasound was used at the discretion of the operator. Mynx closure devices (CardinalHealth, Dublin, OH) were used in all cases followed by 5 min of manual pressure, and patients recovered with flat bedrest for 2 hours.
Primary outcome
The primary outcome was the ability to achieve the predefined diagnostic goal of cerebral angiography using the initial attempted access site. A modified procedural staging system was employed to subclassify different stages of access or need for more complex equipment into stages 1–3b, as previously described (online supplementary figure 1).20
Supplemental material
Secondary outcomes
Secondary outcomes were designed to compare technical success by vessel, safety, major and minor complications, procedure times, and patient satisfaction. We assessed total fluoroscopy time, radiation dose, and contrast utilization. Clinical complications were predefined and categorized as major general complications, major or minor transfemoral-specific complications, and major or minor transradial-specific complications. Procedure times prospectively collected included in-room, out-of-room, attempted access start (when access needle touches skin), successful access (after sheath successfully placed with appropriate back bleeding), procedure end (on placement of closure device), removal of transradial tourniquet, and discharge time for outpatients.
Patient satisfaction was assessed via a patient survey (online supplementary figure 2). Patient responses to the survey questions regarding access site pain immediately after sheath insertion and after sheath removal were recorded during the procedure, while answers to all other questions were recorded 90 min after the procedure, once the effects of sedating medications had subsided. Operators administered the survey during the procedure and trained nurses administered the remainder of the survey in the post-procedural recovery area. The timing of questions was standardized for all patients.
Supplemental material
Statistical analysis
The t-test was utilized to compare continuous variables and means between groups. Categorical variables were compared using Fisher’s exact test or χ2 analysis as appropriate. Given multiple t-test comparisons, a Bonferroni correction was applied and only p values <0.002 were considered significant. SPSS software version 23.0 (IBM, Armonk, New York, USA) was used for statistical tests.
Results
Patient cohorts
Between March 8 and June 27, 2019, 387 patients were enrolled and 75 excluded based on predefined exclusion criteria; then 174 were assigned to right radial access and 138 to femoral access on an alternating week basis (figure 1). Of the 72 patients excluded due to reasonable likelihood of needing an intervention, 33 (46%) had an intervention performed. After screening for predefined access-site specific contraindications, 21 (12%) patients assigned to the radial approach and five (4%) assigned to the femoral approach were crossed over, resulting in 158 and 154 patients in right radial and femoral access arms, respectively. Reasons for exclusion and screening crossover are shown in figure 1. Baseline characteristics between cohorts after screening crossover were all statistically similar (table 1).
Baseline characteristics
Primary outcome
Predefined goals of the diagnostic cerebral angiogram were achieved in 153 (97%) and 152 (99%) of right radial and femoral access cohorts, respectively (p=0.27). Based on pretrial power analysis, this confirms non-inferiority of right radial access to achieve the diagnostic goal of the cerebral angiogram.
In the radial arm, stage 1 failure occurred in two (1%) patients, stage 2 failure occurred in two (1%) patients, and stage 3 failure occurred in one (0.6%) patient. In all four patients who had stage 1 or stage 2 failure, radial artery diameters measured <1 mm. The two patients designated as stage 2 failure had successful radial artery cannulation with sheath, but experienced severe pain after sheath insertion which did not resolve with aspasmolytic cocktail, and thus the sheath was removed and procedural crossover to femoral access was pursued. We encountered radial artery anomalies in 26 (16%) of radial access patients including tortuosity in six (4%), stenosis/hypoplasia in 16 (10%), and radio-ulnar loop in four (3%), though none of these anomalies prevented successful completion of the angiogram with the exception of the two stage 2 patients previously described. Primary access of the ulnar artery was completed in three (2%) of the wrist access patients with subsequent successful completion of the angiogram. The patient designated as stage 3 failure presented with subarachnoid hemorrhage and was found to have a left posterior inferior cerebellar artery aneurysm that partially opacified with firm injection of the right vertebral artery. However, we were unable to directly catheterize the left vertebral artery despite adjunctive use of microcatheters/microwires to obtain adequate aneurysmal views; thus the patient was crossed over to femoral access. In all five right radial access patients who required crossover to femoral access, the cerebral angiogram was subsequently completed successfully through the femoral access site.
