Article Text

Abstract
Background The low profile visualized intraluminal support (LVIS) device is a new generation of self-expanding braided stents recently introduced into China for stent assisted coiling of intracranial aneurysms. This study assessed the clinical safety and efficacy of the LVIS stent for embolization of intracranial saccular aneurysms.
Methods Patients with intracranial saccular aneurysms treated using the LVIS device in our center between April 2014 and December 2014 were reviewed. The primary outcomes were procedural safety, target aneurysm recurrence, and mid-term follow-up of clinical and angiographic outcomes.
Results 97 patients with intracranial saccular aneurysms were treated using the LVIS stent, with 100% technical success rate. No mortality was observed. One patient had transient deficit (1/97, 1.0%). Immediate angiographic outcome evaluation showed complete occlusion in 28 (28.8%) and neck remnant in 39 (40.2%) of the 97 patients, respectively. Of the 76 (78.35%) patients who underwent angiographic follow-up at a mean of 8.1 months, complete occlusion was achieved in 64 (84.2%) patients. In the remaining patients, neck remnant in nine (11.8%) and residual sac in three (4%) patients were observed. None of the patients had any target aneurysm recurrence, and the mortality rate was 0%.
Conclusions The LVIS stent is safe and effective in the treatment of intracranial saccular aneurysms.
- Aneurysm
- Angiography
- Stent
- Intervention
Statistics from Altmetric.com
Introduction
Primary coiling for wide necked or complex aneurysms remains a technical challenge, and controversy still exists regarding its long term stability.1 Compared with primary coiling, stent assisted coiling may reduce recurrence rates and offers benefits with respect to the mechanical barrier, flow diversion, and biological effects.2
The low profile visualized intraluminal support (LVIS) stent (MicroVention Terumo, Tustin, California, USA), a new device offering an option between conventional coil assist stents and flow diverters, was designed to improve the long term efficacy of endovascular treatment while avoiding impact on side branches. The LVIS is a self-expanding closed cell stent, braided with a single nickel titanium wire. It has two flared ends with proximal and distal radiopaque markers, and double helical tantalum strands to assist full length visualization. The small cell size (<0.9 mm) provides better parent artery protection against small sized coils across the aneurysm neck. Its high metal to surface coverage (23% on average) facilitates improved flow diversion over other currently available coil assist stents.
However, its safety and efficacy still require further investigation. Hence this retrospective study was conducted to evaluate the safety and efficacy of embolization of intracranial saccular aneurysms assisted by the LVIS stent.
Materials and methods
This retrospective study was approved by the institutional review board at our hospital, and all patients signed general informed consent forms.
Patient population
Between April 2014 and December 2014, 368 aneurysms (347 patients) were treated with endovascular embolization, of which 171 aneurysms were treated with stent assisted coiling. Among them, patients treated with the LVIS stent were enrolled in the study. Patients with any of the following conditions were excluded: (1) dissecting or fusiform aneurysm, (2) retreated aneurysm, (3) Hunt–Hess grades IV or V, (4) aneurysm treated with stent alone, or (5) inability to give informed consent. A total of 97 patients were enrolled in the study. The study's primary endpoints included procedural safety, target aneurysm recurrence, and mid-term follow-up of clinical and angiographic outcomes. Target aneurysm recurrence was defined as any of the following conditions after the initial aneurysm coiling procedure: (1) target aneurysm hemorrhage, (2) target aneurysm retreatment, or (3) death from an unknown cause.
Endovascular procedure
All procedures were performed under general anesthesia. A 6 F guiding catheter was introduced through a femoral sheath into the carotid artery. Radiologic examination of target vessels was performed using a biplane angiographic system (Artis zee Biplane; Siemens, Erlangen, Germany). Rotational angiography followed by three-dimensional reconstruction was performed to assess the aneurysm and parent artery morphology for accurate measurement. Stent size selection mainly depends on the diameter of the parent artery. The LVIS device is available in three sizes (3.5, 4.5, and 5.5 mm in diameter) with varying lengths. The parent artery diameter at the proximal landing zone mostly dictates the stent size selection. LVIS performs optimally for vessels ≤1.5 mm smaller than the stent nominal size— for example, a 3.5 mm LVIS is recommended for vessel sizes from 2.0 to 3.5 mm. In addition, the stent should be sized as close as possible to the parent artery diameter. The same rules apply to 4.5 and 5.5 mm LVIS. Adequate LVIS device length (7 mm) on each side of the aneurysm neck needs to be maintained to ensure appropriate neck coverage.
