Article Text

Abstract
Background The Low-profile Visualized Intraluminal Support (LVIS) Junior stent is newly approved for the treatment of wide-necked intracranial aneurysms.
Objective To report our multicenter experience with use of the LVIS Jr device.
Methods The neurointerventional databases of the participating institutions were retrospectively reviewed for aneurysms treated with LVIS Jr from the time of Food and Drug Administration approval until February 2016. All patients in the study period were included. Clinical presentation, aneurysm location, aneurysm size, vessel size, procedural complications, clinical and imaging follow-up were included in the analysis.
Results Eighty-five patients (54 female and 31 male) met the inclusion criteria for the study. Sixty-eight (80%) of the aneurysms were unruptured and the remainder were ruptured. The most common location of the treated aneurysms was anterior communicating artery (36%), middle cerebral artery bifurcation (22%), and basilar terminus (15%). The mean aneurysm size was 6.1 mm. The mean minimum parent vessel size was 2.3 mm. The LVIS Jr was successfully deployed in all but one case (99%). Initial angiographic results demonstrated Roy–Raymond class 1–2 occlusions in 61/84 patients (73%). At 6 months, 85% of the patients seen at follow-up had Roy–Raymond class 1–2 aneurysm occlusion. No procedure-related deaths occurred. Two cases of procedure-related complications (intraprocedural rupture and delayed rupture at day 2) were seen, leading to permanent neurologic morbidity. Both these cases were in patients with ruptured aneurysms.
Conclusions The LVIS Jr is a technically feasible, safe, and effective treatment for wide-necked intracranial aneurysms. Early results are promising but will need to be corroborated with longer-term follow-up.
- Aneurysm
- Coil
- Stent
Statistics from Altmetric.com
Introduction
Since its introduction three decades ago, endovascular coil embolization has become a well-established treatment for intracranial aneurysms.1–3 However, specific aneurysm morphology, such as a wide neck, makes coil embolization more challenging or impossible. Adjunctive methods, such as stent-assisted coiling (SAC), have been developed to approach those previously untreatable wide-necked aneurysms.4 ,5–7
The Low-profile Visualized Intraluminal Support (LVIS Jr; MicroVention-Terumo, Tustin, California, USA) device is a flexible, braided, self-expanding nitinol stent that has been recently approved for SAC in the USA. The positive features of the LVIS Jr design include delivery via a 0.017″ microcatheter or Scepter balloon (MicroVention-Terumo), ability to be deployed in smaller vessels than previous stents, resheath ability up to 80% of the deployment length, improved flow diversion, and control enabling a ‘shelf’ to be built at the site of wide-necked bifurcation aneurysms (figure 1).8–10

