Article Text

Abstract
Background Stent retriever thrombectomy has recently been found to be effective for anterior circulation strokes, but its efficacy for basilar artery occlusion (BAO) is unclear.
Objective To carry out a systematic review and meta-analysis to analyze the available evidence for the use of stent retrievers for BAO.
Methods Two independent reviewers searched six databases for studies reporting outcomes following endovascular treatment for BAO.
Results A total of 17 articles (6 prospective and 11 retrospective) were included. The weighted mean age of patients was 67 years (range 59–82) and 59% were male. Thrombolytic drugs were administered intravenously and intra-arterially in 46% (range 0–88%) and 38% (range 0–90%) of patients, respectively. Weighted pooled estimates of successful recanalization (TICI 2b–3) and good outcome (modified Rankin Scale ≤2) were 80.0% (95% CI 70.7% to 88.0%; I2=80.28%; p<0.001) and 42.8% (95% CI 34.0% to 51.8%; I2=61.83%; p=0.002), respectively. Pooled mortality was 29.4% (95% CI 23.9% to 35.3%; I2=37.01%; p=0.087). Incidence of procedure-related complications and symptomatic hemorrhage was 10.0% (95% CI 3.7% to 18.3%; I2=61.05%; p=0.017) and 6.8% (95% CI 3.5% to 10.8%; I2=37.99%; p=0.08), respectively.
Conclusions Stent retriever thrombectomy achieves a high rate of recanalization and functional independence while being relatively safe for patients with BAO. Future prospective studies with long-term follow-up are warranted.
- Thrombectomy
- Thrombolysis
- Device
- Stent
- Stroke
Statistics from Altmetric.com
Introduction
Acute basilar artery occlusions (BAOs) may result in ischemia or infarction in one or all of the brainstem, cerebellum, thalami, or occipital cortex and may present with symptoms including decreased consciousness, hemi or tetraplegia, ataxia, cranial nerve deficits, occulomotor abnormalities, or sudden death. BAOs are well known to be associated with high morbidity and mortality rates;1–3 the outcome for conservatively managed patients with angiographically proven BAO is poor in about 80% of cases.1 ,3
Early recanalization is associated with improved outcomes in these patients.4 Broadly, this can be achieved using IV or IA thrombolytic agents, thromboaspiration, and/or thrombectomy. Intravenous thrombolysis with recombinant tissue plasminogen activator (IV rtPA) is the most widely available therapy but this may achieve early recanalization in only a minority of BAOs.5 This has fueled interest in the use of endovascular techniques in this patient group.
Initial trials based on IA thrombolysis or older devices obtained equivocal results.6 ,7 More recently, multicenter randomized controlled trials have demonstrated technical and clinical efficacy for stent retriever thrombectomy either alone or in addition to IV rtPA versus best medical management for patients with large vessel occlusions in the anterior circulation.8–10 However, the safety, technical success, and clinical efficacy of stent retriever thrombectomy has not yet been proved for patients with BAO. This systematic review and meta-analysis aims to identify and analyze the available evidence on the safety, clinical efficacy, and complications of stent retriever thrombectomy in patients with BAO.
Methods
Literature search strategy
Two independent reviewers systematically searched Ovid Medline, PubMed, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, American College of Physicians Journal Club, and Database of Abstracts of Review of Effectiveness from inception to January 2015. To maximize the sensitivity of the search strategy, the following words were used as either key words or MeSH terms: ‘acute basilar artery’, ‘stroke’, ‘stent retriever’, ‘solitaire’, ‘revive’, ‘trevo’, and ‘mechanical thrombectomy.’ Reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies.
Selection criteria
Eligible studies were those that reported outcomes after stent retriever thrombectomy for BAO. Baseline demographics of the studies were extracted, as well as outcomes and complications of surgery, such as time to recanalization, rate of recanalization (Thrombolysis in Cerebral Infarction (TICI) score ≥2b), favorable clinical outcome (with a modified Rankin Scale (mRS) score ≤2 at 3 months), mortality (discharge and 3-month follow-up), and symptomatic intracerebral hemorrhage. When institutions published duplicate studies with accumulating numbers of patients or increasing lengths of follow-up, only the most complete reports were included. All publications were limited to those involving human subjects and in the English language. Abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded.
