Article Text

Abstract
Background The use of retrievable stents for endovascular clot retrieval has dramatically improved successful revascularization and clinical outcome in selected patients with acute stroke.
Objective To describe the rate and clinical consequences of unwanted spontaneous detachment of these devices during mechanical thrombectomy.
Methods We studied 262 consecutive patients treated with the retrievable stent, Solitaire, for acute ischemic stroke between November 2008 and April 2015. Clinical, procedural, and outcome variables were compared between patients with and without unexpected detachment of this device. Detachment was classified as proximal to the stent proximal marker (type A) or distal to the marker (type B). Poor functional outcome was defined as modified Rankin scale score >2 at 90 days.
Results Unwanted detachment occurred in 6/262 (2.3%) cases, four of type A and two of type B. Stent recovery was possible in three patients, all of ‘type A’, but in none of ‘type B’. The number of prior passes was higher in patients with undesired detachment (3 (2–5) vs 2 (1–3), p=0.007). Detachment was associated with higher rate of symptomatic intracranial hemorrhage (SICH) (33.3% vs 4.3%, p=0.001), poorer outcome (100% vs 54.8%, p=0.028), and higher mortality rate at 90 days (50% vs 17%, p=0.038).
Conclusions Unwanted detachment of a Solitaire is an uncommon complication during mechanical thrombectomy in patients with acute ischemic stroke and is associated with the clot retrieval attempts, SICH, poor outcome, and higher mortality.
- Thrombectomy
- Technique
- Stroke
Statistics from Altmetric.com
Introduction
The Solitaire (Medtronic/Covidien/ev3, Dublin, Ireland) is a nitinol self-expanding stent with a honeycomb pattern in an overlap platform, which uniquely can be fully deployed and then completely retrieved if it has not been detached.
Initially, this device was designed to treat aneurysms, with the detachable option by electrolysis.1 In 2008, we successfully used Solitaire to retrieve an intra-arterial thrombus that had resisted several attempts with the MERCI system in a patient with acute ischemic stroke (AIS).2 Subsequent studies confirmed the efficacy of this device for restoring vascular patency at a significantly higher rate than previous generation devices and techniques.3–5 Recently, several clinical trials have demonstrated that thrombectomy with a retrievable stent in patients with AIS with large artery occlusion safely increases the rate of functional independence.6–10
It is in this new situation, when these stents no longer need to be released, that they need to be strongly attached to the push wire in order to be retrieved. An accidental detachment may halt the removal of the clot and threaten the safety of the patient. In this observational study of a large population from a single center, we aimed to describe the rate, associated factors, and clinical consequences of unwanted spontaneous detachment of these devices during mechanical thrombectomy.
Material and methods
We studied consecutive patients treated with mechanical thrombectomy with retrievable stents in a comprehensive stroke center connected to a stroke network and covering a population of 1.5 million people.
Criteria for primary or rescue endovascular treatment were predefined and approved by the local ethics committee.11 Briefly, all patients with AIS with no contraindication for IV thrombolysis, who arrived within the first 4.5 h, received the standard dose of recombinant tissue-type plasminogen activator (0.9 mg/kg). Patients refractory to, or ineligible for, IV thrombolysis (including stroke onset beyond 4.5 h, unknown onset, or wake-up stroke) were preselected for endovascular stroke therapy according to clinical criteria (National Institutes of Health Stroke Scale (NIHSS) score ≥6 or suspicion of large-vessel occlusion) at the local centers. Subsequently, at our comprehensive stroke center, an indication for endovascular stroke therapy was based on demonstration of a large-vessel occlusion by non-invasive vascular imaging and presence of signs of limited early infarction before transferring the patient to the angiosuite. Multimodal imaging (MRI or CT perfusion) was recommended in patients beyond 4.5 h from stroke onset. Informed consent from the patients or their relatives was obtained before the endovascular procedure. Between November 2012 and December 2014 patients were treated in the REVASCAT clinical trial.10
After the procedure, patients were admitted to an acute stroke unit and managed according to the European Stroke Organization Guidelines.12 A CT scan was performed routinely at 24–36 h after treatment, or earlier if any neurological worsening ≥4 points in NIHSS score occurred.
