Article Text

Abstract
Background and purpose While recent literature has described the prevalence of transverse sinus stenosis in patients with idiopathic intracranial hypertension, tinnitus, and refractory headaches, it is unclear what the prevalence is in the general population. This study evaluates the prevalence of venous sinus stenosis and hypoplasia in the general patient population.
Materials and methods 355 of 600 consecutive patients who underwent CT angiography of the head met the inclusion criteria. The diameters of the dural venous sinuses were recorded. Each study was evaluated by a neuroradiologist for the presence of stenoses. Univariate and multivariate statistical analyses were performed by a statistician.
Results The prevalence of unilateral transverse sinus stenosis or hypoplasia in a sample of patients representing the general population was 33%, the prevalence of bilateral transverse sinus stenosis was 5%, and the prevalence of unilateral stenosis with contralateral hypoplasia was 1%. A multivariate analysis identified arachnoid granulations as a predictor of stenosis (p<0.001). Gender trended toward significance (p=0.094). Race was not a significant predictor of stenosis (p=0.745).
Conclusions The prevalence of bilateral transverse sinus stenosis in the general population is not trivial. These data may be used as a reference for understanding the mechanistic role of stenoses in idiopathic intracranial hypertension, tinnitus, and refractory headaches.
- Blood Flow
- CT Angiography
- Intracranial Pressure
- Stenosis
- Vein
Statistics from Altmetric.com
Introduction
In recent years, the dural venous sinuses and jugular veins have attracted the interest of clinical researchers for their potential role in idiopathic intracranial hypertension (IIH) or pseudotumor cerebri, medically refractory headaches, tinnitus, and venous sinus thrombosis.1–7 Despite identifying a correlation between the anatomic variations in the venous sinuses and specific disease processes, we still know little about the underlying pathophysiology of how variations in cerebral venous outflow can manifest patients’ symptoms.
The most common theories to describe the mechanism underlying these disorders include either overproduction of cerebrospinal fluid (CSF) or inadequate resorption of CSF. However, a more recent extension of these theories suggests that CSF production or resorption dysfunction may be an effect of elevated intracranial venous pressures. Venous hypertension has been associated with transverse sinus stenosis, but it is not clear whether the hypertension is a cause, an effect, or both. Fibrous septae or arachnoid granulations can result in direct intrinsic obstruction of blood flow through the sinus,8 ,9 while elevated intracranial pressures may lead to extrinsic obstruction of blood flow.10 ,11
An initial step toward understanding the pathophysiology is to understand what is ‘normal’ in the general population. While dural venous sinus anatomic variability has been well documented, there are very few published data describing venous sinus stenosis in the general population. The purpose of this study is to evaluate and describe the prevalence of venous sinus stenosis, hypoplasia, and basic drainage patterns among a consecutive group of patients within the general patient population.
Materials and methods
Patient selection
Six hundred consecutive patients who underwent CT angiography (CTA) of the head at our institution between March and October 2013 were included in the study. Any study with CT venography (CTV) was immediately excluded. Exclusion criteria are listed in table 1 along with the number of patients meeting each criterion. In total, 355 patients were included in the final analysis.
Exclusion criteria and the number of patients meeting each criterion
Imaging protocol
All studies were performed on either 16-slice (Lightspeed, Lightspeed Pro) or 64-slice (Lightspeed VCT, HD 750 Discovery) GE CT scanners (GE Healthcare, Waukesha, Wisconsin, USA). CTA was performed at 0.625 mm with a pitch of 1.375:1, a table speed of 27.5, 120 kV, auto amperage ranging from 200 to 350 mA, and a field of view of 25 cm. Angiographic images were acquired from either the aortic arch or the skull base through the vertex of the head (depending on whether imaging of the neck was requested) after the administration of 100 mL of contrast, although dosages varied based on patient size and glomerular filtration rate.
Image interpretation
All studies were evaluated by one of three fellowship trained neuroradiologists with a 20% overlap in assignment to verify inter-reader agreement as described below.
The CTA source data were loaded onto a Carestream Vue PACS system V.11.3 (Carestream Health, Rochester, New York, USA). The CTA studies were reconstructed using the vessel analysis tool (figure 1). The density of the superior sagittal sinus (SSS) and each transverse sinus was measured in Hounsfield units. Each sinus was divided into thirds (proximal, mid, and distal according to the direction of flow through the sinus). Representative measurements were obtained in each third of the sinus (figure 1B), including the minimum, maximum, and mean diameter of the vessel, and the cross-sectional area. Readers interpreted the images to identify stenosis, arachnoid granulations, fistulas, sinus thrombosis, and common venous variants, including alternative outflow anatomy. In the case of a venous sinus stenosis, the readers recorded whether the stenosis was smooth or abrupt, the narrowest width, the length of the stenosis, and the location of the stenosis within the sinus.