The stenting strategies in our series were as follows: (1) semi-jailing technique (86 patients): stents were partially deployed (semi-jailing) to cover the aneurysmal neck after introducing part of the framing coil; additional coils were introduced through the ‘jailed’ microcatheter to embolize the aneurysms; the stent was then fully deployed. (2) Bailout stent placement (11 patients): when conventional coiling failed and coils protruded into the parent artery, stenting was considered to restore blood flow in the parent artery.
Anticoagulation and antiplatelet management
All patients received systemic heparin after sheath placement. The activated clotting time was maintained at 2–3 times of baseline throughout the procedure. If stent placement was planned for patients with remote subarachnoid hemorrhage or unruptured aneurysms, dual antiplatelet drugs (aspirin 100 mg/day plus clopidogrel 75 mg/day) were administered for 3 days before the procedure. Preprocedural thromboelastography was routinely performed to evaluate platelet aggregation inhibition. However, for patients with acutely ruptured aneurysms within 72 h, a loading dose of clopidogrel and aspirin (300 mg each) was administered orally by gastrointestinal tube or per rectum 2 h before stenting. A daily dose of aspirin (100 mg) and clopidogrel (75 mg) was recommended for 6 weeks postprocedure, followed by aspirin only, indefinitely.
Clinical and angiographic follow-up
Follow-up MR angiography (MRA) was typically scheduled at 3 months, with DSA at 6 months, and with MRA or DSA yearly thereafter. Clinical outcomes were assessed at discharge and at the 6 month follow-up using the modified Rankin Scale (mRS). Angiographic images were obtained before, immediately after treatment, and at the 6 month follow-up. A simplified 3 point Raymond Scale (total occlusion, neck remnant, and residual sac) was used to assess the results of the procedure. Two experienced neurologists performed clinical evaluations and follow-up assessments. Angiographic evaluations were conducted by two interventional neurosurgeons (QH and JL).
Results
Study population
A total of 97 patients (57 women and 40 men; mean age 57.3 years) with 107 intracranial aneurysms were included. Clinical and demographic patient data are summarized in table 1. Eight patients suffered multiple aneurysms. Of the 97 saccular aneurysms treated using the LVIS stent, 13 were ruptured ones; the rest were unruptured. Among these 13 patients, 6 were grade I, 4 were grade II, and 3 were grade III, according to the Hunt–Hess grading scale. Based on the maximum aneurysm diameter, there were 13 tiny aneurysms (<3 mm), 54 small aneurysms (3 mm ≤ aneurysm <10 mm), 29 large aneurysms and 1 giant aneurysm. Wide necked was defined as a dome to neck ratio <2 or neck diameter >4 mm. More information regarding these patients and the aneurysms is given in table 1.
Intracranial aneurysms treated and clinical and anatomic findings
Clinical safety and procedure related complications
Stents were successfully implanted in all 97 patients and were deployed in the desired locations, resulting in 100% technical success. The primary endpoint of safety (absence of any new transient or permanent deficit or death) was reached in 96 (98.9%) patients. Mortality or new permanent neurological deficits from hemorrhagic or ischemic stroke did not occur in any of the treated patients within 30 days after the intervention. One case of basilar artery aneurysm experienced acute in-stent thrombosis. Partial recanalization was achieved after intravenous tirofiban injection, and mild transient paresis of his left hand was observed the day after the procedure (figure 1).