Revascularization procedure
Depending on the patient’s condition, procedures were performed under sedation or general anesthesia. Technical details of the procedure have been described elsewhere.3 Briefly, the balloon guide catheter was inserted transfemorally and placed in the proximal internal carotid artery for the carotid territory, and the subclavian artery for the vertebrobasilar territory. A heparin bolus was not administered and no heparinized saline solution was continuously perfused through the catheter during the procedure. With the balloon of the guide catheter deflated, a 0.014 inch guidewire was advanced through the clot (with the tip bent) within the occluded intracranial vessel. The Rebar 18 microcatheter (ev3 Inc, Irvine, California, USA) was then advanced over this wire through the clot, and the guidewire was exchanged for the embolectomy device (Solitaire). Then, the Solitaire was advanced and deployed over the clot with the distal portion of the stent placed a few millimeters after the clot, opening the vessel and allowing blood flow in the lenticulostriate and distal branches if the clot length was shorter than the stent (in almost all cases we used Solitaire 4×20 mm). To prevent arterial rupture, the distal part of the device was deployed in a straight portion of the artery.
The stent was kept deployed for 3 min before retrieving in order to better entrap the clot. The balloon of the guide catheter was then inflated and the microcatheter and the embolectomy device were gently withdrawn into the body of the guide catheter while aspiration with a 60 cc syringe was carried out. The clot was retrieved and the balloon was then deflated. Control angiography was then performed to confirm recanalization and reperfusion.
If the patient had a tandem occlusion, we performed a small angioplasty (with a balloon 2×20 mm) to allow passage of the balloon guide catheter before distal mechanical thrombectomy. After intracranial recanalization, with the technique described above, we carried out angioplasty (with a balloon 5×20 mm) trying to avoid placing a stent to prevent early antiplatelet therapy and hemorrhagic transformation, in accordance with our previous study.13
Unwanted spontaneous detachment of the stent during clot retrieval was classified as proximal to the stent proximal marker (type A) or distal to the marker (type B) (figure 1). In these cases we attempted to capture the device with an Amplatz GooseNeck snare (Medtronic/Covidien/ev3, Dublin, Ireland). Once the stent was gripped by the loop, we proceeded to extract it, using the same technique as described earlier to remove the thrombus (figures 2 and 3).
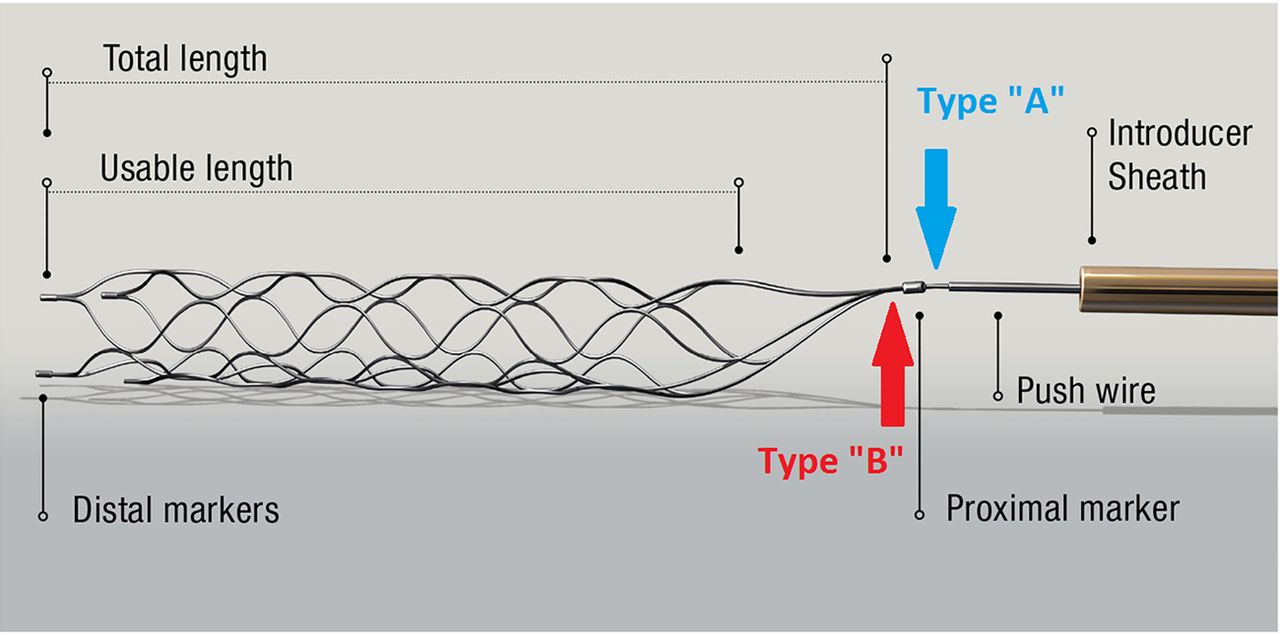
Two sites at which detachment of Solitaire devices occurs, classified as type ‘A’ (proximal to the proximal mark) and type ‘B’ (distal to the proximal mark).