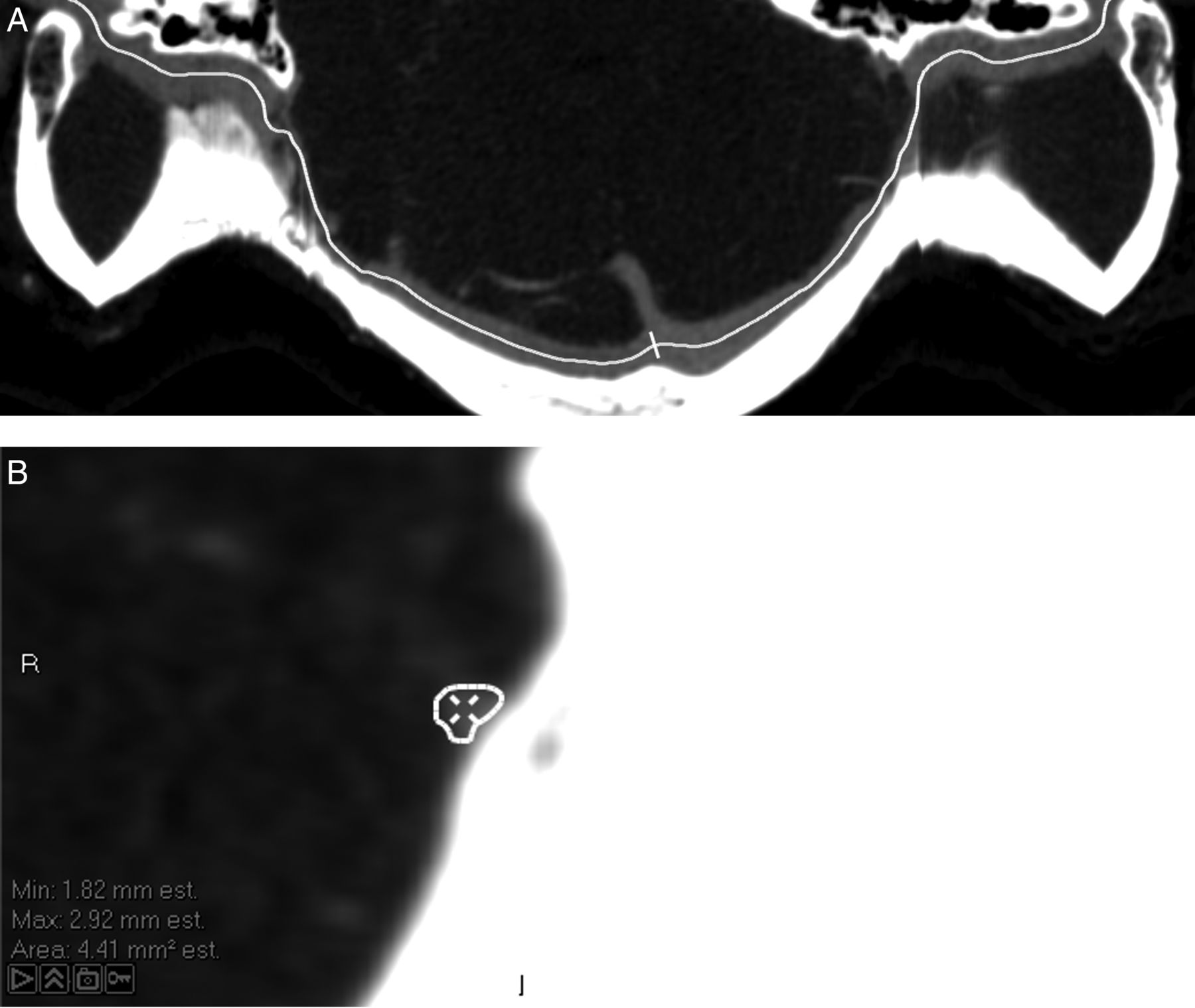
(A) Output of the Carestream Vue vessel analysis tool demonstrating a smooth tapered stenosis of the distal left transverse venous sinus and an abrupt stenosis of the distal left transverse sinus due to an arachnoid granulation. (B) Cross-sectional view of the stenotic left transverse sinus demonstrating edge detection of the vessel margins and automatic measurement of vessel diameter and cross-section area.
