Article Text

Abstract
Background Cerebral arteriovenous malformations (AVMs) are uncommon vascular lesions, and hemorrhage secondary to AVM rupture results in significant morbidity and mortality. AVMs may be treated by endovascular embolization, and technical advances in microcatheter design are likely to improve the success and safety of endovascular embolization of cerebral AVMs.
Objective To describe our early experience with the Headway Duo microcatheter for embolization of cerebral AVMs with n-butyl-cyanoacrylate (n-BCA).
Methods Consecutive patients treated by endovascular embolization of a cerebral AVM with n-BCA delivered intra-arterially through the Headway Duo microcatheter (167 cm length) were identified. Patient demographic information, procedural details, and patient outcome were determined from electronic medical records.
Results Ten consecutive patients undergoing cerebral AVM embolization using n-BCA injected through the Headway Duo microcatheter were identified. Presenting symptoms included headache, hemorrhage, seizures, and weakness. Spetzler Martin grades ranged from 1 to 5, and AVMs were located in the basal ganglia (2 patients), parietal lobe (4 patients), frontal lobe (1 patient), temporal lobe (1 patient), an entire hemisphere (1 patient), and posterior fossa (1 patient). 50 arterial pedicles were embolized, and all procedures were technically successful. There was one post-procedural hemorrhage that was well tolerated by the patient, and no other complications occurred. Additional AVM treatment was performed by surgery and radiation therapy.
Conclusions The Headway Duo microcatheter is safe and effective for embolization of cerebral AVMs using n-BCA. The trackability and high burst pressure of the Headway Duo make it an important and useful tool for the neurointerventionalist during cerebral AVM embolization.
- Arteriovenous Malformation
- Liquid Embolic Material
- Catheter
Statistics from Altmetric.com
Introduction
Cerebral arteriovenous malformations (AVMs) are uncommon developmental or congenital lesions that are characterized by the presence of a vascular nidus and abnormal arteriovenous shunting.1 ,2 Cerebral AVMs may come to clinical attention through intracranial hemorrhage, seizures, headaches, focal neurologic deficits, or they may be incidentally identified.2–7 Intracranial hemorrhage occurs in up to 50% of patients and results in significant morbidity and mortality in 10–40% of patients.2 ,4 ,8 There is ongoing debate as to whether unruptured cerebral AVMs should be treated, but most neurointerventionalists and neurosurgeons believe that the 4% annual risk of cerebral AVM hemorrhage warrants treatment in most patients.6 ,9
Cerebral AVM treatment includes surgical resection, endovascular embolization, radiosurgery, or a combination of these modalities.10 Endovascular embolization continues to play an important role in the treatment of AVMs, and it may be used to eliminate high-flow fistulas within the AVM nidus, secure a nidal aneurysm, decrease the size of the AVM nidus, and decrease the arterial supply to the AVM, all of which facilitate subsequent surgical resection or radiation therapy. Endovascular embolization has also been described as a sole treatment modality for AVMs.11
Endovascular embolization may be performed by injecting n-butyl-cyanoacrylate (n-BCA) (TRUFILL; Codman DePuy Synthes, Raynham, Massachusetts, USA) or ethylene vinyl alcohol (Onyx; Covidien, Minneapolis, Minnesota, USA) through a microcatheter positioned in a cerebral artery that supplies the AVM.10 ,12 The embolic agent exits the microcatheter and fills the nearby AVM nidus. Embolization results in occlusion and thrombosis of the treated AVM nidus with associated decreased arteriovenous shunting. The most significant complications that occur during or following endovascular embolization include post-procedural hemorrhage or stroke in approximately 5–6% of patients.12 If a flow-directed microcatheter is used for endovascular embolization, there is a small risk of catheter rupture with non-targeted embolization given the relatively low burst pressure of these catheters.13
Continued advances in microcatheter design have led to more navigable catheters that allow for microcatheter advancement through significant vessel tortuosity into the distal intracranial circulation. Here we describe our early experience at a single center with the Headway Duo microcatheter (MicroVention, Tustin, California, USA) in the embolization of cerebral AVMs with n-BCA.