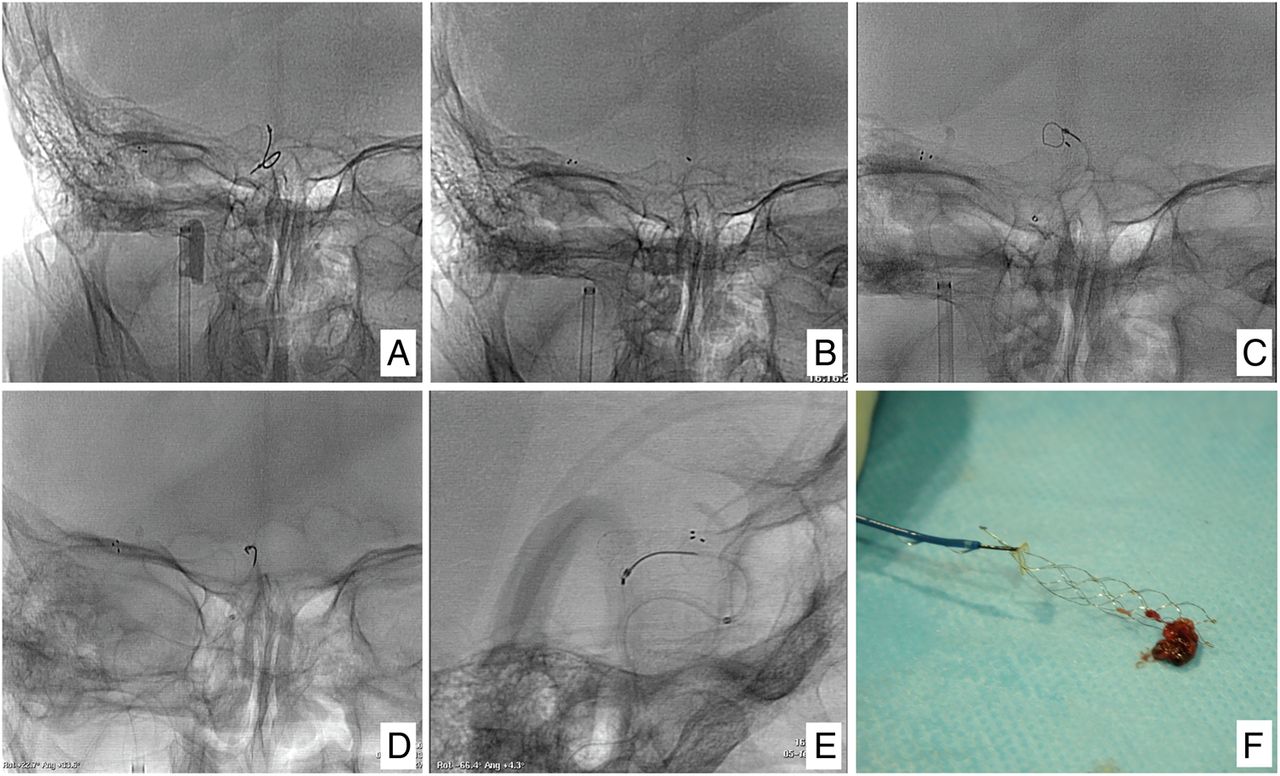
Example of a detachment type ‘A’. The sequence of detachment, capture, and removal of a Solitaire device with an Amplatz GooseNeck snare is shown. (A) The stent was kept deployed for 3 min before retrieving in order to better entrap the clot. The balloon of the guide catheter was then inflated and the microcatheter and the embolectomy device were gently withdrawn under continuous aspiration. (B) Solitaire unwanted detachment of the push wire occurs. We can see how the stent is left in the middle cerebral artery and does not appreciate the push wire, but we can visualize the proximal marker of the stent (type A). (C) We attempted to capture the Solitaire with an Amplatz GooseNeck snare (Medtronic/Covidien/ev3, Dublin, Ireland). (D and E) Once we had gripped the Solitaire by the loop, we extracted the stent, by the same technique as described earlier to remove the thrombus. (F) The Solitaire gripped by the Amplatz GooseNeck snare with thrombus was captured by the stent.

