Article Text

Abstract
Introduction Preliminary studies suggest that flow-diverting stents may be suitable for the treatment of aneurysms of the posterior circulation. The safety and efficacy of using flow-diverting stents for vertebral artery (VA) aneurysms is not well defined.
Objective To examine the fate of covering the posterior inferior cerebellar artery (PICA) in patients undergoing placement of a flow-diverting stent for VA aneurysm.
Methods Consecutive patients who underwent placement of a Pipeline Embolization Device (PED) for treatment of an aneurysm of the V4 segment of the VA between April 2012 and June 2015 at our institution were retrospectively evaluated. Angiograms were reviewed to determine the patency of the PICA when the vessel origin was covered by the PED.
Results 11 patients with VA aneurysms who underwent treatment with the PED were identified. In each case the device covered the origin of the PICA. Follow-up angiography in eight patients demonstrated thrombosis of the aneurysm with patency of the PICA.
Conclusions Flow-diverting stents can be used for the treatment of VA aneurysms. When appropriately sized to the vessel wall and positioned in the VA, the device may cover the origin of the PICA without impairing flow through the branching artery.
Statistics from Altmetric.com
Introduction
The Pipeline embolization device (PED; Covidien–Ev3, Irvine, California) is a flow-diverting stent that may be suitable for the treatment of vertebral artery (VA) aneurysms arising adjacent to the ostia of the posterior inferior cerebellar artery (PICA), anterior spinal artery, or basilar perforating arteries. The presence of interstices between the stent struts allows blood flow to branch arteries and perforating vessels while disrupting flow within the aneurysm, eliminating shear stress on the aneurysm wall, and causing intrasac thrombosis.1 Vessel remodeling occurs as neointimal growth proceeds across the aneurysm neck and the intrasac thrombus is resorbed.
The use of the PED for the treatment of aneurysms of the anterior circulation has been well described.2 In contrast, the safety and efficacy of the PED for posterior circulation aneurysms has not been established definitively. The literature on this subject is growing, but consists mainly of small series of patients.3–9 Because of the large number of perforating vessels in the posterior circulation that supply vital brainstem structures, endovascular surgeons have been cautious about using flow-diverting stents in this region. There have been very few reports of cases in which the ostium of the PICA is covered by a PED placed in the VA. We report the use of the PED in patients with aneurysms involving the intradural segment (V4) of the VA.
Methods
We retrospectively evaluated the angiograms of consecutive patients who underwent placement of a PED for treatment of an aneurysm of the V4 segment of the VA between April 2012 and June 2015 at our institution. Angiograms obtained after PED placement were reviewed to determine the patency of covered branch vessels and aneurysm occlusion. All authors reviewed the angiograms, and a consensus was reached regarding patency of covered branch vessels and aneurysm occlusion.
All patients were treated with the PED using a standard technique under monitored sedation as the sole endovascular intervention. Patients were premedicated with dual antiplatelet agents (clopidogrel 75 mg/day and aspirin 325 mg/day) for 7 days prior to the procedure. Platelet function was assessed on the day of the procedure by measuring the P2Y12 value for a target <194 P2Y12 reaction units (PRUs). Patients were also anticoagulated with an intravenous heparin bolus (70 U/kg) with titration to maintain an activated clotting time (ACT) >250 s or two times the patient's baseline.
The PED was positioned to cover the neck of the aneurysm and the diseased segment of the VA. The distal end of the PED was positioned proximal to the vertebrobasilar junction whenever possible to prevent jailing the contralateral VA. The insertion of multiple overlapping stents was also avoided so blood flow through covered branch vessels and perforating arteries could be maintained. The diameter of the PED was selected to closely appose the vessel wall at the proximal VA, thereby preventing endoleak around the device. In all cases, the PED was oversized 0.5 mm greater than the diameter of the vessel wall to elongate the struts, thereby decreasing the risk of covered vessel occlusion. A final angiogram was obtained after deployment to assess stent placement and vessel patency.
Heparin use was discontinued at the end of the procedure but its effects were not reversed. Patients were continued on dual antiplatelet therapy with clopidogrel (75 mg/day) and aspirin (325 mg/day) after surgery. Follow-up CT angiography (CTA), MR angiography (MRA), or digital subtraction angiography (DSA) were performed at 6 months. If the aneurysm was occluded and the PED was patent, clopidogrel was discontinued but treatment with aspirin (325 mg/day) is continued for life. An additional follow-up angiogram was obtained at 1 year.