Defining transverse sinus dominance
Historically, authors have subjectively determined which transverse venous sinus is dominant. A post hoc review of the images included in this study reveal that a 20% difference in the size of the transverse sinuses was the threshold at which all readers could agree that the larger sinus could be called ‘dominant’.
Defining a stenosis and hypoplasia
Using models developed by Marmarou et al12 and Stevens et al,13 a stenosis was defined as a 40% reduction in caliber of the vessel. Similarly, a hypoplastic sinus was defined as a sinus that is 40% smaller in average caliber than the contralateral sinus.
Inter-reader agreement
To determine the level of agreement between readers, 20% of all studies were reviewed by a second reader. Inter-reader agreement was estimated using the Fleiss κ statistic based on each reader's interpretation of the presence or absence of a transverse venous sinus stenosis.
Statistical analysis
Data are presented as mean and range for continuous variables and as frequency for categorical variables. Statistical analyses of categorical variables were carried out using χ2 and Fisher exact tests as appropriate. Statistics of means were carried out using the unpaired Student t test, both with and without equal variance (Levene test) as necessary, and Wilcoxon rank sum tests when variables were not normally distributed. Analysis of variance followed by Bonferroni post hoc testing was used to assess means between three or more groups. Clinical covariates predicting bilateral transverse sinus thrombosis with a univariate p<0.15 were included in the multivariable logistic regression analysis.14 For comparisons of inter-rater reliability using the κ statistic, κ≥0.61 was considered substantial and κ≥0.81 almost perfect.15 p Values of ≤0.05 were considered statistically significant.
Results
Patient demographics
Of the 355 patients included in the analysis, 172 were women (48%) and 183 were men (52%). The mean age was 57.4±17.6 years (range 3–92).
SSS variants and stenoses
The mean diameter of the SSS increased in size as cortical veins drained into the sinus from proximal to distal (figure 2). The mean diameter of the SSS was larger in men than in women (5.21±0.66 mm vs 4.57±0.67 mm, p<0.001). However, there was no significant difference in size based on the race of the patient (p=0.344). Arachnoid granulations were present within the SSS in 178 patients (50%).

{kind=link}
{kind=link}
Mean diameters and distribution of stenoses throughout the dural venous sinuses. Arach Gran, arachnoid granulations; Dia, dameter.
Twenty-three patients (7%) had a stenosis of their SSS. The mean diameter of the stenosed segment of the SSS was 2.24±0.82 mm with a mean length of 9.4±4.4 mm. Arachnoid granulations were present in 20 of the 23 stenotic SSSs (87%).
The SSS preferentially drained to the right transverse sinus (RTS) in 174 cases (51%) and to the left transverse sinus (LTS) in 58 patients (17%). In 112 cases (33%) the SSS drained equally to both transverse sinuses.
Transverse sinus anatomy
The mean diameter of the transverse sinuses increased slightly distal to the vein of Labbe (figure 2). Overall, the mean diameter of the LTS (5.07±1.27 mm) was significantly smaller than the mean diameter of the RTS (5.95±1.19 mm) (p<0.001). Accordingly, the RTS was dominant in 47% of the cases, the LTS was dominant in 13% of cases, and the sinuses were co-dominant in 40% of cases. Women were statistically more likely to have a smaller mean diameter of their LTS (4.66±1.20 vs 5.47±1.19, p<0.001) and RTS (5.57±1.12 vs 6.30±1.16, p<0.001). The transverse sinuses were on average larger in Caucasian patients (5.17±1.30 mm on the left, 6.06±1.24 mm on the right) than in African-American patients (4.48±1.12 mm on the left, 5.53±0.89 mm on the right) (p=0.002 on the left, p=0.012 on the right).
Arachnoid granulations were identified within the LTS in 115 patients (32%) and within the RTS in 67 patients (19%).
Transverse sinus stenosis and hypoplasia
Seventy-nine of the patients included in the study (22%) had at least one stenosis (table 2, figure 2). More were identified in the LTS (n=61, 17%) than in the RTS (n=34, 10%) (p=0.004). The majority of all stenoses resulted in an abrupt caliber change (n=65, 68%). The mean diameter of the stenosed segment of the transverse sinus was 2.04±0.43 mm on the left and 2.19±0.49 mm on the right. The mean length of a stenosis was 15.54±12.28 mm in the LTS and 16.51±12.53 mm in the RTS. Arachnoid granulations were present in the majority of sinuses that had a stenosis (77% on the left and 71% on the right).