Materials and methods
Our hospital's Institutional Review Board approved this study, which complied with the Health Insurance Portability and Accountability Act.
We retrospectively reviewed our internal database and identified all patients undergoing endovascular embolization of a cerebral AVM using n-BCA injected through a 167 cm Headway Duo microcatheter from July 2014 to September 2015. At our institution, nearly all cerebral AVM embolizations are performed with n-BCA due to institutional preferences. Patient demographic information and outcomes were obtained by electronic medical record review.
All procedures were performed using a Siemens Artis Zee biplane system in a dedicated neuroangiography suite. Procedures were performed under monitored anesthesia care or general anesthesia with neurophysiologic monitoring. Mean arterial pressures were maintained in the range of 60–80 mm Hg during the embolization procedure and for a 24 h period in the intensive care unit following embolization.
The common femoral artery was accessed with a 6 Fr shuttle SL sheath (Cook Medical, Bloomington, Indiana, USA). Intravenous heparin was administered to achieve an activated clotting time of 250–300 s after arterial access was obtained. Diagnostic cerebral angiograms were performed with a 5 Fr Berenstein II catheter (Cook Medical) positioned in the internal carotid artery (ICA) or the vertebral artery. Prior to endovascular embolization, the Berenstein II catheter was removed and replaced with a 115 cm or 125 cm 5 Fr Sofia distal access catheter, which was advanced into the supraclinoid ICA or the V4 segment of the vertebral artery. A 167 cm Headway Duo microcatheter was then advanced through the Sofia distal access catheter over either a 0.014 inch Traxcess (MicroVention) or a Synchro 2 (Stryker, Alameda, California, USA) microwire proximal to the AVM nidus.
In some instances the microwire was withdrawn into the Headway Duo microcatheter and positioned several centimeters proximal to the microcatheter tip while it was advanced into the distal intracranial circulation. The distal tip of the Headway Duo was found to be very soft and to behave in a similar manner to a flow-directed microcatheter during advancement toward the AVM nidus. Additionally, agitation of the microwire during advancement of the microcatheter tip (a modified Dottering technique) seemed to accentuate the flow-directed properties of the microcatheter tip.
Appropriate microcatheter position was confirmed by superselective contrast injection and the absence of neurophysiologic monitoring changes following intra-arterial methohexitol (Brevital) injection through the microcatheter. Prior to endovascular embolization, the Headway Duo microcatheter was flushed with approximately 20 mL of D5 (dextose 5% in water) solution to remove any ionic solution within the catheter. The n-BCA was diluted by mixing with ethiodol based upon the proximity of the microcatheter to the AVM nidus and the rate of flow through the AVM; typical dilutions of n-BCA:ethiodol were 1:1–1:3. Endovascular embolization was performed by injection of n-BCA through the Headway Duo using continuous fluoroscopic and roadmap guidance. Once adequate embolization of the AVM nidus was achieved, slight negative pressure was applied to the syringe and the microcatheter was rapidly removed from the Sofia distal access catheter.
Results
Ten consecutive patients (7 women, 3 men) who underwent endovascular embolization of a cerebral AVM with n-BCA injected through the Headway Duo microcatheter were identified. The mean patient age was 25 years. Four patients presented with intracranial hemorrhage (40%), three with headaches (30%), two with seizures (20%), and one with upper and lower extremity weakness contralateral to the AVM (10%). The AVMs ranged in Spetzler–Martin grades from 1 to 5 and were located in the basal ganglia (2 patients; 20%), parietal lobe (4 patients, 40%), frontal lobe (1 patient; 10%), temporal lobe (1 patient; 10%), the right cerebral hemisphere (1 patient; 10%), and the posterior fossa (1 patient; 10%). These data are summarized in table 1. Representative examples are shown in figures 1 and 2.