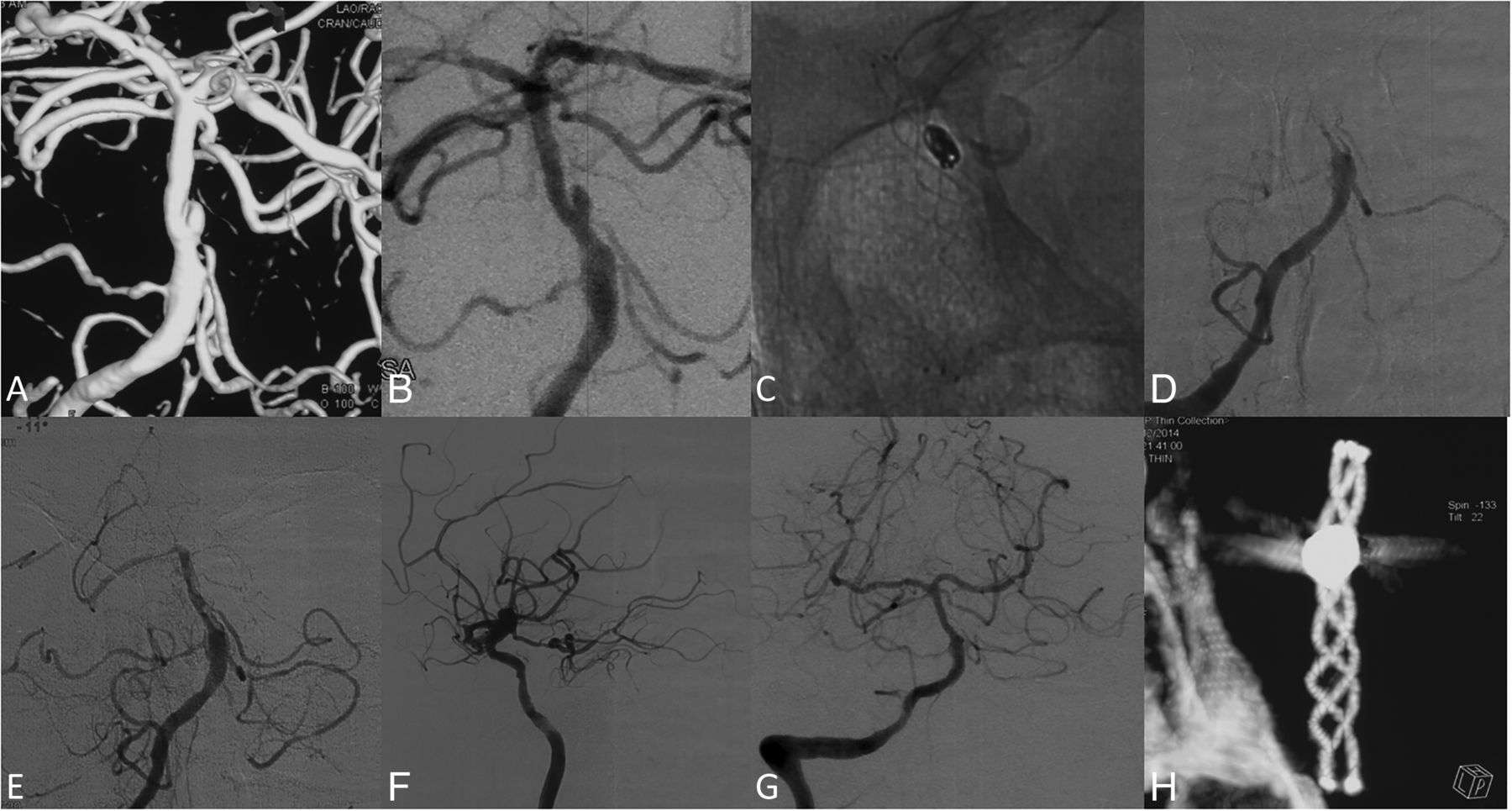
Angiograms of a 69-year-old man with an unruptured basilar artery (BA) aneurysm. (A) Three-dimensional reconstruction of the aneurysm. (B) The aneurysm in the working projection before treatment. (C) The 3.5 mm×24 mm LVIS stent being deployed. (D) Acute in-stent thrombus occurred during the procedure. (E, F) Partial recanalization was achieved after intravenous tirofiban injection. Compensation from the right internal carotid artery to the posterior circulation via the posterior communicating artery. (G, H) Total aneurysm occlusion with patency of the BA at the 8.1 month follow-up visit, with X-ray showing the stent fully opened.
Incomplete opening during initial stent deployment occurred in 10 (10.31%) patients; after retrieving and releasing the stent for repeated adjustment, 8 stents were fully opened under fluoroscopy, while the remaining 2 patients received further balloon dilatation. Immediate postprocedural angiograms showed complete occlusion in 28 patients, neck remnant in 39 patients, and residual sac in 30 patients. Clinical outcomes were assessed at discharge using the mRS. mRS scores at discharge were 0 in 78 patients, 1 in 16 patients, and 2 in 3 patients. Three patients developed groin hematoma after the procedure and recovered after hemostasis by compression; one bedridden patient developed pneumonia. No patient experienced gastrointestinal bleeding or myocardial infarction, and there was no mortality during the periprocedural period (table 2).