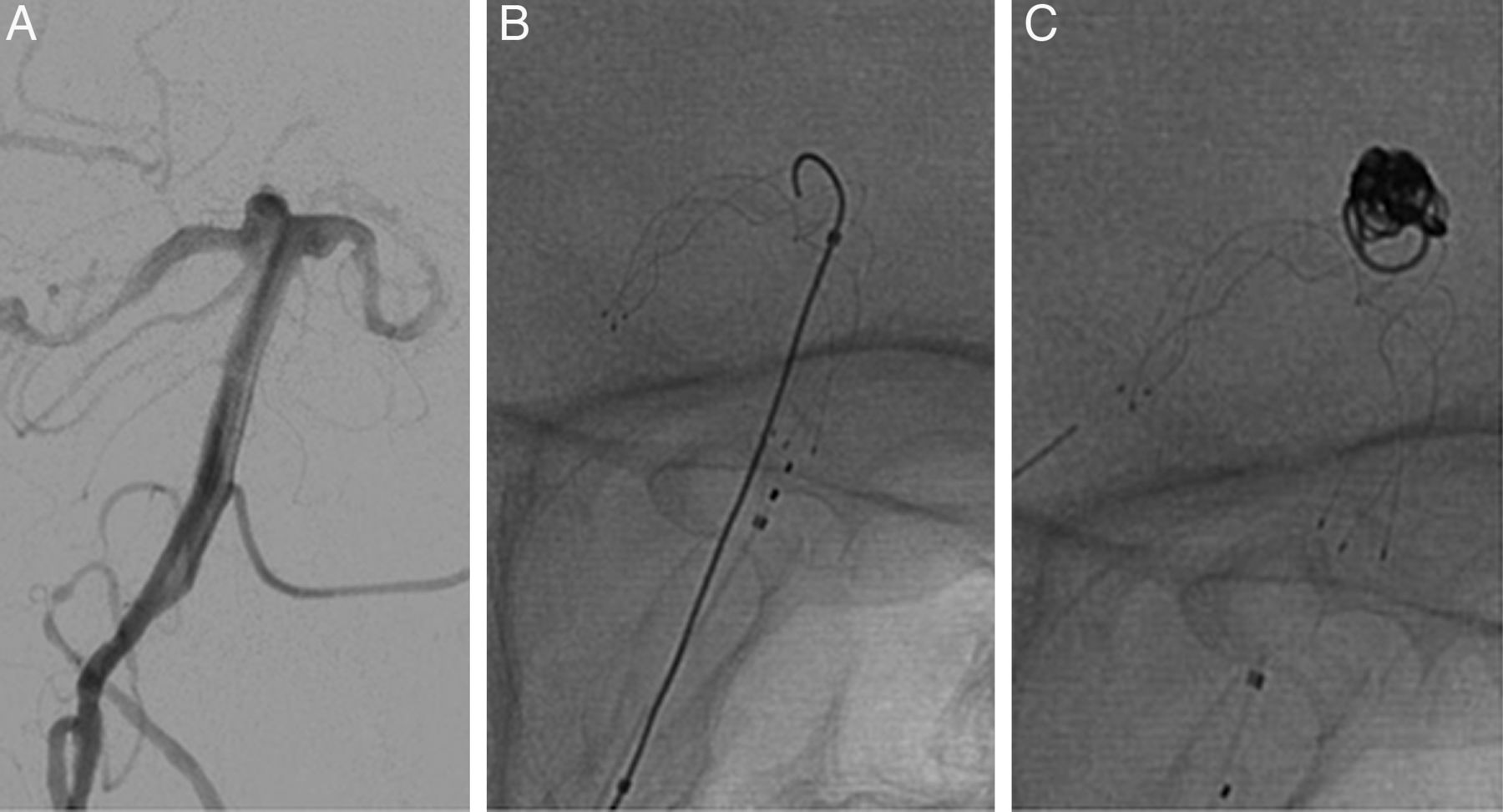
A patient with a ruptured wide-necked basilar apex aneurysm (A). Unsubtracted view showing the Low-profile Visualized Intraluminal Support (LVIS) Jr deployed with a ‘shelf’ across the aneurysm neck (B). Final unsubtracted image showing coil embolization with LVIS Jr and coils (C).
In this paper, we publish a large multicenter, post-Food and drug Administration approval, series of aneurysms treated with the LVIS Jr stent system.
Methods
We retrospectively reviewed the records of all patients treated with LVIS Jr stents at four tertiary care centers (Baptist Jacksonville, Baptist Miami, Grady Memorial Hospital, and Rush University). All patients were treated by fellowship-trained neurointerventional members of a multidisciplinary cerebrovascular service.
The charts were reviewed for basic patient demographic data. In addition, the treated aneurysms and associated vessels were analyzed for size parameters. The procedure data were analyzed for any periprocedural complications or technical difficulties with deployment of the LVIS Jr stent. Finally, patient outcomes were recorded, including data on complications, patient follow-up, and aneurysm occlusion rate based on the Roy–Raymond scale.11 All the above information was completed on a standardized form developed by the four centers. Each individual center collected their own data and reviewed their center's angiographic imaging, which was then entered on the standardized form.
All procedures were performed following written informed consent. All patients were premedicated with dual antiplatelet therapy. Platelet function tests were performed according to each center's protocol. All procedures were performed by experienced neuroendovascular surgeons with significant SAC experience. Intraprocedural heparinization was performed to achieve an activated clotting time >250 s. Heparin was discontinued on conclusion of the procedure. Dual antiplatelet therapy was continued for 6 months after the procedure.
All sites obtained local institutional review board approval for the study. Continuous variables are reported as mean±SD or median (IQR). Categorical variables are reported as proportions. Statistical analyses were performed using IBM SPSS Statistics 21 (IBM-Armonk, New York, USA).
Results
A total of 85 patients and aneurysms were treated in the study. Fifty-four patients were female and 31 were male. The average patient age was 60.5±12.7 years.