Demographic and clinical details of patients with cerebral AVM treated with n-BCA and the Headway Duo Microcatheter
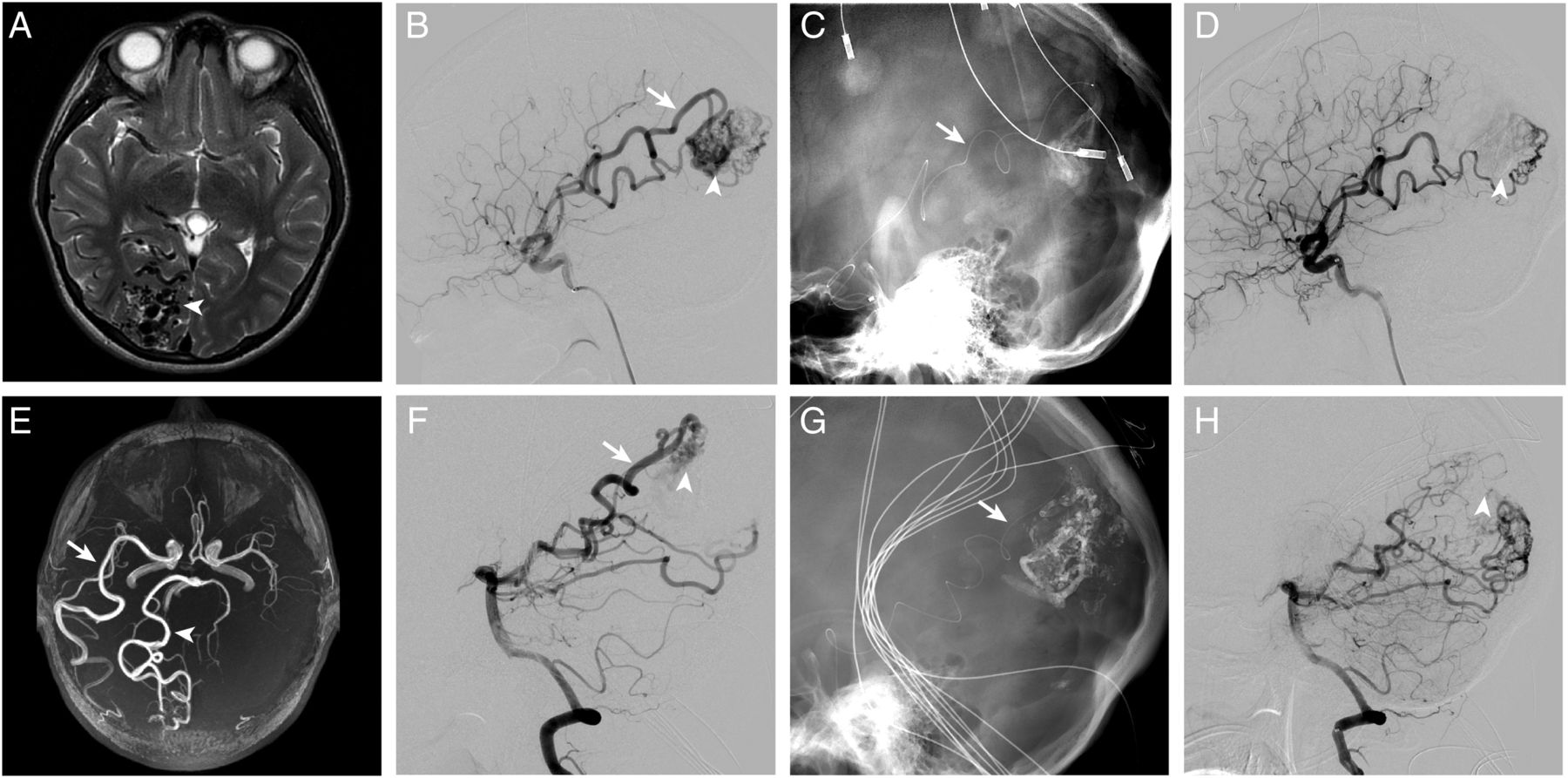
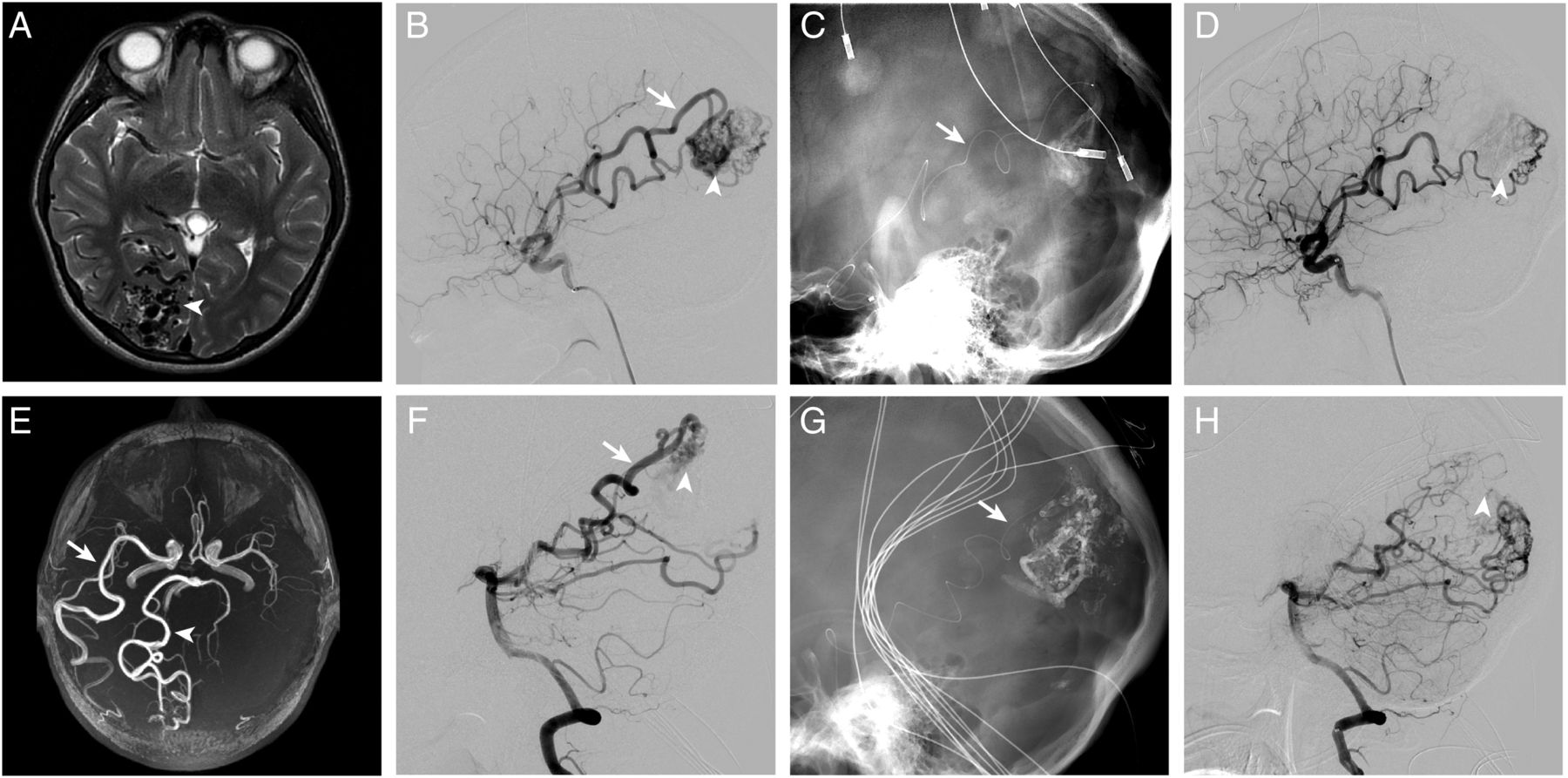
Parietal and occipital lobe arteriovenous malformation (AVM) embolized from middle cerebral artery (MCA) and posterior cerebral artery (PCA) pedicles. A T2-weighted MR image shows multiple flow voids (A, arrowhead) and the MR angiography image shows an enlarged right MCA pedicle (E, arrow) and right PCA pedicle (E, arrowhead) supplying an AVM in the right parietal and occipital lobes. Digital subtraction angiography after right internal carotid artery (B) and right vertebral artery (F) injections shows an enlarged inferior division right MCA pedicle (B, arrow) and an enlarged right parieto-occipital artery pedicle arising from the right PCA (F, arrow) supplying a right parietal lobe AVM (B and F, arrowheads). Fluoroscopic image shows a Headway Duo microcatheter (C and G, arrows) traversing extreme tortuosity in the MCA (C, arrow) and parieto-occipital artery (B, arrow) pedicles supplying the AVM. Following embolization, there is a marked decrease in the size of the AVM nidus (D and H, arrowheads).