Data extraction and critical appraisal
Two investigators (KP and SP) independently reviewed each retrieved article. Discrepancies between the two reviewers were resolved by discussion and consensus. Because quality scoring is controversial in meta-analyses of observational studies, two reviewers (KP and SP) independently appraised each article according to the Dutch Cochrane Centre checklist proposed by the Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. The key points of this checklist include: (i) clear definition of the study population; (ii) clear definition of outcomes and outcome assessment; (iii) independent assessment of outcome parameters; (iv) sufficient duration of follow-up; (v) no selective loss during follow-up; and (vi) important confounders and prognostic factors identified.
Statistical analysis
A meta-analysis of proportions was conducted for the available main perioperative and postoperative variables. First, to establish variance of raw proportions, a Freeman–Tukey transformation was applied. To incorporate heterogeneity (expected among the included studies), transformed proportions were combined using the DerSimonian–Laird random-effects model. Finally, the pooled estimates were back-transformed. Heterogeneity was evaluated using Cochran Q and I2 test. Weighted means were calculated as the total number of events divided by the total sample size. Subgroup analyses were additionally conducted to determine potential sources of heterogeneity. All analyses were performed using the metafor package for R V.3.01. A p value <0.05 was considered statistically significant.
Results
After removal of duplicates, a total of 498 articles were identified from the six electronic databases (figure 1). After evaluating the abstracts of these articles, 51 remained eligible for assessment. The full texts of these articles were assessed by both reviewers, and 17 articles fulfilled the inclusion criteria.1–4 ,11–23 Six studies were prospective single-center studies, 10 were retrospective single-center studies, and one was a retrospective multicenter study. Study characteristics’ are summarized in table 1.
Study characteristics

PRISMA (Preferred reporting items for systematic review and meta-analysis) flow chart of search strategy of the present systematic review.
Baseline characteristics
Table 2 summarizes the baseline characteristics of the 17 relevant studies. Overall, the weighted mean age of all patients was 67 (range 59–82) years and 59% were male. A majority had hypertension (67%; range 48–78%). The pooled, weighted prevalence of dyslipidemia was 44% (range 24–61%), prior atrial fibrillation was 33% (range 19–45%), diabetes mellitus type 2 was 26% (range 14–44%), hypercholesterolemia was 26% (range 24–57%), and coronary heart disease was 16% (range 7–22%). The proportion of smokers was 21% (range 17–36%).
Baseline characteristics
The prevalence of patients with a history of stroke was 34% (range 21–58%), of which 28% (range 10–36%) were due to large artery disease and 41% (range 14–61%) due to cardioembolism. Three-quarters of patients were initially screened with CT (75%; range 0–100%) and a quarter with MRI (25%; range 0–100%) (table 3).
Basilar artery occlusion location, patient management and treatment
BAO and treatment
The BAO was located in the proximal, mid, and distal portion of the basilar artery in 33% (range 22–50%), 34% (range 0–41%) and 32% (range 26–60%) of patients, respectively. The mean presenting National Institute of Health Stroke Scale (NIHSS) was 17.8 (table 3).
Stent retriever thrombectomy was performed in 77% (range 14–100%) of patients, while thrombectomy with non-stent retrievers (Merci device, Penumbra aspiration catheter) or sole use of IA thrombolytic agents was used in 21% (range 0–86%). The mean number of passes of the thrombectomy device was 2 (range 1.3–2.8). Thrombolytic drugs were administered intravenously in 46% (range 0–88%) of patients, and intra-arterially in 38% (range 0–90%). Anti-platelet and anticoagulant drugs were given to 24% (range 14–52%) and 14% (range 4–50%) of patients, respectively (table 3).
The mean time to recanalization was 7.6 h, with a procedural time of 216 min (table 3).