Stent implantation procedure characteristics and outcomes
Mid-term follow-up results
All patients were followed-up for 5.9–13.5 months (mean 7.8 months) and no new neurologic deterioration or death was observed. DSA follow-up was performed for 76 of 97 patients, at intervals ranging from 6.5 to 12.6 months (mean 8.1 months). According to DSA follow-up images of these 76 patients, complete occlusion was achieved in 45 (59.21%), neck remnant in 26 (34.21%), and residual sac in 3 (6.58%) patients. Among the remaining 21 patients, 13 underwent enhanced MRA follow-up without evidence of aneurysm recanalization. The parent vessels of all cases were patent, with no evidence of intimal hyperplasia or in-stent stenosis. In addition, branch arteries covered by the stents also maintained patency on follow-up angiography (figure 2).

{kind=link}
{kind=link}
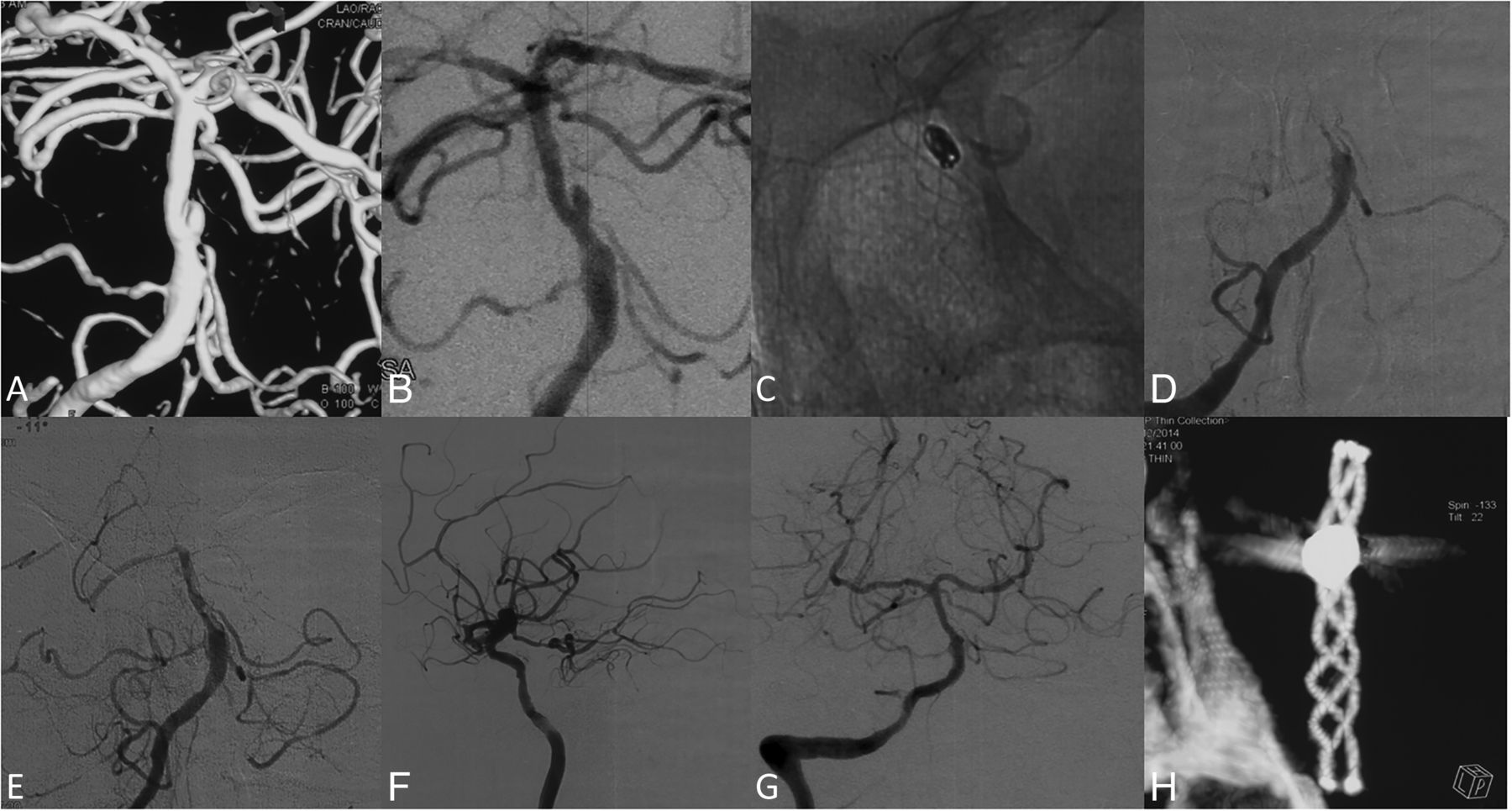
A 52-year-old man with a ruptured left middle cerebral artery (MCA) aneurysm treated with stent assisted coiling. (A) The aneurysm in the working projection before treatment. (B) The 3.5 mm×24 mm LVIS stent being deployed using the semi-jailing technique. (C, D) Immediate postprocedural angiogram revealed neck remnant with patency of the parent vessels. (E) Stent opened fully under X-ray. (F) Total aneurysm occlusion was achieved at the 6 month follow-up.