{kind=link}
{kind=link}
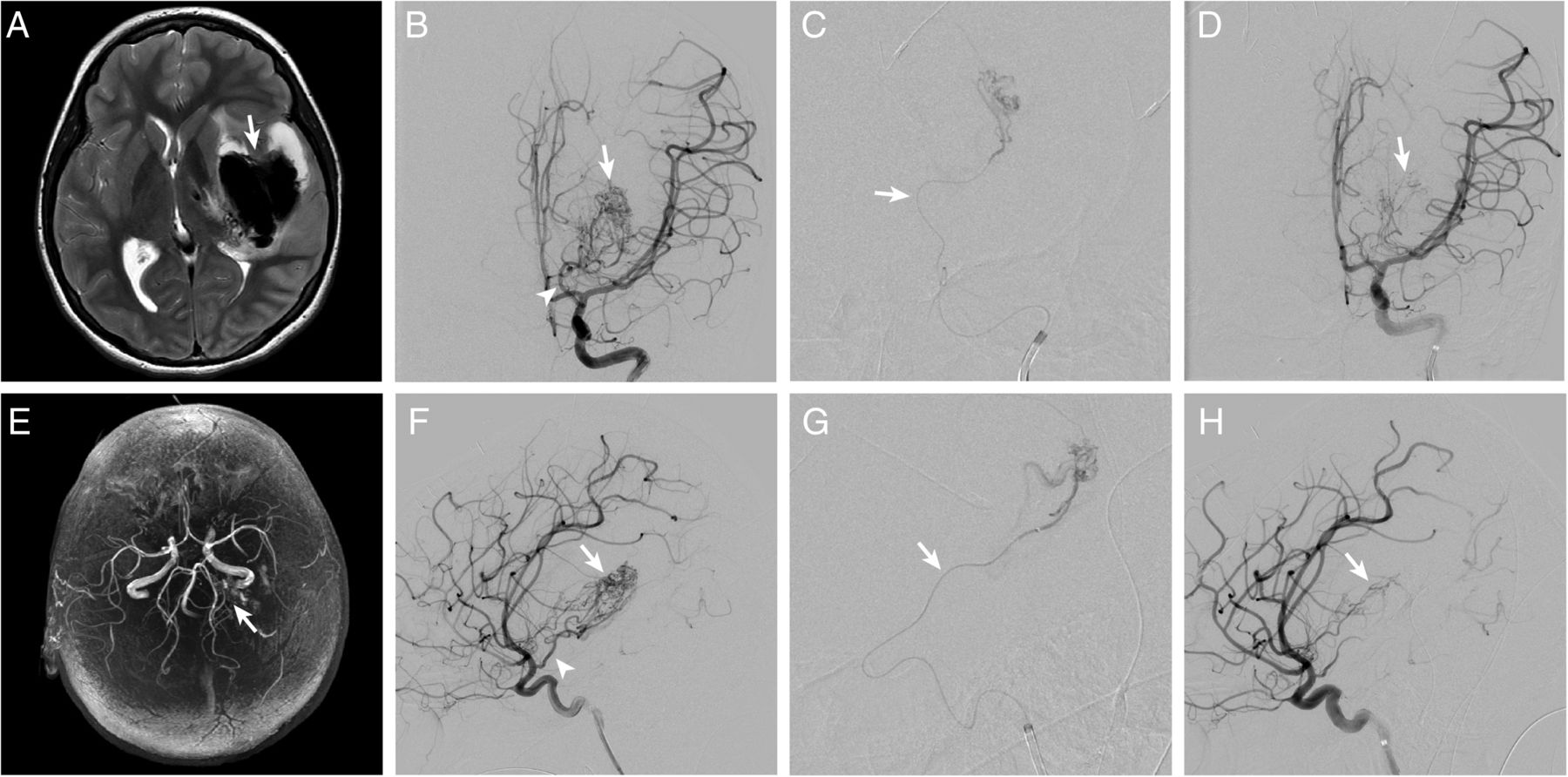
Basal ganglia arteriovenous malformation (AVM) embolized from anterior choroidal artery pedicles. An MR image shows a large intraparenchymal hemorrhage (A, arrow) centered in the left basal ganglia and the MR angiography image shows increased vascularity in the region of the hemorrhage (E, arrow), which suggests the presence of an underlying AVM. Anteroposterior (B) and lateral (F) digital subtraction angiography after left internal carotid artery injection shows an AVM (B and F, arrows) with arterial supply arising from hypertrophied anterior choroidal artery pedicles (B and F, arrowheads). Superselective digital subtraction angiography through a Headway Duo microcatheter (C and G, arrows) positioned in an anterior choroidal artery pedicle demonstrates filling of the posterolateral aspect of the AVM. Following embolization there is no significant residual arteriovenous shunting through the embolized AVM nidus (D and H, arrows).
All patients underwent endovascular embolization using n-BCA injected through a 167 cm Headway Duo microcatheter. A total of 50 arterial pedicles were embolized, and multiple arterial pedicles were embolized in each patient (range 3–9) in a single or in multiple sessions (see table 2). All embolization procedures were technically successful. There was one post-procedural hemorrhage (out of 32 sessions; 3%) that was well tolerated by the patient, and no other complications occurred. There were no instances of microcatheter rupture or of the Headway Duo being glued into a vessel after embolization.
AVM embolization treatment details
Following embolization, there was an angiographic cure of a single AVM; however, this AVM recurred on a 6-month follow-up angiogram. This recurrent AVM and the residual AVMs in other patients were treated by surgical resection with a complete cure in four patients and radiosurgery in four patients. Two additional patients have not yet undergone planned radiosurgery at the time of writing. Patients treated by radiosurgery have not had follow-up angiograms to assess for any residual AVM at this time.