Operation parameters
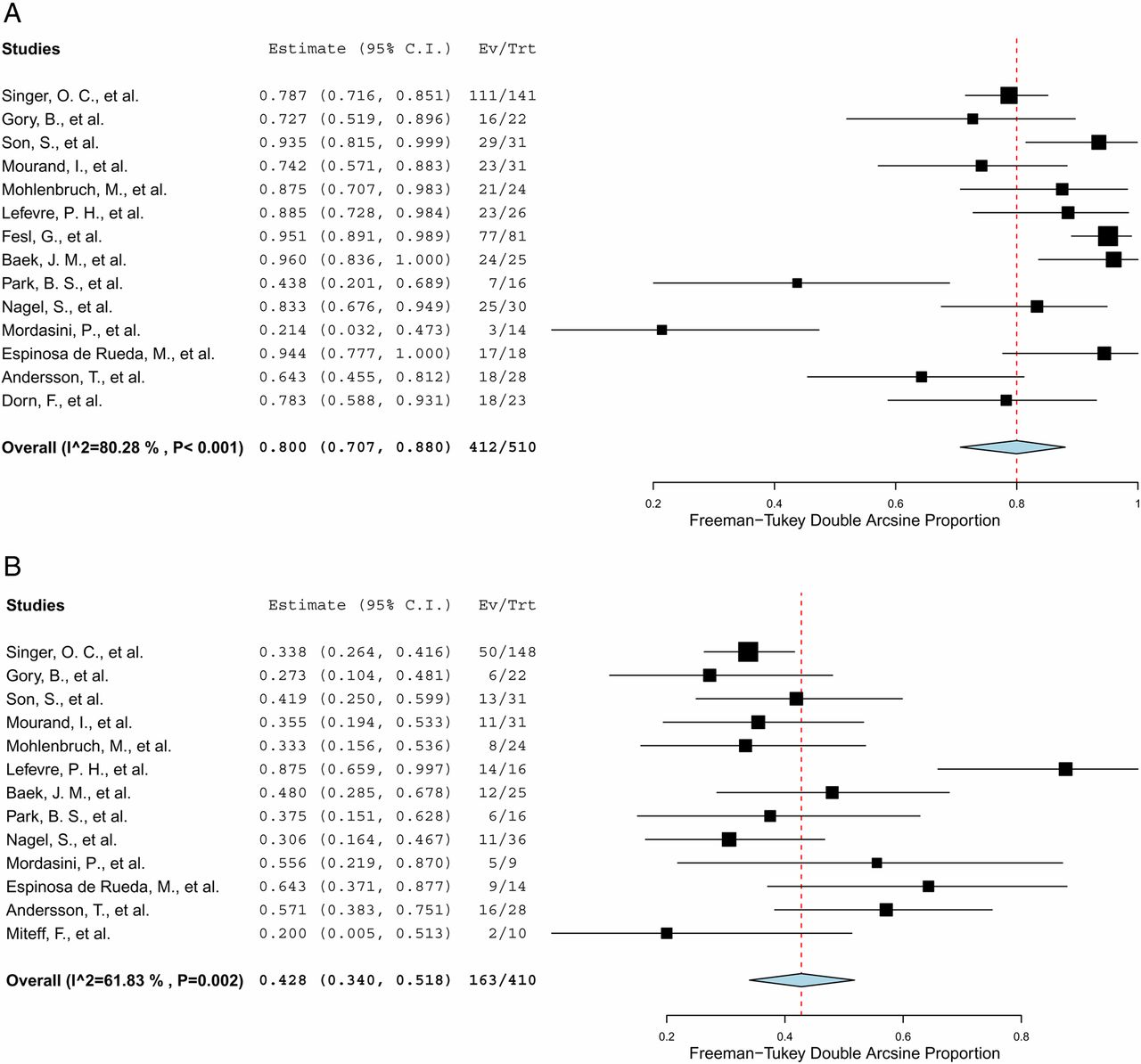
Weighted pooled estimates of successful recanalization (TICI 2b–3) and good outcome (mRS≤2) were 80.0% (95% CI 70.7% to 88.0%; I2=80.28%; p<0.001) and 42.8% (95% CI 34.0% to 51.8%; I2=61.83%; p=0.002), respectively (figure 2A, B).

Forest plots for (A) successful recanalization (TICI 2b–3) and (B) good outcome (mRS≤2). mRS, modified Rankin Scale; TICI, Thrombolysis in Cerebral Infarction.