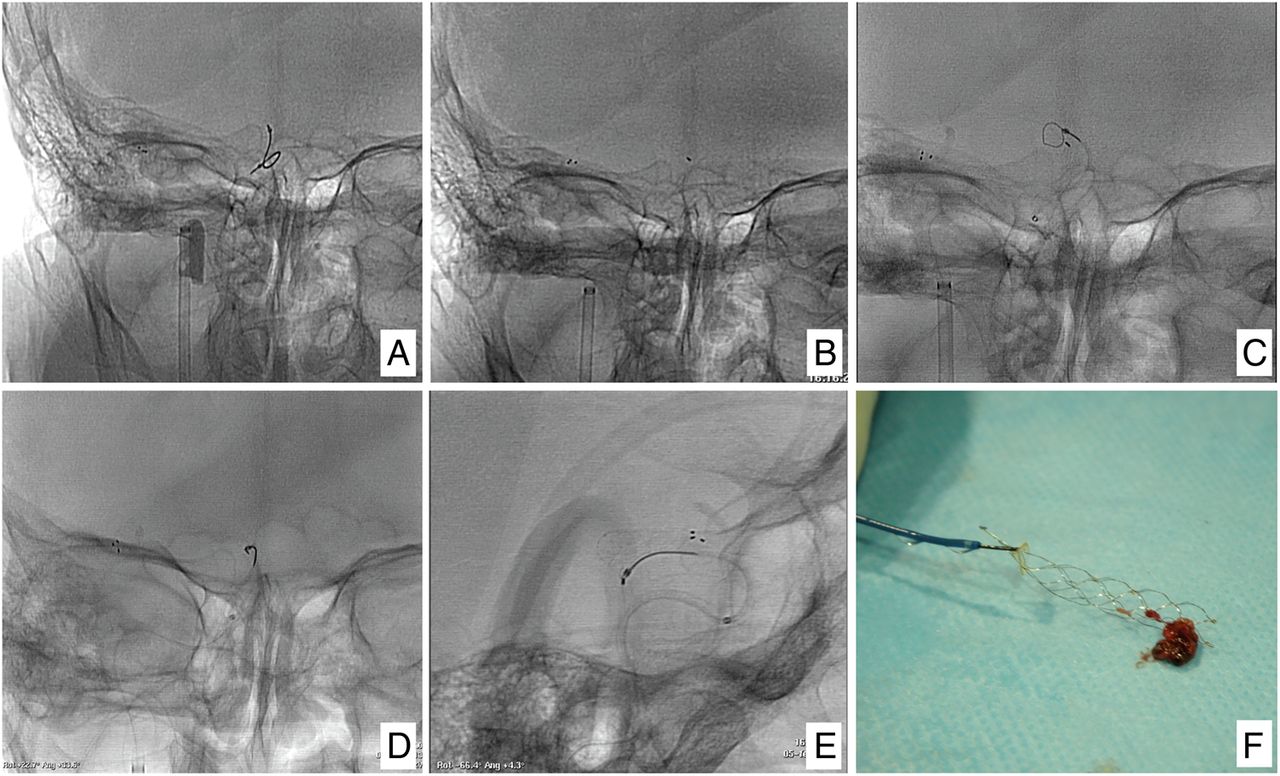
Example of a detachment type ‘B’. The sequence of the detachment, and failed attempt to capture the Solitaire with an Amplatz GooseNeck snare is shown. (A) The stent was kept deployed for 3 min before retrieving in order to better entrap the clot. The balloon of the guide catheter was then inflated and the microcatheter and the embolectomy device were gently withdrawn under continuous aspiration. (B and C) Solitaire unwanted detachment of the push wire occurs. We can see how the stent is left in the middle cerebral artery and does not appreciate the push wire, but we cannot visualize the proximal marker of the stent (type B). (D) We attempted to capture the stent with an Amplatz GooseNeck snare many times, but this was not possible. (E) The proximal Solitaire marker attached to the push wire. It can be seen that the stent was removed just distal to the proximal brand of the stent.