In urgent cases in which antiplatelet premedication was not possible, a loading dose of abciximab was administered (0.25 mg/kg) immediately before PED deployment and dual therapy was continued after the procedure. For patients who had a PRU >194 on the day of the procedure despite premedication with aspirin and clopidogrel, a half loading dose of abciximab (0.125 mg/kg) was administered immediately after PED deployment, and patients were continued on aspirin and prasugrel (10 mg/day) thereafter.
Results
Thirteen patients underwent PED placement for an unruptured aneurysm of the V4 segment of the VA during the study period, 11 of whom had the ostia of the PICA covered by the PED. These 11 patients comprised the study cohort (table 1). The mean age of the patients was 52 years (range 39–59 years); six patients were female (55%). Two of the 11 patients had ruptured dissecting aneurysms with subarachnoid hemorrhage. In six patients the aneurysm was diagnosed on imaging obtained for evaluation of headache, neck pain, or facial pain. In one patient the aneurysm was diagnosed on follow-up for a left internal carotid artery dissection. One patient presented with headaches and neck pain after blunt head trauma. One patient presented with ataxia, dysphagia, and vertigo from a PICA stroke.
Patients with VA aneurysm who underwent PED placement with stent covering branch vessel
In 10 patients the aneurysm was located on the right VA, and one patient had a saccular aneurysm arising from the PICA–VA junction (figure 1). The aneurysm was located distal to the PICA ostia in three patients (figure 2), proximal to the PICA ostia in four, and involved the PICA ostia in four. Two patients had saccular aneurysms and nine had fusiform dissecting aneurysms. Both ruptured aneurysms were of the dissecting type. One patient had two fusiform dilations from an enlarging dissecting aneurysm (figure 3). In each case, prior to treatment there was no evidence of flow restriction through either the VA or the PICA.

Patient 2. (A) Pre-procedure digital subtraction angiography showing saccular aneurysm arising from the vertebral artery–posterior inferior cerebellar artery (VA–PICA) junction. (B) CT angiogram (CTA) obtained 6 months after Pipeline embolization device (PED) deployment showing aneurysm occlusion with patency of PICA.

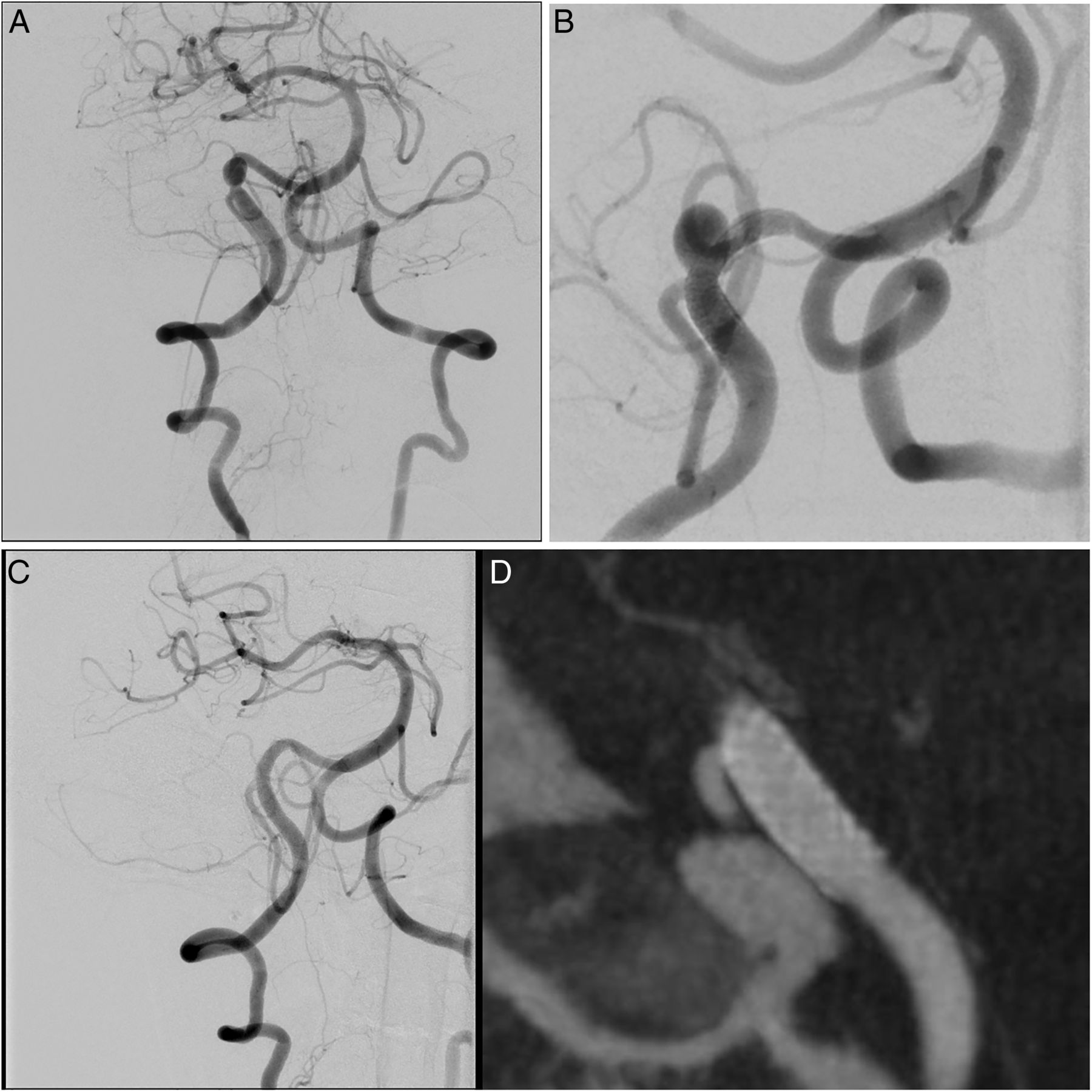
Patient 1. (A) Digital subtraction angiography (DSA) depicting saccular aneurysm of the right vertebral artery just distal to the origin of the posterior inferior cerebellar artery (PICA). (B) Magnified view showing placement of the Pipeline embolization device (PED) across the neck of the aneurysm and the origin of the PICA. (C) DSA at 1 year showing aneurysm occlusion and vessel remodeling. (D) Dyna CT at 1 year showing patency of the covered PICA.

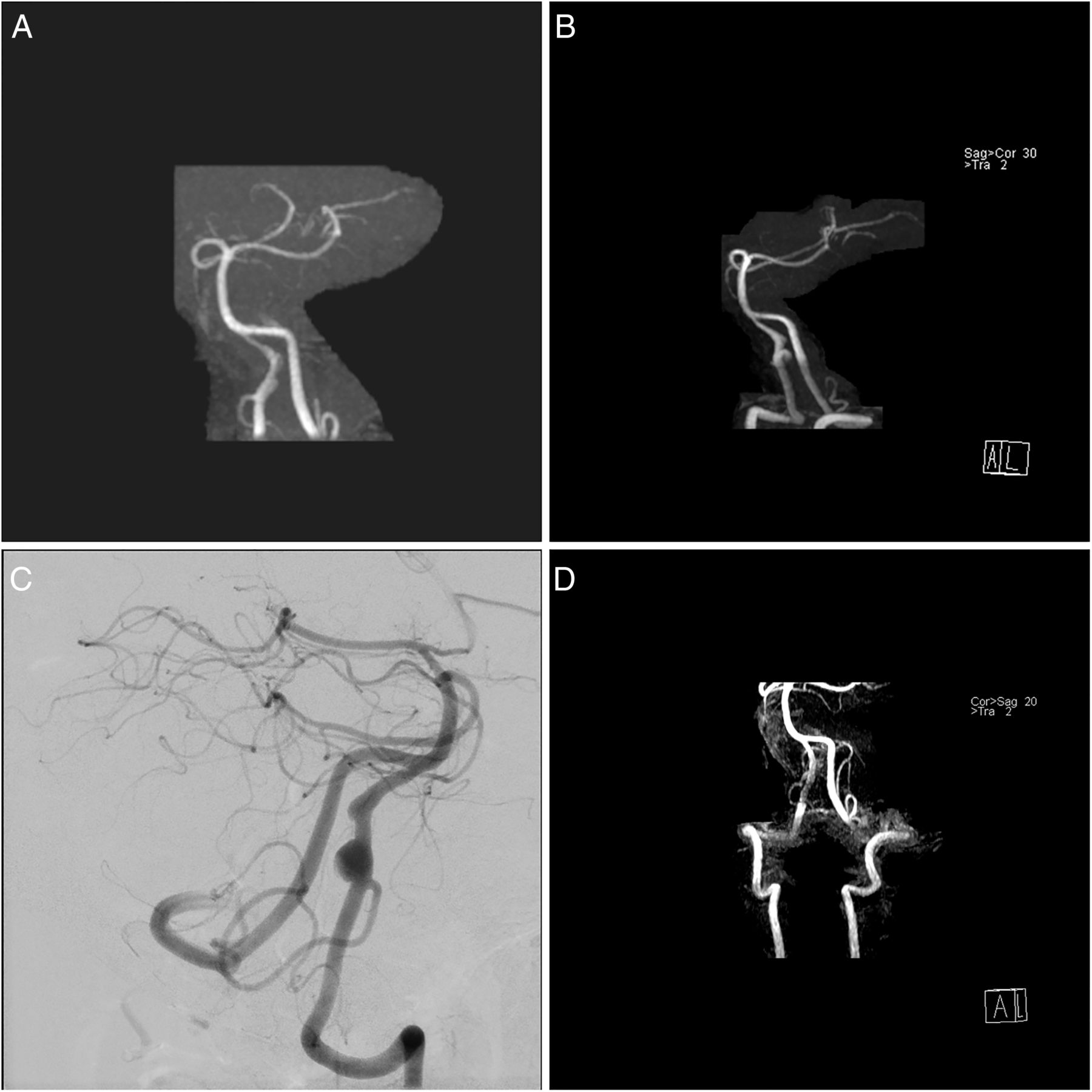
Patient 6. (A) MR angiogram (MRA) showing two fusiform dilations of a dissecting vertebral artery (VA) aneurysm. (B) Interval MRA 5 months later showing enlargement of the dissecting VA aneurysm. (C) Digital subtraction angiography showing aneurysms located just distal to the posterior inferior cerebellar artery (PICA) origin. (D) MRA obtained 6 months after Pipeline embolization device (PED) deployment demonstrating that the covered PICA is patent. There is artifact of the stented segment of the VA from the PED.
Elective cases
Nine patients underwent elective treatment of an unruptured VA aneurysm using the PED. All nine patients who underwent pretreatment with dual antiplatelet therapy responded appropriately (<194 PRU) on the day of the procedure. In each of these nine elective cases the distal end of the PED was positioned proximal to the vertebrobasilar junction and the covered PICA branch remained patent on the angiographic run immediately after PED deployment. Angiographic follow-up was available on eight patients (range 3 weeks to 1 year). In these eight patients, no covered branch vessel occlusions were identified and there was no evidence of flow restriction through the VA or the covered PICA. All eight patients demonstrated evidence of vascular reconstruction of the affected V4 segments with aneurysm occlusion. Aneurysm occlusion was visualized as early as 3 weeks after PED placement. There was no evidence of in-stent stenosis or endoleak on any of the follow-up angiograms. No patient developed new neurological symptoms after PED placement.
Emergency cases
Two patients presented with subarachnoid hemorrhage from a ruptured VA aneurysm, both of which were treated with the PED. Both received intraprocedural abciximab followed by dual antiplatelet therapy post-procedure. In one patient the PED remained proximal to the vertebrobasilar junction (Patient 7) whereas, in the other, the distal end of the PED was positioned in the basilar artery (Patient 8).