Mortality and morbidity
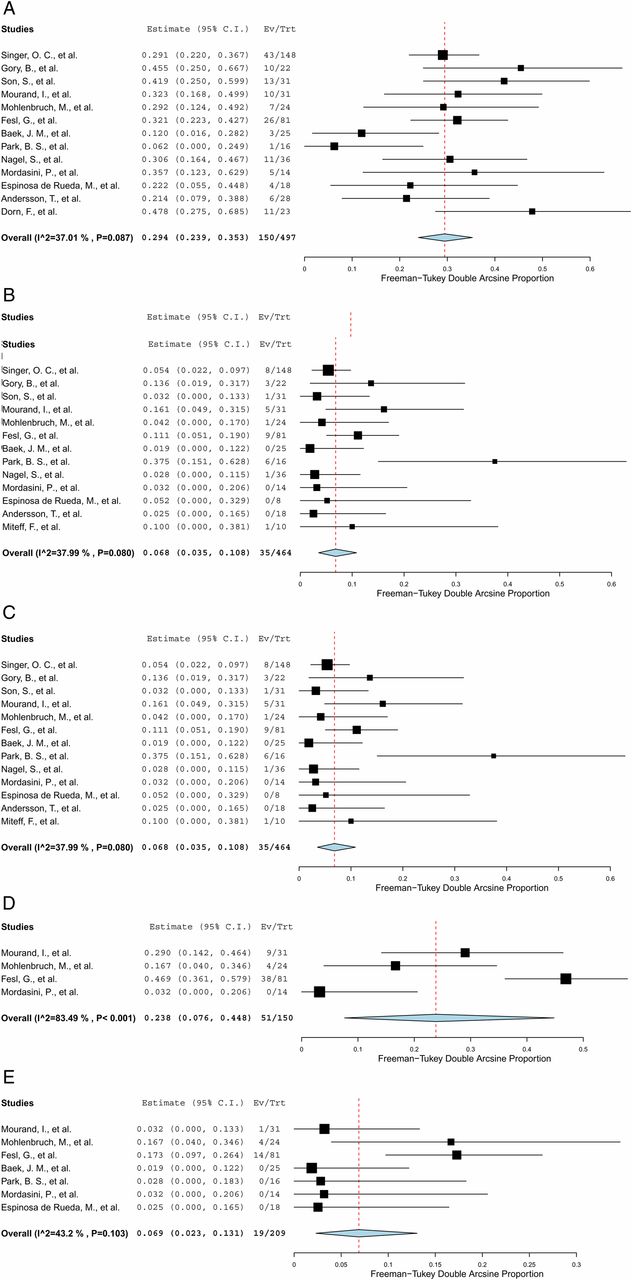
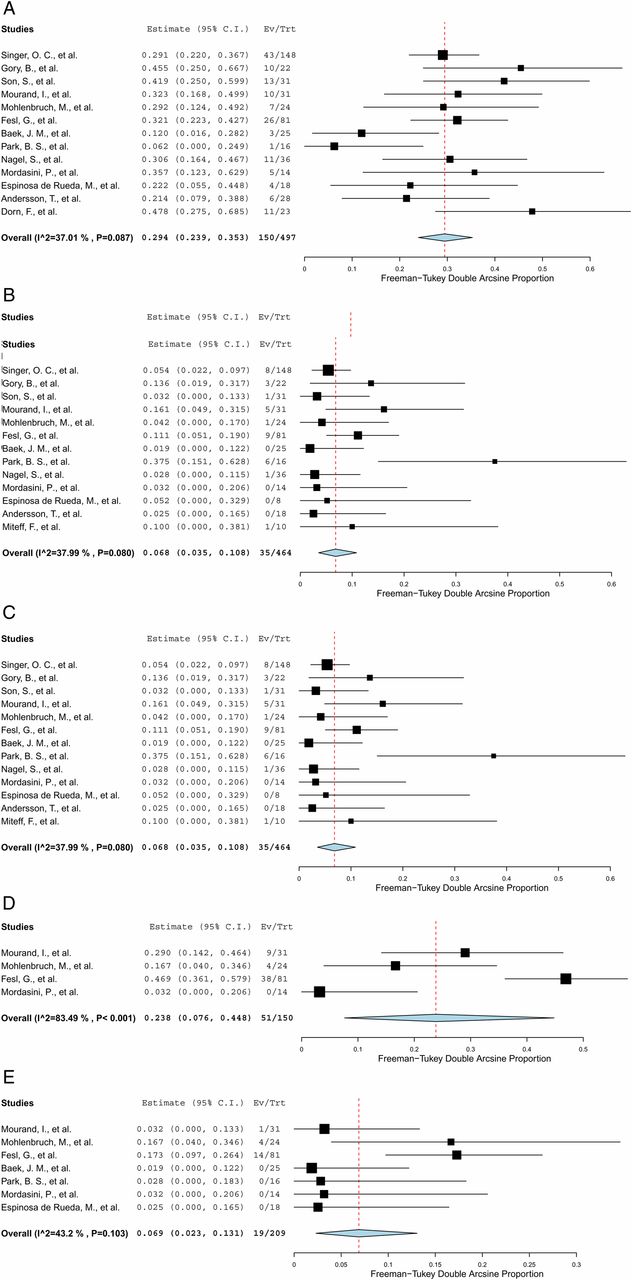
From 13 studies, pooled mortality was 29.4% (95% CI 23.9% to 35.3%; I2=37.01%; p=0.087) (figure 3A). The weighted, pooled estimate of procedure-related complications was 10.0% (95% CI 3.7% to 18.3%; I2=61.05%; p=0.017), with symptomatic intracranial hemorrhage (SICH) and dissection occurring in 6.8% (95% CI 3.5% to 10.8%; I2=37.99%; p=0.080) and 6.9% (95% CI 2.3% to 13.1%; I2=43.2%; p=0.103) of the cohort, respectively (figure 3B, E). Embolic infarcts occurred in 23.8% of patients (95% CI 7.6% to 44.8%; I2=83.49%; p<0.001) (figure 3D).
{kind=link}
{kind=link}
{kind=link}
Forest plot for (A) mortality; (B) procedure-related morbidity; (C) symptomatic hemorrhage; (D) embolic infarct; (E) dissection.
Endovascular retriever: stent versus non-stent
Two studies compared stent and non-stent retriever thrombectomies. In the study of Singer et al,22 stent retrievers included Solitaire, Trevo, Acandis Aperio, Mindframe, Preset, Revive, and Bonnet, and non-stent retrievers included Merci, Penumbra, Phenox clot retriever, and Catch device. The study of Son et al compared Solitaire with the Penumbra suction device. Pooled analysis showed no significant difference in a good outcome (mRS 0–2) between these two treatments (34.4% vs 40.0%; RR=0.91; 95% CI 0.55 to 1.49; p=0.71). Son et al23 showed that patients treated by Penumbra suction thrombectomy had significantly higher complete recanalization rates (TICI score of 3: 23.1% vs 72.2%, p=0.015) and shorter total procedure times (101.9±41.4 vs 62.3±34.8 