Outcome variables
Neurologic worsening was defined as an increase of at least four points in the NIHSS score evaluated at 24–36 h after thrombectomy. Symptomatic intracranial hemorrhage (SICH) was defined as any parenchymal hemorrhage associated with neurologic worsening of at least four points in the NIHSS score. Poor functional outcome was considered present when the modified Rankin Scale score was ≥3 at 90 days. Causes of mortality and device-related mortality were also recorded.
Results
Between November 2008 and April 2015 a total of 306 patients with AIS were treated with mechanical thrombectomy in our center. A Solitaire (AB or FR) device was used in 262 patients. In 243/306 (79.4%) patients thrombectomy was performed only with a Solitaire, while in 19 (7.2%) cases an additional device was used in combination with the Solitaire. Unwanted detachment occurred in 6/262 (2.3%) cases, four of type A and two of type B (two with the Solitaire AB and four with the FR). Clinical characteristics of these six patients are shown in table 1. Stent recovery using the snare device was possible in three patients, all of them type A. Table 1 shows baseline clinical characteristics and procedural variables in patients with an undetached and detached device. Patients with undesired detachment were older and received a higher number of passes with the same device (3 (2–5) vs 2 (1–3), p=0.007) than patients without detachment.
Baseline and procedure variables associated with Solitaire detachment
Detachment was associated with a lower frequency of complete recanalization, higher rate of SICH at 24 h, poorer outcome, and higher mortality rate at 90 days (table 3). Mortality was device detachment-related in a patient who developed a large infarction in the territory of a permanent occluded artery by the stent bringing the thrombus inside.
Discussion
The use of stent retrievers for the revascularization of occluded intracranial vessels in patients with acute stroke, has significantly improved the efficacy and safety of endovascular procedures in comparison with previous devices.5 Moreover, they have led to a revolution in the management of patients with stroke and a large artery occlusion, since they can reduce disability without increasing the rate of adverse events with respect to intravenous thrombolysis.3–10
Device- and procedure-related adverse events ranged from 2.6% to 10.9% in recently published endovascular thrombectomy clinical trials with stent retrievers; arterial dissection or perforation were reported, but spontaneous unwanted detachment of the Solitaire retrievable stent device was not mentioned in these reports.4 ,6–10
In this observational study of a large number of patients we report an undesired detachment rate of 2.3%. Both, type A and B detachments were found. This procedural complication was associated with a higher number of retrieval attempts and resulted in a significant increase in SICH and poor clinical outcome.
A previous report by Korean authors14 has found a similar rate of detachment—3.9%—nine patients among 232 Solitaire thrombectomies. Type ‘A’ was seen in three patients, and type ‘B’ in the remaining six patients. Four cases underwent three or more retrieval attempts, but in five cases the artery remained completely occluded after the procedure and only one patient achieved favorable functional outcome at 3 months. Unexpected detachment was associated with a relatively large-diameter stent (Solitaires 6×30 mm in seven cases), especially in elderly patients with middle cerebral artery occlusions. However, in our series all cases were treated with Solitaires 4×20 mm (table 2).