There were no patient deaths in this series. One previously normal patient who presented with an intracranial hemorrhage was discharged with a modified Rankin Scale (mRS) score of 4, but improved to mRS 1 after 3 months. All other patients had no change in their baseline mRS score (range 0–3) from admission to discharge and at 3 months of follow-up when available.
Discussion
Endovascular embolization is an important modality in the treatment of cerebral AVMs. Transarterial embolization with n-BCA or Onyx can decrease blood flow through an AVM and reduce the vascular nidus size, which facilitates subsequent surgical resection or radiosurgical treatment.10 ,12 However, cerebral AVMs may cause significant cervical and cerebral vascular tortuosity due to the high blood flow through these lesions that may limit the neurointernventionalist's ability to perform safe embolization. Highly trackable microcatheters with a small profile are necessary to navigate vascular tortuosity and safely perform AVM embolization. Here we describe our initial experience in the embolization of cerebral AVMs using intra-arterial n-BCA injection through the Headway Duo microcatheter.
The Headway Duo microcatheter performed extremely well during the endovascular embolization procedures. All 41 arterial pedicles were accessed successfully using the Headway Duo, and we found the microcatheter to be very trackable in navigating significant vessel tortuosity. The 167 cm length of the Headway Duo facilitated selection of very distal arterial pedicles that other microcatheters may be unable to access due to length constraints. The ability to use a tapered 0.014 inch microwire rather than the less steerable 0.008 inch microwire that is used with most flow-directed microcatheters also facilitated microcatheter navigation through significant vessel tortuosity and the selection of distal arterial pedicles.