min, p=0.044). However, successful recanalization rates TICI score ≥2b: 84.6% vs 100%, p=0.168) and clinical outcomes (judged by the mRS scores recorded at 3 months: 3.6±2.6 vs 3.2±2.6, p=0.726) were not significantly different between the types of endovascular retriever.
BAO with and without endovascular thrombectomy devices (stent retrievers)
Nagel et al19 compared outcomes before and after the introduction of endovascular thrombectomy devices (stent retrievers: Revive and Solitaire) for BAO.
Complete recanalization (TICI 3) was higher after the introduction of stent retrievers (66.7% vs 45.1%, p=0.062). Similarly, higher rates of a favorable clinical outcome were seen in the stent retriever group (30.6% vs 13.5%; p=0.026). Mortality was lower in the later treated group (36.1% vs 57.7%; p=0.034). The frequency of SICH was lower in the later treated group (2.8% vs 8.1%, p=0.45). Treatment after the introduction of stent retrievers was an independent predictor of good clinical outcome (OR=2.56; 95% CI 1.01 to 6.78) and mortality (OR=0.36; 95% CI 0.15 to 0.86) in an adjusted logistic regression model.
Discussion
This systematic review and meta-analysis demonstrates high rates of successful recanalization for acute BAO treated in most cases with stent retriever thrombectomy. The overall recanalization rate was 80.0%. Although not as high as recanalization rates, stent retriever thrombectomy resulted in acceptable favorable outcome rates of 42.8%. Pooled mortality was 29.4% and procedure-related complications were 10.0%, with SICH and dissection occurring in 6.8% and 6.9% of the cohort, respectively.