Patient 8 developed immediate in-stent stenosis and occlusion of the covered PICA after PED employment; after abciximab administration the in-stent stenosis resolved. The covered PICA recanalized on follow-up imaging 6 months later (figure 4), and although the patient suffered a PICA distribution infarction ipsilateral to the treated aneurysm, she recovered to her neurological baseline. In this patient the distal end of the PED was positioned in the basilar artery; therefore, the contralateral VA ostium was covered. On follow-up, occlusion of the contralateral V4 segment was seen extending from the contralateral PICA ostium to the basilar artery. The contralateral PICA remained patent.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
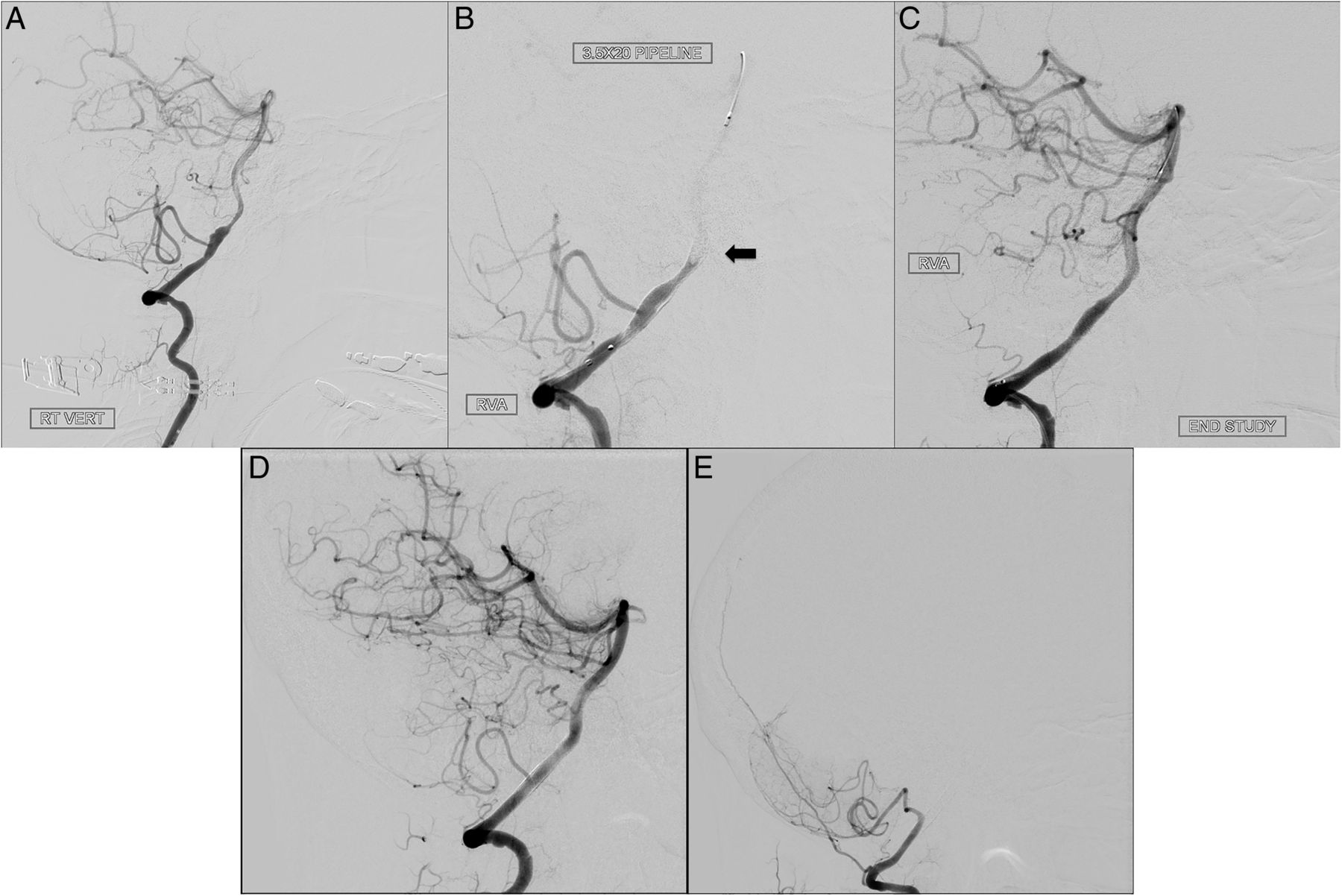
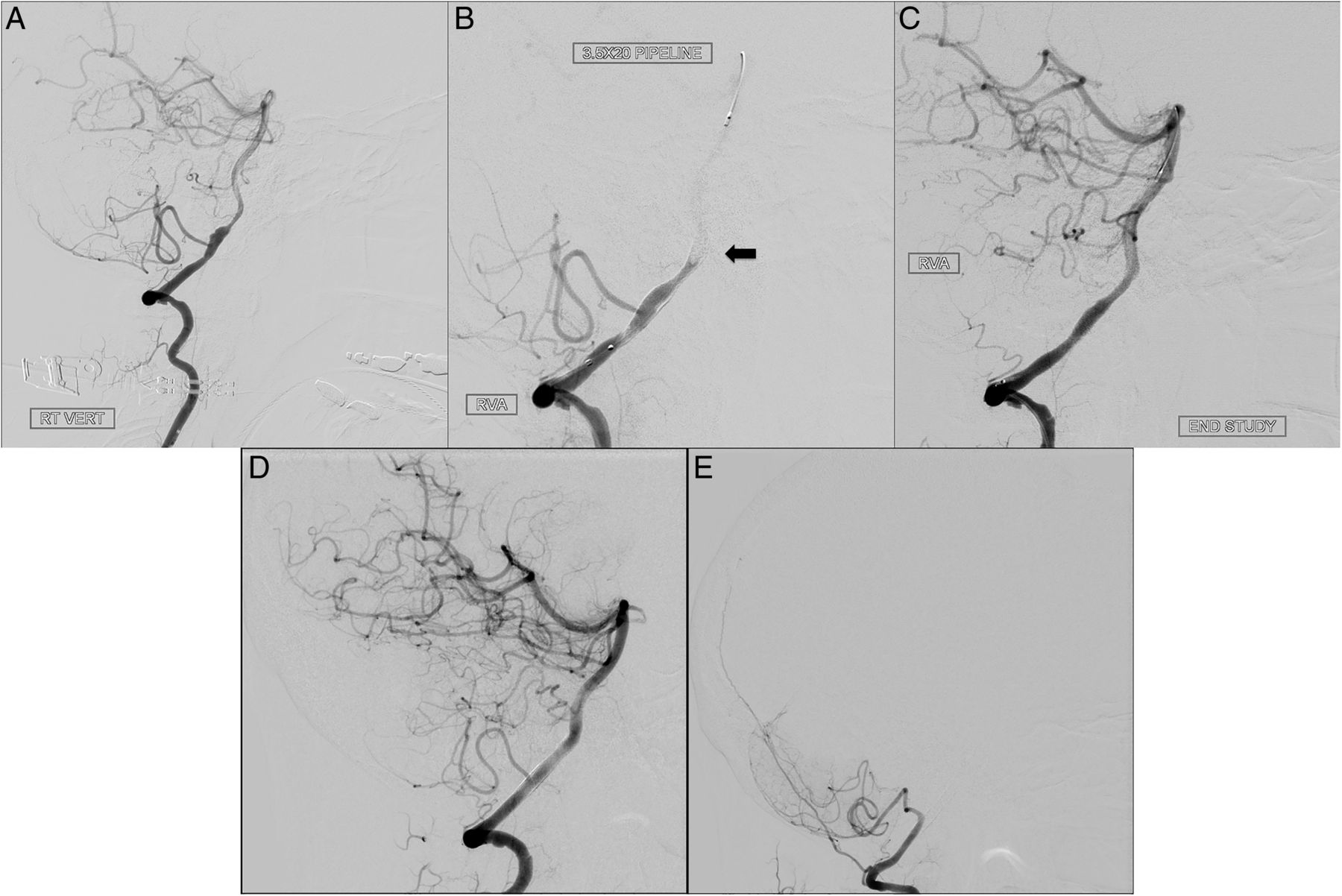
Patient 8. (A) Pre-procedure digital subtraction angiography (DSA) showing dissecting fusiform right vertebral artery (VA) aneurysm involving the posterior inferior cerebellar artery (PICA) ostia. (B) Intra-procedure run depicting acute basilar artery occlusion during Pipeline embolization device (PED) deployment. The distal end of the PED is located in the mid-basilar artery (arrow), covering the left VA. (C) Intra-procedure run shows recanalization of the basilar artery but occlusion of the covered PICA. DSA obtained 6 months after PED deployment shows (D) reconstruction of the right VA, occlusion of the dissecting aneurysm, and recanalization of the covered PICA and (E) occlusion of the covered left VA distal to the left PICA.