The small distal tip of the Headway Duo (1.6 Fr) accentuated the navigability of the microcatheter and allowed for selection and embolization of distal and small arterial pedicles. We also observed that the distal tip of the microcatheter demonstrated some flow-directed properties, which were capitalized on when advancing the Headway Duo toward the AVM nidus without a leading guidewire. Thus, the Headway Duo exhibits hybrid properties of a wire-directed and flow-directed microcatheter. These properties have made the Headway Duo one of the most used microcatheters in our institution.
There were no intra-procedural complications in this series. The absence of vessel perforation or intra-procedural AVM rupture confirms the safety and navigability of the Headway Duo. n-BCA is a cohesive liquid embolic agent, and there is a risk of the microcatheter tip becoming stuck in the n-BCA cast during embolization.14 However, there were no instances of the Headway Duo becoming ‘glued’ to the artery wall during embolization in this series. Rupture of flow-directed microcatheters proximal to the microcatheter tip with associated non-target n-BCA embolization is a rare but severe complication.14 There were no instances of Headway Duo microcatheter rupture in our series. The burst pressure of the Headway Duo is 700 psi, which is significantly higher than the 70–100 psi burst pressure of most flow-directed microcatheters. Therefore, rupture of the Headway Duo would be a highly unlikely event. There was one post-procedural hemorrhage (3% of embolization procedures) that was well tolerated by the patient. This low rate of peri-procedural hemorrhage and complication rate is lower than that reported in larger series following AVM embolization.12
At our institution, cerebral AVM embolization is almost exclusively performed using n-BCA due to physician preferences. Onyx has been shown to be an excellent embolic agent in the treatment of cerebral AVMs, and we would expect the Headway Duo microcatheter to perform similarly when using Onyx as a liquid embolic agent in cerebral AVM embolization. It would also be of interest to compare the performance of the Headway Duo with detachable tip microcatheters during cerebral AVM embolization.
There are a few disadvantages of the Headway Duo microcatheter. First, although the Headway Duo can be advanced over a 0.014 inch microwire, it performs best when the microwire tapers distally to a 0.012 inch size (such as with the Traxcess microwire). The use of a non-tapered 0.014 inch microwire incurs a theoretical risk of shearing of the hydrophilic microwire coating. Next, although the 156 cm Headway Duo has a coil marker, the 167 cm Headway Duo does not. The lack of a distal coil marker on the longer microcatheter can be a disadvantage in the rare event that a coil must be placed as a means of embolization or facilitate subsequent liquid embolic agent embolization. The addition of a coil marker may also facilitate the use of the 167 cm Headway Duo in the treatment of distal cerebral aneurysms (such as pericallosal artery aneuryms), for which the trackability of this microcatheter would be a significant advantage. Future generations of this device may address these shortcomings.
In summary, we found the Headway Duo to be a highly trackable microcatheter with a small distal tip that exhibits hybrid properties of a microwire-guided and flow-directed microcatheter. It will be of interest to assess further the performance of the Headway Duo in a larger number of patients and in the treatment of other vascular pathologies, such as dural arteriovenous fistulas and high-flow congenital vascular lesions.
Conclusions
Cerebral AVM embolization with n-BCA injection through the Headway Duo microcatheter is safe and effective. The excellent trackability, small profile of the microcatheter tip, and the newly appreciated flow-directed properties of the microcatheter tip facilitated successful embolization of arterial pedicles arising from cerebral vessels.
References
Footnotes
Contributors All authors made substantial contributions to the conception and design of the study, acquisition of data, or analysis and interpretation of data.
Competing interests HMD received consulting funds from MicroVention.
Ethics approval Ethics approval was obtained from Stanford Medical Center IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Published and unpublished data may be shared for additional publications pending the authors’ agreement to a research collaboration when appropriate.