Factors affecting functional outcome
Several factors may account for the disconnection between high rates of recanalization and the relatively lower rates of favorable outcome, such as time to treatment, baseline core infarct, and rate of embolic infarction.
The lengthy time from stroke onset to recanalization is likely to have negatively affected functional outcome. The pooled time from stroke onset to recanalization from 10 studies was 7.6 h, including a mean procedural time of 216 min (range 77–441 ). The Basilar Artery International Cooperation Study (BASICS) prospective registry demonstrated that the chance of a poor outcome was significant increased when recanalization therapy was started after 6 h.5 Interestingly, five studies in this review that assessed the association between time to recanalization and favorable outcome, did not find a significant correlation.4 ,13 ,16 ,17 ,20 The lack of association may be because most patients were being treated at a late time point (>5 h), resulting in a limited association between time and outcome, and thus with outcome governed by more dominant factors such as collateral flow and baseline ischemia. Future studies to assess functional outcome in which patients with BAO are recanalized within a shorter time after symptom onset are warranted.
The extent of baseline ischemia is also likely to influence functional outcome; recanalization of BAO up to 48 h after onset was found to be beneficial in the absence of extensive baseline ischemia in one study.24 The degree of baseline ischemia is dependent on the status of collateral flow, volume of core infarct, and volume of penumbra. A number of studies using diffusion-weighted imaging (DWI) or CT angiographic source images have demonstrated an association between baseline imaging evidence of ischemia and eventual outcome despite high rates of effective recanalization.25 However, few studies in this review described the degree of baseline ischemia. Moreover, the baseline imaging for patients varied between studies; with 25% of patients undergoing MRI, and 75% undergoing CT at primary admission. Future studies controlling for the degree of baseline ischemia is essential to determine which patients with BAO benefit the most from stent retriever thrombectomy.
Distal embolic infarction occurring during endovascular thrombectomy is another factor which may influence favorable outcome rate. The pooled rate of embolic infarction (23.8%) in this review was higher than that recorded for anterior circulation strokes in the North American Solitaire Acute Stroke Registry (16.2%).26 The higher rates for BAO are probably due to the competing flow from the contralateral vertebral artery. Potential methods of reducing the risk of fragmentation and distal embolic infraction include combining the use of stent retrievers with distal aspiration catheters with positioning of the distal aspiration catheter beyond the vertebrobasilar junction. Both IV and IA rtPA may have a role in treating distal embolization. In this analysis, thrombolytic drugs were administered intravenously to 46% and intra-arterially to 38% of patients. However, it was not possible to ascertain whether the addition of thrombolytic agents affected outcome.
Stent retriever thrombectomy versus conservative management (antiplatelet/anticoagulant)
Recent data on outcomes in conservatively managed patients with BAO can be drawn from the BASICS prospective registry,5 which recorded outcomes in a cohort of 183 patients between 2002 and 2007 with a mean NIHSS score of 15, treated with antiplatelets or anticoagulant agents only. Favorable outcomes (mRS≤2) were seen in 27% of patients presenting with mild–moderate stroke and 4% of patients presenting with severe stroke (coma, locked-in, or tetraplegia). This equated to an overall favorable outcome rate of 17%. The overall mortality was 31% but for severe stroke was 54%. Although making a direct comparison with these studies has limitations, the results of this review suggest that favorable outcome rates are approximately doubled with modern endovascular techniques.
Stent retriever thrombectomy versus intravenous thrombolytic agents
The pooled frequency of recanalization after stent retrievers (80%) exceeds that of previously published recanalization rates after IV rtPA; Bhatia et al27 demonstrated extremely low rates of recanalization with IV rtPA for BAO that were of the order of 8%.