Prevalence of transverse sinus stenosis and hypoplasia among the 355 included patients
In total, 20 patients (6%) may be predisposed to elevated venous pressures. Sixteen patients (5%) had bilateral transverse sinus stenoses (BTSS) and four patients (1%) had a unilateral stenosis with a hypoplastic contralateral transverse sinus. Of note, in all four of those cases, the stenosis was in the RTS while the LTS was hypoplastic. Patients with BTSS or unilateral stenosis with hypoplasia of the contralateral side were more likely to have arachnoid granulations (90%) than patients with unilateral or no stenosis (31%) (p<0.001). There was also a trend toward more women having BTSS than men, although this was not statistically significant (p=0.107).
A multivariate analysis identified increasing age (p=0.008) and the presence of arachnoid granulation (p<0.001) as predictors of BTSS (p<0.001). Neither gender (p=0.332) nor race (p=0.483) were significant predictors of stenosis when controlling for other factors.
Inter-reader agreement
The inter-reader agreement on the presence or absence of transverse sinus stenoses ranged from 91% to 95%. Fleiss κ was 0.756 for the LTS and 0.824 for the RTS.
Discussion
Previous studies have suggested that the prevalence of BTSS ranges from 23% to 93% in IIH.1–3 However, it is difficult to appreciate the magnitude of these numbers without first understanding the prevalence of BTSS in the general population.
Prior to evaluation of the sinuses, a standardized definition of what constitutes a stenosis and hypoplasia must be agreed upon. Marmarou et al developed a model of the CSF system that incorporated intracranial compliance, dural sinus pressure, resistance to absorption, and CSF formation.12 This model demonstrated excellent prediction of intracranial pressure with changes in the CSF volume. Stevens et al13 incorporated a Starling-like resistor into the model to predict the effect of a collapsible sinus on intracranial pressures. A study validating this model showed that patients with a transverse sinus stenosis of >40% have two stable pressure states.16 The lower state represents normal CSF pressure. However, a perturbation in arterial inflow or an increase in CSF volume can cause a transition to the upper steady state consistent with the elevated intracranial pressures seen in patients with IIH. Based on this work, a 40% reduction in caliber of the vessel was defined as a stenosis. Similarly, a sinus that was 40% smaller in average caliber than the contralateral sinus was defined as a hypoplastic sinus.
After screening 600 patients, 355 were included in this study. This is believed to represent the largest such investigation into the prevalence of unilateral and bilateral transverse venous sinus stenosis in the literature. Based on the above definition of a stenosis and hypoplastic sinus, 18% of patients had a unilateral stenosis, 16% had a unilateral hypoplastic sinus, 5% had BTSS, and 1% of patients had a unilateral stenosis with hypoplasia of the contralateral transverse sinus. In the largest study of ‘normal’ patients to date, a flow gap in the transverse sinus was identified in 31% of 100 patients with a normal MRI, a total similar to that identified in the current study.17
In total, approximately 6% of the patient population in this study demonstrated either BTSS or a unilateral stenosis with contralateral hypoplasia. Small studies (ranging from 40 to 59 patients) have estimated a similar prevalence of BTSS in control patients, ranging from 0% to 7%.2 ,18 ,19 This gives context to the prevalence of BTSS of >90% described in previous studies of patients with IIH.2 ,3 Similarly, patients with IIH without papilledema (IIHWOP) who suffer from unresponsive chronic headaches and patients with monosymptomatic tinnitus have been found to have increased prevalence of BTSS at 49% and 18%, respectively.20 ,21 One could infer that MR venography (MRV) or CTV may be warranted as part of the initial investigation for a patient with any of these conditions. Conversely, patients with IIHWOP who have responsive chronic tension-type headaches or migraines have been found to have a BTSS prevalence of 9% and 7%, respectively.4 ,22 The prevalence in these conditions is similar to that in the general population, suggesting that BTSS as either a contributor to or result of the condition may be less likely.
Recent studies into the etiology of IIH have suggested a correlation with the presence of arachnoid granulations, septae, or congenital stenosis.2 ,8 ,23 Our findings support the theory that arachnoid granulations tend to be associated with transverse venous sinus stenosis. Arachnoid granulations were identified in 70% of patients with a unilateral stenosis, while only 18% of patients with no transverse sinus stenosis had arachnoid granulations. It should be noted that, in many cases where arachnoid granulations were present in a stenotic sinus, it was the overgrowth of the arachnoid granulation that caused the potential impediment of flow through the transverse sinus. Previous studies have indicated that arachnoid granulations form as intracranial pressure increases,24 which could lead to a positive feedback mechanism. The increasing size of the arachnoid granulation could lead to impediment of flow out of the dural venous sinuses, which in turn leads to elevated venous pressures. As previously demonstrated, this leads to resistance to CSF absorption with a concomitant increase in CSF pressure to restore the pressure gradient,25 which could then lead to further increase in arachnoid granulation overgrowth.