Discussion
Endovascular treatment of wide neck, complex, or giant aneurysms remains an ongoing challenge, typically requiring stent assisted coiling to reconstruct the parent artery.3 After introduction of the Neuroform stent (Stryker) for the treatment of aneurysms, other companies launched several types of intracranial stents, including Enterprise (Codman), Leo (Balt), and Solitaire (eV3). Even though these stents differ fundamentally, none is functionally or physically superior to other stents, and the selection of stents is mainly based on clinical and technical indications.4 ,5 The Enterprise stent, LEO stent and Solitaire stent use a closed cell design while the Neuroform stent uses an open cell design. The LEO and LVIS stents are braided stents, while the Enterprise, Solitaire, and Neuroform stents are laser cut stents. Laser cut stents usually have a much lower metal coverage rate than braided stents.
In this retrospective single center study, endovascular coiling with the LVIS stent appeared safe and effective for the treatment of intracranial aneurysms. Compared with previous studies reporting endovascular coiling with other stents, the use of the LVIS stent in this setting was associated with higher procedural success rate (100% vs 94% (Neuroform) and 96.9% (Enterprise)), lower complication rate (perioperative stroke incidence 1.0% vs 5.0% (Neuroform) and 4.2% (Enterprise)), and better mid-term angiographic results (complete occlusion rate 84.2% vs 69% (Neuroform) and 36% (Enterprise)).6 ,7 Compared with previous research on the LVIS stent, the complete occlusion rate at follow-up visits in this study was 84.2%, similar to those reported by Young Dae Cho et al8 and Wojciech Poncyljusz et al9 (82% and 92.6%, respectively). Recently, a prospective, multicenter trial of the LVIS for treatment of wide necked intracranial aneurysms was conducted by David Fiorella et al,10 and the technical success rate was 93.5%, without any major stroke or death within 30 days; 21/28 (75%) treated aneurysms with 6 month angiographic follow-up demonstrated complete occlusion.
Stents have been shown to improve the long term outcome of endovascular treatment of aneurysms; clinical follow-up showed that the probability of further thrombosis after stent implantation was 18.5 times that of non-stent assisted procedures.11 Compared with the balloon assisted therapy group, the follow-up results showed a significantly higher cure rate in the stent group (75.4% vs 50%), and significantly lower retreatment rate than the balloon group (4.3% vs 15.6%).11 ,12 However, conventional stent assisted coil embolization for large or giant aneurysms has high aneurysm recurrence rates, which may be related to the low metal coverage rates of the stents used in these procedures.5
The general endovascular treatment strategy of aneurysms has recently focused on reconstruction of parent vessels rather than on embolization of the aneurysm sac. In this context, flow diverters with a high metal coverage rate were invented for endovascular procedures; because of their excellent blood flow diversion, some large and complex aneurysms can be completely cured. However, the potential for branch vessel occlusion is relatively high, and may cause serious complications.13 ,14 Metal coverage rate is one of the most important characteristics of a stent. Stents with a low metal coverage rate cannot play a good role in diverting blood flow, but stents with too much metal coverage rate can affect branch vessels. The LVIS stent, which was recently developed for endovascular embolization of intracranial aneurysms, has a mean metal coverage rate of 23%, between those of conventional stents (6–11%) and flow diverters (30–35%). Compared with conventional intracranial stents, the LVIS provides better flow diversion effects, and hemodynamic changes after stenting have been shown to improve long term outcomes of endovascular treatment.15 As shown in this study, complete occlusion was initially achieved in 28.9% of aneurysms, progressing to 84.2% based on the last follow-up data.