Sixty-eight (80%) of the treated aneurysms were unruptured and the rest were ruptured. The locations of the treated aneurysms are listed in table 1. The mean aneurysm diameter was 6.1±3.4 mm. All aneurysms were wide necked, defined as a neck diameter >4 mm and/or a dome:neck ratio <2:1.
Location of treated aneurysms
The LVIS Jr was successfully deployed in all but one case, where it failed to fully open and appose the vessel wall in tortuous anterior cerebral artery anatomy (figure 2). The stent was removed in this case and the aneurysm treated with a Neuroform (Stryker, Kalamazoo, Michigan, USA) stent-assisted coil embolization without complication. One case with temporary stent kinking also occurred, which resolved during the procedure with a fluffing technique (figure 3).

A patient with an unruptured wide-necked anterior communicating artery aneurysm and tortuous anterior cerebral artery anatomy (A). Subtracted (B) and unsubtracted (C) images of the Low-profile Visualized Intraluminal Support (LVIS) Jr stent not fully apposing the vessel walls. Final unsubtracted angiogram showing embolization with Neuroform stent and coils after the LVIS Jr was recaptured and removed (D).

A patient with an unruptured internal carotid artery terminus aneurysm (A). The 6 month follow-up angiogram demonstrates complete occlusion (B). Inter-procedure Low-profile Visualized Intraluminal Support (LVIS) Jr kink (C) was managed with a fluffing technique (D), leading to a fully open and apposed stent construct (E).
In 74 cases, a single LVIS Jr stent was deployed. The remaining cases had double stents deployed in ‘Y’ (seven cases), overlapping (two cases), and ‘T’ (one case) configurations. In one of the ‘Y’ stent cases a barrel vessel reconstruction device (Reverse Medical, Irvine, California, USA) and a LVIS Jr were used. In 59 cases, measurements of the parent vessel size were available. The mean minimum distal vessel size was 2.3 mm (range 1.2–3.5 mm).
For coiling, the microcatheter was jailed in the aneurysm before the stent deployment in 55 (65%) cases. In 22 (26%) cases the aneurysm was entered through the stent cells for coiling, and in 7 (8%) cases the stent was deployed after coiling owing to fear of coil prolapse.
Initial angiographic results consisted of Roy–Raymond class 1 in 36 cases (43%), class 2 in 25 cases (30%), and class 3 in 23 cases (27%). Radiographic follow-up at a minimum of 6 months was available in 49 cases with Roy–Raymond class 1 occlusion in 35 cases (71%), class 2 in 7 cases (14%), and class 3 in 7 cases (14%). No cases at follow-up had any significant stent migration or flow-limiting stenosis.
In eight cases procedure-related complications occurred (table 2). There were no procedure-related deaths. The complications led to permanent neurologic morbidity in two (2.4%) cases: one case of intraprocedural rupture and one of delayed rupture at postprocedure day 2. Both cases of permanent morbidity were in patients with ruptured aneurysms, giving an overall complication rate in ruptured aneurysms of 11.8% (2/17).
Listing of complications
Discussion
This manuscript provides the results of one of the largest published series of LVIS Jr stents. The primary finding is that the stent is feasible and safe in the treatment of wide-necked aneurysms. In our series, the stent was successfully deployed in 84/85 cases (99%), which is similar to the >90% success rate in other LVIS Jr studies.12–15 In only one case (figure 2) the stent did not fully appose the tortuous anterior cerebral artery anatomy, which is a potential limitation of the braided cell design. This is in comparison with the braided cell advantage of being able to build a ‘shelf’ across a wide aneurysm neck.8
The majority of our procedure-related complications were unrelated to the stent and transient. Our rates of transient (7%) and permanent (2%) complications are similar to, if not better than, those of other large published series of SAC.16 ,17 This low complication rate is particularly important, because many surgeons have used the high rate of complication seen in older SAC papers as rationale to treat wide-necked aneurysms with surgical clip ligation. Our paper indicates that these difficult lesions can be successfully treated with a low rate of complications.
This series also details the range of vessel sizes in which a LVIS Jr can be successfully deployed using its 0.017″ delivery catheter. The ability to treat aneurysms on small vessels is one of the technical breakthroughs of the LVIS Jr stent (figure 4). Alghamdi et al found similar results in a smaller series, in which the mean distal vessel diameter was 1.9 mm. In their study one case of 43 aneurysms treated had symptomatic intra-stent stenosis, which occurred at 6 months after the patient stopped their Plavix and aspirin.12 In our series, we had no cases of delayed complications.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A patient with a large posterior inferior cerebellar artery (PICA) aneurysm (A). Successful deployment of a Low-profile Visualized Intraluminal Support (LVIS) Jr stent from basilar artery to PICA (B) with final coiling angiogram (C).