Cadaver studies have demonstrated the presence of arachnoid granulations and septa of varying sizes in otherwise normal appearing transverse sinuses,9 ,26 potentially as a consequence of the coalescence of embryonic venous plexus into the dural venous sinuses during early development of the fetus.27 It stands to reason that smaller transverse sinuses are more susceptible to stenoses, as the septa or arachnoid granulation have a lower threshold to reach before growth leads to obstruction. This theory is, in part, supported by the observations in this study that the smaller LTS is significantly more likely to have a stenosis than the larger RTS.
Recent literature has suggested that race may be a predictor of worse visual outcomes in patients with IIH.28 This study identified no significant difference in the prevalence of transverse sinus stenosis between different races when accounting for the presence of arachnoid granulation and the sex of the patient. However, the data do demonstrate a significant difference in the overall mean diameter of the transverse sinuses when comparing Caucasians with African-Americans. It is conceivable that the smaller transverse sinuses could lead to more significant elevations in perfusion pressure when a 40% stenosis occurs based on Bernolli's equation. In turn, this could lead to worse visual symptoms in African-American patients for a given degree of stenosis when compared with Caucasian patients.
CTA may seem an unconventional choice for evaluation of the venous system. However, CTV or MRV would impart a significant selection bias into the results, as they are typically performed in people in whom venous pathology is suspected and therefore are not representative of the general population. MRV in controls would seem a good option. However, MRV signal intensity can suffer due to in-plane saturation effects and the slow turbulent flow found in the transverse sinuses.29 MRA does not routinely opacify the venous structures and post-contrast MPRAGE or other 3D sequences have not been validated in a systematic way for the evaluation of the vascular system. In the end, CTA makes a reasonable choice for an assessment of the ‘general population’ at our institution as we tend to perform CTAs for all suspected strokes, many of our trauma patients, and anyone suspected of having a vascular disorder.
There are a few additional potential limitations to this study, the most significant of which is the assumption that patients can simulate the general population. In an effort to overcome this limitation, any patient with venous imaging was excluded due to the higher pre-test probability of the presence of venous pathology. In addition, any patient with a mass, stroke, fracture, or hemorrhage that could conceivably alter venous outflow was excluded. Past medical history of suspected or confirmed IIH, tinnitus, acute or refractory headaches, multiple sclerosis, recent lumbar puncture, or any change in vision also resulted in exclusion. Any observable mass effect, including tonsillar or uncal herniation and midline shift, were immediately excluded regardless of cause. Another limitation is the distribution of men to women in this study compared with the IIH patient population. However, gender was not found to be a significant factor in the prediction of stenosis in a multivariate analysis. Additionally, the study is retrospective and suffers all of the limitations therein. This includes the lack of dedicated venous imaging in a control population. Finally, as a single-center study, the data would need to be replicated at another center to verify the conclusions of the study.
Conclusion
The prevalence of unilateral transverse sinus stenosis or hypoplasia in a sample of patients representing the general population was 33%, while the prevalence of BTSS was 5% and the prevalence of unilateral stenosis with contralateral hypoplasia was 1%. Once these data are verified, future researchers may be able to use the data as a reference for understanding and comparing the prevalence of BTSS in patients with various disease processes such as IIH, tinnitus, and medical refractory headache.
Acknowledgments
We would like to acknowledge the role of Claire McKinley and Thomas Tandy in helping to complete this project. Both were instrumental in obtaining regulatory approval and keeping the project on time.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work: CRD, RMS, MW, AE, MEJ, RWC, JG and KCL. Acquisition of data: CRD, DAO, MAR, PM and SM. Analysis/interpretation of data: CRD and RMS. Drafting the manuscript: CRD and RMS. Revising the manuscript: All authors. Final approval: All authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: All authors.
Competing interests JG is a consultant for Covidien, Microvention, and Stryker. MEJ receives payment for lectures from Stryker and Covidien. AE is a consultant for Stryker and Covidien. He received a research grant from Stryker. He receives royalties from Cook and CareFusion.
Ethics approval This study was approved by the University of Virginia Institutional Review Board with a waiver for informed consent. Patient information was handled in accordance with HIPAA regulations.
Provenance and peer review Not commissioned; externally peer reviewed.