Recently, the mid-term safety and durability of stent assisted coiling with LVIS and LVIS Jr stents have been investigated.8 ,9 We previously reported our preliminary experience with the LVIS Jr stent, in terms of the results of the immediate and mid-term follow-ups.16 ,17 In the current series, we evaluated the mid-term follow-up results of enrolled patients treated using only the LVIS device. In our study, the initial complete occlusion rate was 28.9% (28/97) overall, rising to 84.2% by a mean of 8.1 months of angiographic follow-up.
Thromboembolic events or vascular occlusions are major complications of stent assisted coiling of cerebral aneurysms; incomplete stent expansion is a common cause, particularly in wire braided stents.18 ,19 The currently available stents designed for intracranial aneurysms make it difficult to judge under fluoroscopy whether the stents are fully opened. In contrast, the LVIS stent offers good visibility: the proximal and distal ends are flared with four radiopaque markers, and its body contains two radiopaque helical strands, which ensures full length visualization under fluoroscopy. The success of the stent opening can be identified by observing the two helical strands. Additionally, the stent can be retrieved up to 80% of its length, and operators can make repeated adjustments during the procedure. Young Dae Cho et al8 and Wojciech Poncyljusz et al9 reported 9.0% and 8.9% incomplete stent expansion during procedures, respectively. In our study, initial segmentally incomplete stent expansion occurred in 10 (10.3%) cases; we retrieved the stent and unsheathed it again to achieve full opening in 8 patients, while the remaining 2 patients underwent further balloon dilatation. Acute in-stent thrombus occurred during the procedure in one patient with an unruptured basilar artery aneurysm; tirofiban was given through intravenous injection, and the patient suffered a mild transient paresis of his left hand after the procedure.
During endovascular aneurysm treatment, it is not uncommon for coils to protrude into the parent artery, particularly in relatively wide necked aneurysms; endovascular stenting has become an important bailout technology to solve this problem. The LVIS is a self-expanding braided stent developed for treatment of intracranial aneurysms. Whether the LVIS provides sufficient radial force compared with laser cut stents is a concern in clinical practice. Complications of the coil protruding into the parent artery in 11 cases were successfully resolved by deploying the LVIS stent. All stents opened optimally, which was confirmed by DynaCT, and the postoperative vessel patency rate was 100%.
Another advantage of the LVIS stent is small cell size (<0.9 mm); the average metal coverage can reach up to 23%, compared with 11% for Neuroform, 10% for Enterprise, and 6% for Solitaire stents.20 High metal coverage can provide a flow diversion effect, but also introduces concerns about branch vessel occlusion;21 due to the small cell size of the LVIS stent (<0.9 mm), physicians were concerned that the LVIS stent might influence blood flow in the branch arteries. However, follow-up angiography of 30 cases with branch vessels covered by stents revealed no branch vessel occlusion, indicating that the LVIS provides excellent protection of branch vessels, even with its tight mesh design.
In conclusion, this study retrospectively analyzed the safety and efficacy of the LVIS stent for endovascular treatment of intracranial saccular aneurysms. The results of this new generation intracranial stent are encouraging compared with other stents. A total of 97 stents were successfully deployed, without any permanent neurologic event. A much higher aneurysm complete occlusion rate at follow-ups was achieved by LVIS than other laser cut coil assist stents. However, this study had several limitations: the samples in this retrospective study were from a single institution and therefore patient selection bias is possible. The long term efficacy remains unknown due to the mid-term follow-up period in this study.
References
Footnotes
Contributors ZF and QH contributed equally to the preparation of the manuscript. ZF, YF, and WZ contributed equally to data collection. YX and BH contributed equally to clinical follow-up. QH and JL contributed equally to the interventional procedures.
Funding This research was supported by the Major Project of Shanghai Committee of Science and Technology (grant No 13411950300). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the institutional review board of Changhai Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.