Illustrative case
Patient 6: A 40-year-old man underwent an MRA for evaluation for headaches and neck pain after a skiing accident and was found to have a 5 mm fusiform aneurysm located on the V4 segment of the VA, just distal to the PICA origin. He was started on daily aspirin monotherapy (325 mg). Five months later, a follow-up MRI demonstrated enlargement of the aneurysm to a diameter of 10 mm with an additional 5 mm aneurysmal dilation located distal to it. An enlarging dissecting aneurysm was diagnosed and treatment with a PED was proposed. Dual antiplatelet therapy with aspirin and clopidogrel was initiated and the intervention was planned for 1 week later.
The P2Y12 result on the day of the procedure was 130 PRU. A loading dose of intravenous heparin (70 U/kg) was administered, and anticoagulation was titrated to maintain an ACT >250 s. The right VA was selected and the PED was deployed in the standard method described above. The distal end was positioned in the segment of the VA that was proximal to the vertebrobasilar junction. The PED covered both fusiform dilations of the dissecting aneurysm. Because of the proximity of the aneurysm to the PICA, covering the ostia of the PICA was unavoidable. An angiogram obtained after deployment demonstrated normal flow in the right VA, PICA, basilar artery, and posterior cerebral arteries. There was no evidence of complication or distal emboli.