Clinical characteristics of the patients who unwanted detachment occurred
Procedural related complications and outcome variables when Solitaire detachment occurs during endovascular treatment
Recently, the Solitaire-FR-related adverse events reviewed by MAUDE (Manufacturer and User Facility Device Experience) were published on the US Food and Drug Administration website. In total, 85 adverse events related to the use of the Solitaire FR stent were reported between March 2012 and October 2014. Inadvertent detachment of the device was described in 80 patients; 13 of these 80 patients (16%) died after the procedure and 11/62 patients (18%) with available outcome data had a procedure-related injury. Detachment occurred, respectively, at the first, second, and third pass in 9 (21%), 21 (49%), and 13 (30%) of the 43 patients for whom this information was available. Resistance was perceived by the physician during retrieval of the device in 12 patients. A rescue maneuver was reported in 20 (25%) of the 80 cases, resulting in flow re-establishment in 13 (65%).15
Our results show that type ‘A’ detachment can be recovered, whereas type ‘B’ is almost impossible to recapture (figures 2 and 3). This might be because in type ‘A’ detachment, the proximal marker remains attached to the stent, and makes the ‘stent legs' converge and join the marker. This allows a radiopaque reference to direct the snare and slide it around the stent to capture the Solitaire. In the ‘B’ type, the break occurs at the junction of the stent with the proximal marker, allowing the ‘stent legs' to open or stay together making a ‘spearhead’ that digs into the wall of the artery. In this situation, there is no radiopaque reference to direct the snare, and as the ‘legs' are leaning against the wall, it becomes very difficult to slide the loop out of the stent to capture the Solitaire.