Recanalization rates with IV rtPA were quoted as 67% in the BASICS registry5 but follow-up CT angiography, MR angiography or transcranial Doppler ultrasound was performed hours to days after treatment in a minority of patients. A favorable outcome (mRS≤2) was seen in 44% of a population with mean presenting NIHSS score of 21. However, the mortality rate was 42%. A systematic literature review of patients with BAO treated with intravenous tPA28 (76 patients, 51% in coma) demonstrated favorable outcome in 22% with mortality of 50%, and the SICH rate was 11%. Again, though there are limitations in making direct comparisons with these studies, the results would suggest a 10–20% reduction in mortality but rates of favorable outcome are not overtly better than the BASICS data, which is surprising bearing in mind low rates of early BAO recanalization with IV rtPA.27
High rates of SICH do not seem to be responsible for this. Similar rates of SICH were seen in this analysis and the IV rtPA arm of the BASICS study and much lower rates than published in Lindsberg and Mattle's systematic review.28 Other procedural complications, such as vessel dissection (seen in 6.9%, although highly variable), might affect outcome, though the influence is debatable as many iatrogenic dissections have a benign course.
Stent retriever thrombectomy versus intra-arterial thrombolytic agents
Most published reports pertaining to endovascular treatment of BAO centers on the use of IA thrombolytic agents. In the largest series to date, the data of 180 adult patients with angiographically confirmed BAO treated with IA thrombolysis at five German stroke centers were retrospectively evaluated.29 Complete recanalization was achieved in 55% and partial recanalization in 19%. However, favorable outcomes (mRS≤2) were seen in only 23% and the mortality was 43%. Furthermore, the BASICS registry found that patients treated with IA thrombolytic agents fared poorly, since in a cohort with a presenting NIHSS score of 25, the favorable outcome was 17.4% (mRS≤2); the mortality rate was 41% and the SICH rate was 14%. Therefore, there is no obvious benefit for the use of IA thrombolytic agents as a sole treatment and the results of this analysis suggest that the use of stent retrievers achieves better rates of recanalization and clinical outcome with lower rates of SICH.
Endovascular retriever: stent versus non-stent
Recent advances in endovascular devices have improved the rate of recanalization and clinical outcomes. Compared with the last generation of mechanical devices, stent retrievers have been found to improve the rate of recanalization and favorable clinical outcomes in large vessel occlusion strokes of the anterior circulation.10 In the SWIFT trial, recanalization was achieved more often in the Solitaire group (stent retriever) than it was in the Merci group (non-stent retriever) (61% vs 24%, p=0.0001) and more patients had a good 90-day neurological outcome with Solitaire than with Merci (58% vs 33%, p=0.02).30
The high rates of recanalization seen in this study suggest that similar results can be achieved when treating BAO. However, only two studies have compared stent and non-stent retriever thrombectomies in BAO.22 ,23 Pooled analysis showed no significant difference in good outcome (mRS 0–2) according to the type of retriever device. Interestingly, Son et al demonstrated that Penumbra suction thrombectomy (non-stent retriever) seemed to allow a more rapid and complete recanalization than Solitaire stent retriever thrombectomy.23
Limitations
This review has several limitations. First, both prospective and retrospective studies were included with relatively few patients. Most papers looked specifically at BAO, although some examined posterior circulation strokes3 and others assessed both anterior and posterior circulation occlusions.14 ,21 Although the stent retrievers showed a good recanalization rate, no randomized clinical trials have assessed their clinical efficacy in comparison with the reference treatment for BAO. Second, definitions and protocols varied between studies. For example, Baek et al1 included patients with a baseline NIHSS score ≥4, no bilateral diffuse pontine ischemia on DWI, and start of the procedure within 8 h after symptom onset, whereas Mourand et al18 included patients without NIHSS restriction or limit on DWI ischemic lesion load, and the recanalization could be achieved within 24 h of ictus. These limitations should be considered when interpreting the results of our systematic review.
Conclusion
Mechanical thrombectomy, mainly with stent retriever, for patients with an acute, symptomatic BAO can achieve high rates of recanalization, with relatively low rates of SICH. Future randomized controlled trials to assess its clinical efficacy in comparison with the reference treatment are warranted.
References
Footnotes
Contributors KP: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, acquisition of data, statistical analysis, study supervision. SP, YRH, FJ: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, acquisition of data. AM: drafting/revising the manuscript, study concept or design, analysis or interpretation of data, contribution of vital reagents/tools/patients, study supervision, obtaining funding.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available in the manuscript.