The patient continued taking dual antiplatelet therapy (clopidogrel 75 mg/day and aspirin 325 mg) after the procedure. At 6 months, an MRA demonstrated obliteration of the dissecting aneurysm with remodeling of the diseased V4 segment. The PED was patent without evidence of in-stent stenosis. Clopidogrel was discontinued but the patient has continued taking lifelong aspirin monotherapy.
Discussion
VA aneurysms adjacent to the PICA origin are challenging to treat. Both endovascular and microsurgical treatments can put the PICA, anterior spinal artery, and basilar perforators at risk. Currently, the treatment of posterior circulation aneurysms has shifted away from microsurgical clipping to endovascular techniques. Parent vessel occlusion, trapping, coiling, stent-assisted coiling, or stent monotherapy are currently used to treat these aneurysms. Parent artery occlusion is a reliable technique for obliteration of the aneurysm, but it may not be feasible for cases with dominant artery or major branch (PICA or anterior spinal artery) involvement without collateral flow. In these cases, flow-diverting stents such as the PED may be the preferred treatment modality.
One of the advantages of the PED is the potential to maintain patency of branching vessels and perforators arising from the parent artery.10–13 The presence of interstices between stent strands facilitates flow to branching vessels while disrupting flow in the aneurysm and causing intrasac thrombosis. The drawback is that patients receiving PEDs must undergo dual antiplatelet therapy, usually with aspirin and clopidogrel, which exposes them to an increased risk of hemorrhagic complications. At our institution, vascular imaging via CTA, MRA, or DSA is obtained after 6 months. If the aneurysm is occluded without evidence of endoleak or in-stent stenosis, then clopidogrel is discontinued to reduce this risk, although the patient is treated with aspirin monotherapy for life.
Flow-diverting stents, such as the PED, are designed to be porous enough to preserve the patency of branch vessels that are covered by the device while simultaneously altering flow away from the aneurysm. Thromboembolic complications after PED placement more frequently occur in distal branches and parent arteries, particularly in the posterior circulation;14 ,15 however, thrombosis of perforating branches remains a risk. A recent meta-analysis reported a perforator infarction rate of 3%, with a higher rate among patients with posterior circulation aneurysms than those with anterior circulation aneurysms.15 One explanation for this trend is the lack of collateral blood flow in the posterior fossa. The risk of thrombosis may increase if multiple overlapped PEDs are inserted, although animal studies of this scenario have demonstrated excellent patency of small branch arteries.10 Other potential causes of perforator thrombosis include clopidogrel resistance, poor apposition of the PED to the aneurysm wall, neointimal overgrowth over the branch vessel, or endothelial injury triggering platelet aggregation.
It is generally believed that covered branch arteries will remain patent provided that flow is maintained through the PED.11 ,16 One theory is that demand phenomena continue to draw blood into the covered branch.17 None of the patients in our series developed flow restriction of a covered PICA; however, other reports have shown mixed results regarding the fate of covered branch vessels.4 ,18–20 Yeung et al4 reported one patient with a dissecting aneurysm of the VA treated with PED that required coverage of the PICA because of its close proximity to the aneurysm. A follow-up angiogram at 18 months demonstrated patency of the PICA with obliteration of the aneurysm. Lall et al21 described one patient with a giant vertebrobasilar aneurysm who experienced dysarthria and lower cranial neuropathies immediately after PED placement from PICA occlusion. After treatment with intra-arterial abciximab, a follow-up angiogram demonstrated revascularization of the PICA and the patient experienced a resolution of the neurological symptoms. Chalouhi et al5 described patency of a covered PICA 6 months after three overlapping PEDs were deployed for a left VA aneurysm. Other studies have reported the fate of covered branches of the anterior circulation or basilar artery.4 ,16 ,18–24 It is important to note that many perforating vessels in the vertebrobasilar system cannot be seen on angiography.
We report that the PED was positioned proximal to the vertebrobasilar junction in 10 of 11 patients, allowing flow from the contralateral VA to proceed unimpeded. In Patient 8 the distal end of the PED was positioned in the basilar artery, which obstructed inflow from the contralateral VA and resulted in occlusion of the contralateral V4 segment distal to the PICA.