Spontaneous detachment of the stent may also occur owing to ‘fatigue’ of the material due to prolonged use, or additional stress from the technique used, damage during washing for re-use, or a manufacturing defect.
Another aspect to consider is the likelihood of a higher rate of detachment using a ‘Solumbra’ technique, in which the Solitaire is pulled into an intermediate aspiration catheter. In this case the forces applied to the binding of the stent may be greater.
A technical aspect which might help to prevent this complication is to coat the proximal marker of the stent with the microcatheter during removal of the stent, thus, possibly, reducing the stress of the material. On the screen you can visualize the following sequence: the microcatheter radiopaque marker, followed by a non-radiopaque proximal area of the stent, followed by the proximal marker of Solitaire, followed by a hypodense area (area of electrolytic detachment), followed by a radiopaque area produced by the push wire.
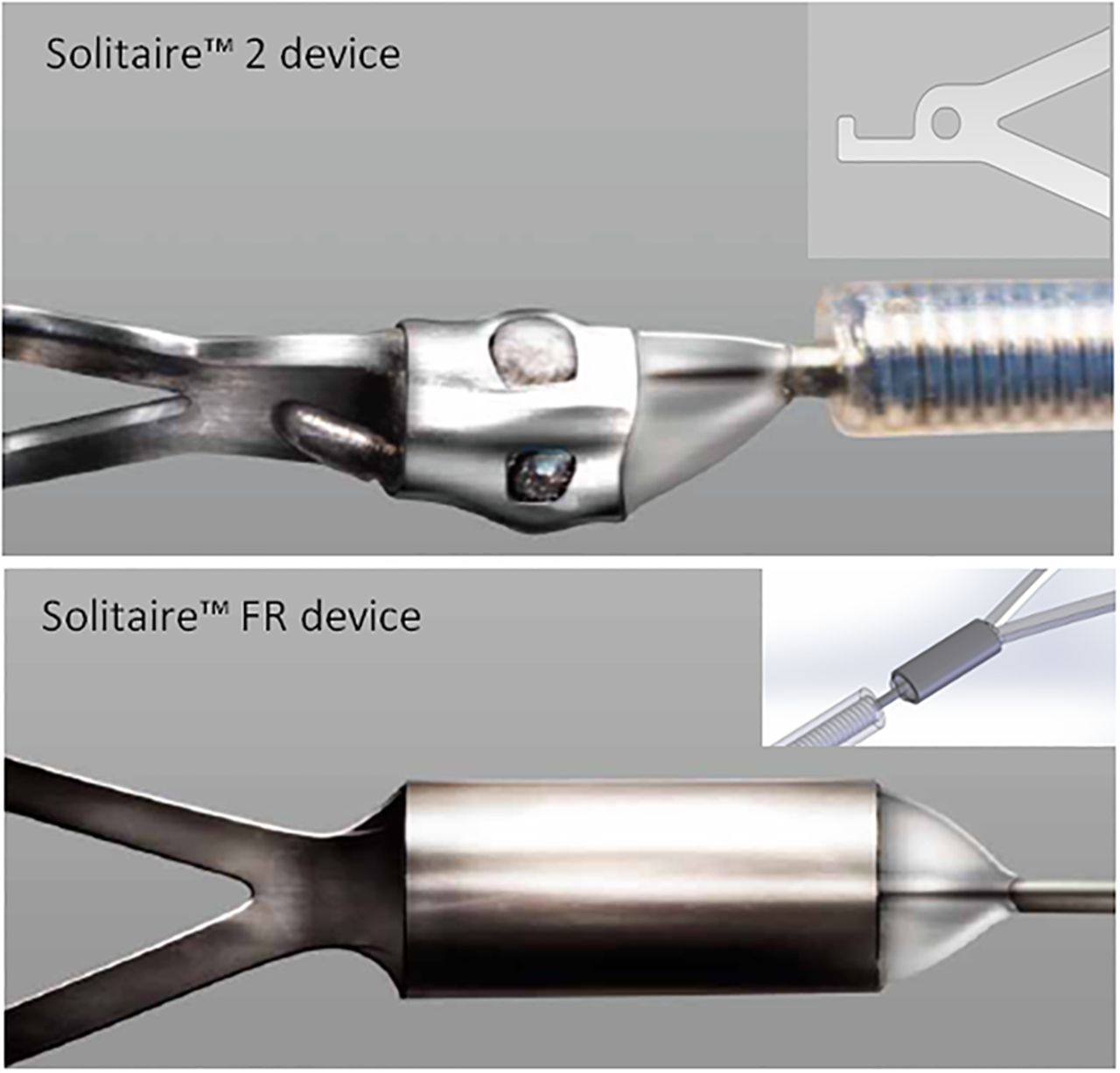
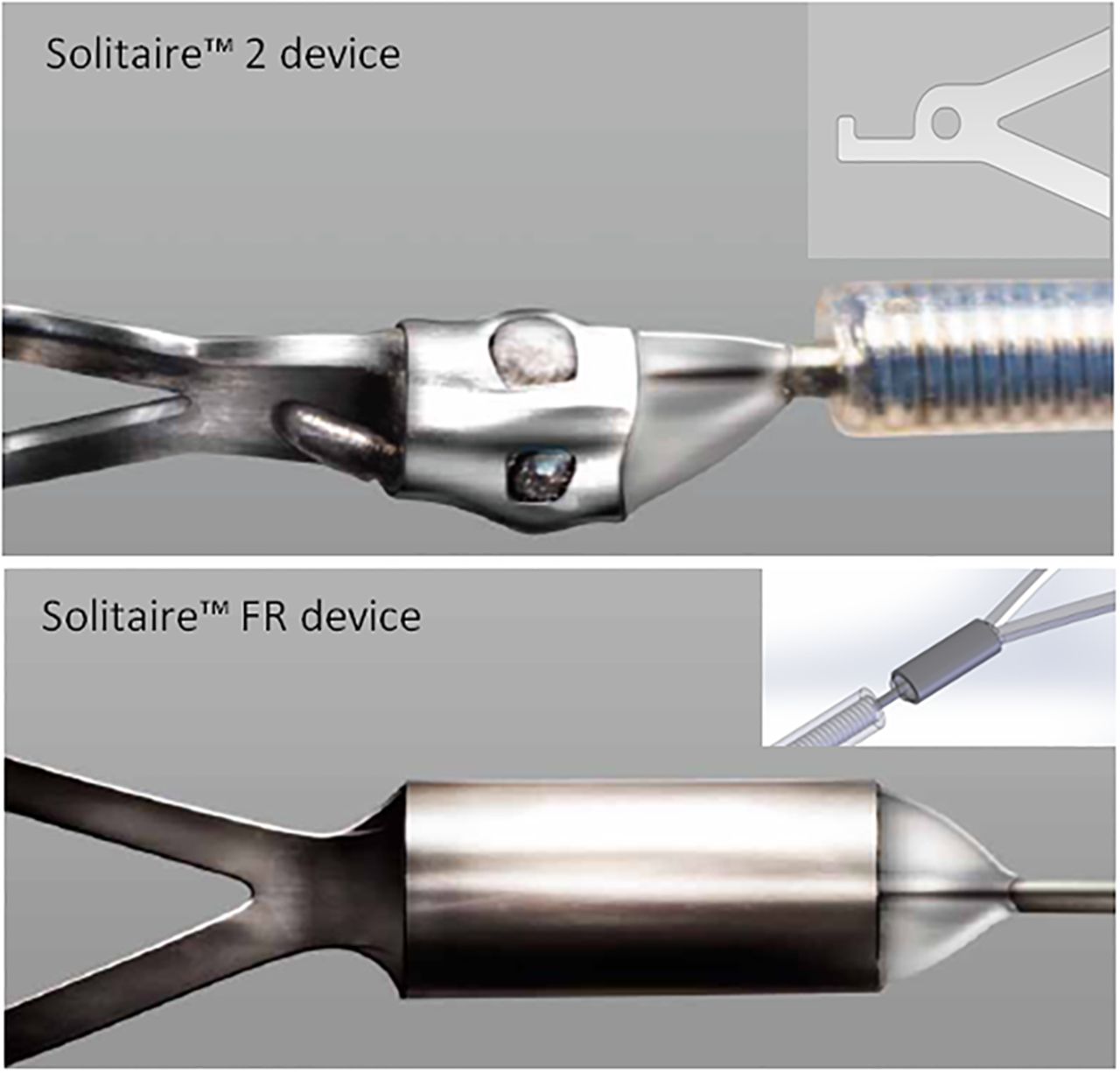
In an in vitro investigation16 the tensile force needed to separate the Solitaire stents from the pusher wire was about 6 N. In the recently marketed ‘Solitaire 2’, in which the manufacturer has made some changes to the binding site of the stent with the push wire (figure 4), the redesigned attachment zone has double the joint strength, increasing from 6 to 12 N the tensile force needed for separation.17 ,18