In the femoral access cohort, stage 1 failure occurred in one (0.6%) patient, stage 2 failure occurred in one patient (0.6%), and there were no stage 3 failures. The stage 1 failure occurred in a patient with a prior right femoral endarterectomy, so left femoral artery access was attempted primarily. The 21 G needle and 45 cm 0.021 inch wire were successfully advanced into the left femoral artery; however the 0.035 inch standard and extra stiff 0.035 inch dilators were unable to be advanced into the artery due to severe femoral artery atherosclerosis, so crossover to right radial access was necessary. The stage 2 failure occurred due to the presence of distal aortic occlusion. In both femoral access patients who required crossover to right radial access, the angiogram was subsequently completed successfully via the right radial approach.
Secondary outcomes
Technical success
Successful injection of predefined supra-aortic arteries of interest was achieved between 95% and 100% and there was no significant difference in technical success by vessel between the two approaches. We successfully accessed the left vertebral artery from the right wrist in 41/43 (95.3%) and the right vertebral artery from the groin in 70/72 (97.2%) (p=0.63). Although standard techniques were adequate in the majority of cases, adjunctive techniques, such as the use of long sheaths, intermediate catheters, microcatheters or microwires, were required in two (1.3%) patients in the femoral group and two (1.3%) patients in the radial group to complete the procedure (p=0.23).
Safety
The average transfemoral angiogram fluoroscopy time was 11.8 min, biplane radiation dosage 1510 mGy and contrast dosage 140 mL, compared with fluoroscopy time 14.8 min (p=0.001), biplane radiation dosage 1631 mGy (p=0.11) and contrast dosage 143 mL (p=0.67) in the radial group.
The average transfemoral angiogram procedural time was 29 min and the total in-room time was 1 hour 7 min, compared with a procedural time of 34 min (p=0.002) and a total in-room time of 1 hour 6 min (p=0.67) in the radial group.
Among the 121 outpatients in this study, the average transfemoral time from in-room to discharge was 3 hour 42 min, compared with 3 hour 25 min in the radial group (p=0.059). The average transfemoral recovery room time was 2 hour 52 min, compared with 2 hour 31 min in the radial group (p=0.009).
There were no major complications, and minor complications were similar between cohorts: four (2.5%) versus nine (5.8%) for radial and femoral access, respectively (p=0.14). Transfemoral-specific complications included severe access site local pain (n=3), closure device failure (n=4), and transient right leg paresthesias requiring extended recovery time (n=2). In comparison, transradial-specific complications included severe access site local pain (n=2), radial artery vasospasm (n=1), and closure device failure (n=1). There were no instances of radial artery occlusion.
Patient satisfaction
The patient satisfaction survey tool was administered to 112 (73%) of 154 patients in the femoral group and 128 (81%) of 158 patients in the radial group, with an overall response rate of 77%. The other 72 patients had a condition that prevented them from being able to respond to the survey questions, such as aphasia, altered mental status or endotracheal intubation.
Patient satisfaction significantly favored the radial approach concerning access site pain after sheath insertion, sheath removal, and before discharge, back pain before discharge, embarrassment, anxiety, and overall discomfort (table 2). Mean overall satisfaction showed a trend favoring radial access which nearly met statistical significance with a p value of 0.005.
Patient satisfaction
Patients in the radial access group reported a statistically higher preference for radial access if they had to undergo another angiogram (table 3). This preference showed a trend in the femoral access group which nearly met statistical significance with a p value of 0.008. Of patients who had a prior femoral access angiogram and then had radial access for the first time in this study (n=66), 56 (85%) preferred radial access for subsequent angiogram versus five (9%) who preferred femoral access, and five (8%) who had no preference.
Patient access site preferences for subsequent angiography
Discussion
Interventional cardiology produced level 1 evidence supporting the superiority of radial over femoral access for coronary angiography, given multiple, large, prospective, randomized trials showing lower vascular bleeding and renal complications, as well as a mortality and patient satisfaction benefit. However, the comparative efficacy and safety between transradial and transfemoral approaches for neuroendovascular procedures has not been previously established. We performed a prospective, non-inferiority comparative effectiveness study to directly compare these approaches. The primary outcome of this study was the ability to achieve the pre-defined goals of angiography; there was no difference in primary outcome between the transradial and transfemoral approach (97% vs 99%, p=0.27), confirming right radial access is non-inferior to femoral access for technical success. This result serves to address perceived efficacy limitations of the transradial approach including, but not limited to, difficulty accessing a smaller artery, advancing diagnostic catheters to the arch via a different corridor, and catheterizing supra-aortic vessels from a different vector. Our ability to catheterize the left vertebral artery from the right wrist was greater than 95% and statistically similar to our ability to access the right vertebral artery from the groin. As our field is in its infancy with regards to device and technology development specific to transradial neuroendovascular procedures, success and efficacy from the transradial approach have only potential to improve with time.