Our rates of complete and near-complete occlusion at the time of coiling (73%) and at follow-up (85%) are similar to other published LVIS results. While some larger series of LVIS and LVIS Jr cases demonstrate complete or near-occlusion rates >90%, it should be noted that those studies include both the larger LVIS stent and the smaller LVIS Jr stent.10 ,14 This is important because in those studies the majority of the cases were internal carotid artery sidewall aneurysms, as opposed to our series where the majority of aneurysms were on distal bifurcation vessels, such as the anterior communicating artery or middle cerebral artery. In addition, the LVIS stent has a higher metal coverage and smaller pore size than the LVIS Jr, and accordingly the results from the combined studies are not comparable to the studies that involve only the LVIS Jr stent. Other smaller LVIS Jr studies which deal with the anterior communicating artery and middle cerebral artery, respectively, have demonstrated initial complete and near-complete occlusion rates of 83%, which is similar to our findings.18 ,19 Additionally, 20% of the aneurysms treated in our study were ruptured, which tends to result in higher rates of incomplete occlusion owing to concerns that the aneurysm might be unstable.
Recently, Shankar et al 20 reviewed 100 cases of LVIS Jr, and found an initial and 6 month complete and near-complete occlusion rates of 87% and 88%, which is similar to our data of 73% and 85%, respectively. There are some key differences, however, between our data and the Shankar paper. First, the aneurysm populations are somewhat different—while 58% of their aneurysms were wide necked, all of our cases were wide necked either by size or dome to neck ratio. Additionally, the locations of the aneurysms differ. Our study had a higher percentage of middle cerebral artery and other distal bifurcation aneurysms, which are important locations for the use of the ‘shelf’ technique that is a particularly distinguishing benefit of the braided LVIS Jr stent compared with other non-braided stents. In addition, 64% of the coil embolizations in our study were done by the jailing technique, whereas nearly all the cases in the other paper were performed through already deployed stent cells. Finally, our paper contains data on distal vessel measurements, which we believe is important information for the practitioner with these newer, smaller stents.
Given that this is a new ever-changing technology, we have compared our results with other published LVIS Jr studies (table 3). The table includes studies that used only the LVIS Jr but not those that used both the LVIS and LVIS Jr stents owing to the differences in technology described above, which make it difficult to determine the true data for the LVIS Jr stent.
Review of published LVIS Jr studies
Overall, the reported LVIS Jr rate of occlusion is better than published rates for Neuroform and Enterprise (Codman, Raynham, Michigan, USA) stents. King et al compared the literature on SAC from 2004 to 2014 and found that the rate of complete occlusion was 53% at the time of coiling and 69% at follow-up for all patients undergoing SAC.17 This increased rate of occlusion with LVIS Jr might be related to the increased metal coverage and corresponding enhanced flow-diversion properties of the hybrid closed cell design. The LVIS Jr stent has a level of metal coverage and flow diversion between that of traditional open-cell stents and true flow diverters. These results combined with the ability to access distal vessels with a smaller 017″ delivery catheter and precise deployment, make the LVIS Jr an interesting product in the neurointerventional arsenal.
This study had limitations. First, like any retrospective study, there is inherent selection bias. Additionally, we do not have long-term follow-up on some of our patients owing to the recent introduction of this technology in the US market.
Conclusion
This study demonstrates that use of the LVIS Jr stent in the treatment of wide-necked intracranial aneurysms is both feasible and safe. Early results are promising, but larger studies with longer follow-up should be conducted to conclusively prove its efficacy.
References
Footnotes
Contributors JAG conducted literature searches, collected data, drafted the initial version of paper, and revised later additions. RAH/GD/KK/DCH/ES/IL/DG/MB/PAS/MM/DKL collected data and revised later versions of the paper. RGN provided the initial idea for the study, collected data, and revised later versions of the paper.
Competing interests GD: consultant MicroVention. RAH: consultant, unrestricted educational grant MicroVention. DKL: research grant, advisory board and speaker MicroVention.
Ethics approval Institutional review board for each site. Emory/Grady for corresponding author.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data are available.