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes between the Solitaire FR (B) and the new Solitaire 2 (A) at the junction between the stent and the push wire are shown.
In conclusion, unwanted detachment of a Solitaire device is an uncommon complication during mechanical thrombectomy in patients with AIS and is associated with the number of clot retrieval attempts, SICH, poor outcome, and higher mortality. Changes that have been made to the new Solitaire 2, may reduce or eliminate this potential complication.
Acknowledgments
We acknowledge the work and cooperation of vascular neurologists, residents, anesthesiologists, and neurointerventional nurses in the management of these patients.
References
Supplementary materials
Footnotes
Contributors CCa: conception and design; analysis and interpretation of data; drafting of the article; participated in the direct treatment of patients in the study. LD: acquisition of data; analysis and interpretation of data; revision of the article critically for important intellectual content. SR, PG-B, MRG-S, CH, CCu: acquisition of data; revision of the article critically for important intellectual content; participated in the direct treatment of patients in the study. MG, NPdlO, MM, EL-C: acquisition of data; revision of the article critically for important intellectual content. AD: analysis and interpretation of data; drafting the article and revising it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests CC is Covidien consultant; AD is Co PI of REVASCAT trial; other authors report no conflict of interest. All the coauthors have reviewed and approved the final version of the manuscript. All coauthors had full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Provenance and peer review Not commissioned; externally peer reviewed.