The ostium of the PICA was covered in all of our cases. One patient experienced a PICA occlusion during PED placement and developed an associated region of diffusion restriction on postoperative MRI. Her 6-month follow-up angiogram demonstrated recanalization of the covered PICA. Of the 10 remaining cases, none developed new neurological symptoms associated with PICA occlusion, such as lateral medullary syndrome or Wallenberg syndrome (ie, ataxia, dysphagia, hoarseness, nausea, vertigo, or nystagmus). It is possible that collateralization may develop over time between branches of the PICA and anterior inferior cerebellar artery or the posterior meningeal artery, which may protect against lateral medullary infarction; however, we did not identify such anastomoses or new collateral circulation in any of our patients during our short follow-up period.
Each of our patients required only one PED stent for adequate aneurysm neck coverage. In contrast, Munich et al6 reported a series of 12 patients undergoing PED placement for fusiform vertebrobasilar aneurysms, of whom 11 required multiple stents. These authors reported new periprocedural neurological complications in three patients, large posterior circulation infarcts in two patients, and three patients with silent microembolic infarcts on postoperative MRI. Furthermore, one patient had residual aneurysm filling and endoleak requiring additional treatment, one developed stenosis proximal to the PED requiring balloon angioplasty, and one developed in-stent stenosis. The use of multiple stents may increase the risk of PED-associated complications, particularly if there is too much overlap and metal surface area coverage. Studies with larger sample sizes are needed to more accurately determine the factors associated with thromboembolic complications from PED use in the posterior circulation.
One of the limitations of this study is the short follow-up time. In-stent thrombosis from intimal hyperplasia and occlusion of distal branches and perforating vessels is a potential complication of the PED. Cases of in-stent thrombosis occurring 1 year after treatment or later have been reported.3 ,25 One patient with a VA aneurysm treated with multiple telescoping PEDs experienced device thrombosis 1 year later.25 Dual antiplatelet therapy with clopidogrel and aspirin for 6 months followed by lifelong daily aspirin has been the standard regimen to prevent this complication. Long-term studies are needed to determine the efficacy of the PED as well as the optimal post-treatment antiplatelet regimen. While all of our patients had follow-up vascular imaging, follow-up MRIs were not performed on all patients so we were not able to determine whether there were any clinically silent thromboembolic complications. No patient in our series developed new neurological deficits or symptoms after PED placement.
In 10 of 11 of our cases, the distal end of the PED was positioned proximal to the vertebrobasilar junction. This location is chosen to avoid covering the contralateral VA. In contrast to a covered PICA through which flow is directed outward from the interstices of the PED to the branch artery, flow of the contralateral VA is directed toward the PED. Thus, a covered VA increases the risk of developing an endoleak if the stent is not directly apposed to the vessel wall and blood can pass around the device. Moreover, the PED may obstruct flow from the covered contralateral VA, increasing the risk of thrombosis. The anterior and posterior spinal arteries also arise from the distal V4 segment, proximal to the vertebrobasilar junction. The fate of covering these branch vessels has not been evaluated.
Our findings demonstrate the successful use of PED for the treatment of the various types of VA aneurysms neurointerventional surgeons will encounter, including ruptured, unruptured, saccular, and dissecting. As the use of PED increases, larger studies are needed to determine long-term outcomes such as rates of aneurysm occlusion, thromboembolic complications from device insertion, and the sequelae of covered branch vessels and perforators. Our results provide a rationale to base further investigation on PED use in the posterior circulation.
Conclusions
We report preliminary experience with the successful treatment of 11 patients with aneurysms of the VA using the PED. In each case the PED covered the ostium of the PICA. One patient developed an intraprocedural PICA occlusion on the ipsilateral side of the treated aneurysm but had PICA recanalization at 6 months follow-up. In this patient the PED covered the contralateral VA, resulting in an asymptomatic V4 segment occlusion. Follow-up angiography was available in eight patients, and each demonstrated thrombosis of the aneurysm with patency of the PICA.
Acknowledgments
The authors thank Kristin Kraus for her help in preparing this manuscript.
References
Footnotes
Contributors MDM: Authored manuscript, data collection. CK, VW: Data collection. PT: Study design, study supervision, data collection, critically reviewed manuscript.
Competing interests PT is a consultant for Covidien and proctors physicians in the use of the PED.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the University of Utah IRB (#82408).
Provenance and peer review Not commissioned; externally peer reviewed.