Moreover, secondary outcomes suggest patient safety is similar between approaches, though patient satisfaction is markedly higher with radial access. No major complications occurred and there was a statistically similar low rate of minor complications in the two groups. Though fluoroscopy time was higher in the radial access cohort, this was not clinically significant as total radiation dose was similar between groups. Importantly, though procedure time was 5 min longer for radial access (statistically significant), total in-room time was the same for radial and femoral access groups. For radial access, set up time was saved without the need to prep groins and immediately post-procedure without the need to hold femoral pressure after closure device deployment. Importantly, recovery room time was lower and discharge home time faster in the radial access group. When taken together, radial access showed a trend toward lower total time from entry into the angiography suite to discharge home which nearly reached statistical significance. We employed a relatively conservative transradial tourniquet deflation protocol by starting gradual deflation at 1 hour after placement of tourniquet. Other centers initiate deflation after 30 min. With a less conservative deflation protocol, total recovery time could be significantly lessened further in radial access patients.
With regards to patient satisfaction, radial access patients reported significantly less access site pain, back pain, embarrassment, anxiety and overall discomfort with significantly greater overall satisfaction. Patients strongly preferred the radial approach for future angiography and 85% of patients who previously underwent both transradial and transfemoral approaches would request transradial access for their next angiogram. In a healthcare climate demanding increasingly efficient utilization of resources and reimbursement tied to reported patient satisfaction, practice changes that improve patient satisfaction scores are vital.
Important limitations of this study include its single-center analysis and modest size as compared with cardiology trials. Complication rates of diagnostic cerebral angiograms are low; this study was not powered to detect a difference in complication rates between the two access approaches. Though no patients experienced symptomatic radial artery occlusion, we did not perform ultrasound examination post-procedure, only radial pulse checks by trained recovery nurses. Thus, we cannot reliably report the incidence of asymptomatic radial artery occlusion in this study. Anatomic contraindications to each approach exist; 8.3% (26 of 312) of the patients in this study were not candidates for their selected approach because of pre-defined contraindications. The rate of pre-procedure crossovers was higher for the group assigned to the transradial approach (12% vs 4%, p=0.007), but not for intraprocedural crossovers (3.2% vs 1.3%, p=0.27). This is likely reflective of strict screening criteria for the transradial approach utilized in this study; it is possible that many of these patients excluded from the transradial approach could have safely undergone radial arteriography. The results of this study are only valid for neurointerventionalists who are trained in both transradial and transfemoral cerebral angiography. Our center has considerable experience with both approaches; as such, the results of this study may not be valid for centers without significant prior transfemoral and transradial experience. The patient satisfaction survey utilized in this study was not an externally validated instrument.
Conclusion
This prospective, comparative effectiveness study directly comparing right transradial and transfemoral access for diagnostic cerebral angiography confirms equivalent success and patient safety, with a significant patient satisfaction benefit favoring right radial access. Findings of this report prompted our institution to adopt a radial-first approach for diagnostic cerebral angiography and can serve as a basis for future trials focused on comparing radial and femoral access for neuroendovascular interventions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrJeremyStoneMD, @shashvatdesaiMD, @ashupjadhav
Contributors Study design: JS, BMZ, BJ. Drafting the article: JS. Acquisition of data/data analysis: JS, BMZ, DAT, MB/ JS, SMD. Reviewed and revised article before submission: all authors. Study supervision: BJ.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BJ: Consultant: Medtronic, Stryker. MB: Investor: Penumbra, Inc. BAG: Consultant: Microvention. TGJ: Consultant: Stryker Neurovascular (PI DAWN-unpaid), Ownership Interest: Anaconda, Advisory Board/Investor; FreeOx Biotech, Advisory Board/Investor; Route92, Advisory Board/Investor; Blockade Medical, Consultant; Honoraria: Cerenovus.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement De-identified patient data are available from the authors upon reasonable request.