Article Text

Abstract
Objective To compare the efficacy and safety of our target puncture technique with the traditional technique during percutaneous kyphoplasty (PKP) for osteoporotic vertebral compression fractures (OVCFs) with intravertebral clefts (IVCs).
Methods 104 patients treated with PKP for single OVCFs with IVCs were retrospectively reviewed. All patients were divided into three groups: cleft filling by the traditional technique (Group A, n=18); interdigitated filling (Group B, n=50); and overfilling by the target technique (Group C, n=36). Oswestry disability index (ODI) and visual analog scale (VAS) scores and radiological evidence of vertebral body height and kyphotic angle, cement leakage, and adjacent vertebral fractures were studied before and after surgery (immediate, 1 and 2 years).
Results The ODI and VAS scores decreased for all patients and no significant difference was found between the three groups after treatment. However, 1 and 2 years after surgery a greater increase in ODI and VAS scores was observed in Group A compared with the other two groups. The initial correction of vertebral body height and kyphotic angle was not significant among the three groups. However, loss of correction was greater in Group A. No significant difference was found in cement leakage. The incidence of adjacent vertebral fractures in Group C was higher than in the other two groups.
Conclusions Different puncture techniques were initially effective for all patients with IVCs. However, cement cleft filling by the traditional technique was found to have less stability causing higher VAS/ODI scores and greater loss of correction. Hence, our target puncture technique was recommended in this study.
- CT
- Spinal cord
- Spine
- Technique
- Trauma
Statistics from Altmetric.com
Introduction
Osteoporosis is very common in the elderly population, becoming the leading cause of vertebral compression fractures as the size of the geriatric population increases.1 The appearance of intravertebral clefts (IVCs) after osteoporotic vertebral compression fractures (OVCFs) is not a rare phenomenon (incidence 10–48%).2 ,3 The IVC is presented as an important risk factor for severe vertebral collapse, progressive kyphosis, intractable back pain, and neurologic deficits.4 ,5 Hence, in order to restore spinal stability and obviate severe pain from OVCFs with IVCs, percutaneous kyphoplasty (PKP) has been widely recommended and has also achieved good outcomes at initial follow-up.6–8
However, previous studies9–11 have reported a high incidence of recollapse of the augmented vertebrae after PKP for the treatment of OVCFs with IVCs during long-term follow-up. Some authors have proposed that the presence of an IVC might be an important predisposing factor for recollapse.9 ,12 They demonstrated that cement in the IVC area was mainly filled with a solid lump mass because it is the fibrocartilaginous membrane at the periphery of the IVC area that prevents cement from diffusing sufficiently into the surrounding cancellous bone. We therefore attempted to make the cement to be sufficiently interdigitated with the surrounding cancellous bone by adopting our target puncture technique during PKP for treatment of OVCFs with IVCs. The purpose of the present study was to evaluate different cement filling patterns in the IVC area on the efficacy and safety of PKP for the treatment of OVCFs with IVCs when different puncture techniques were adopted.
Materials and methods
Selection of patients
To compare the efficacy and safety of our target puncture technique with the traditional puncture technique during PKP for treatment of OVCFs with IVCs, 845 patients who underwent PKP to treat single OVCFs from January 2008 to December 2013 were initially investigated. The inclusion criteria were as follows: (1) a single-level osteoporotic vertebral fracture at the thoracolumbar region (T11–L1) and no evidence of a previous adjacent osteoporotic vertebral fracture; (2) an IVC sign within the affected vertebra that could be detected either by CT, which showed a linear, triangular, or irregular region, or by MRI, which showed low signal intensity on T1-weighted images, high (fluid-containing) or low signal (gas-containing) on T2-weighted images;2 ,13–15 (3) a follow-up period of at least 2 years; (4) no additional history of trauma after surgery; (5) regular radiologic follow-up studies and continuation of osteoporotic medications throughout the follow-up period. Exclusion criteria were severe trauma, known malignancies, neoplastic fractures, and spinal infections.13 Finally, a total of 104 patients with IVCs were enrolled in our study, with a female to male ratio of 68 to 36 (mean age 74.32 years).
Operative procedure and grouping
The patients were divided into three groups: cleft filling by the traditional technique (Group A, n=18); interdigitated filling (Group B, n=50); and overfilling by the target technique (Group C, n=36).
All of the PKP procedures were performed by three spinal surgeons with more than 10 years’ experience (XJ, DL, and ZY). Each of the surgeons received standard training in PKP. The PKP technique was adopted by using a transpedicular approach (bipedicular needle insertion) in an extended posture under local anesthesia (1% lidocaine) in all cases according to methods of previous reports.6–8 ,16 For the traditional puncture operation in PKP treatment of OVCFs with IVCs, 11 or 13 gauge needles were inserted in a parallel or slightly descending course through the pedicle until the tip was optimally positioned in the IVC area under fluoroscopic guidance. The stylet was then removed from the trochar and a balloon was placed into the channel and inflated in order to elevate the endplate and restore the height of the vertebral body, thereby reducing the fracture. Poly(methyl methacrylate) (PMMA) powder with sterile barium sulfate (Tianjin Synthetic Material Research Institute, Tianjin, China) was injected into the IVC area for complete filling of the cleft, maximizing stabilization of the fracture fragments. Finally, cement injected by the traditional puncture technique was routinely filled with a solid lump pattern (the cleft group for Group A).
For our target puncture operation, most steps were similar to the traditional puncture operation in PKP for treatment of OVCFs with IVCs, as described above. However, the tip was positioned in the peripheral cancellous bone instead of being directly positioned in the IVC area. The deflated balloon was then continually inflated to compact the surrounding cancellous bone to form a cavity until the cavity broke through the periphery of the IVC and communicated with the IVC area. In this condition, cement injected could be sufficiently infiltrated into the surrounding cancellous bone and perform an extensive interdigitation in addition to being located in the IVC area (interdigitated group, Group B). Furthermore, cement could be interspersed throughout the cancellous bone space if the injection of cement into the affected vertebrae was continued even after the interdigitated filling pattern of Group B had been achieved (overfilling group, Group C), as shown in figures 1 and 2.

Diagrammatic representations of different puncture techniques used in percutaneous kyphoplasty for the treatment of osteoporosis vertebral compression fractures with intravertebral clefts (IVCs). (A–C) Group A: cleft filling pattern using the traditional puncture technique. (D–F) Group B: interdigitated filling pattern using the target puncture technique. (G–I) Group C: overfilling pattern using the target puncture technique. The white slit in the vertebral body (images A, D and G) represents the IVC, the red-dotted line (images B, E and H) represents the position of the inflated balloon, and the part of the vertebral body shaded black (images C, F and I) represents the region filled with cement.

Sagittal CT imaging manifestation of different distribution patterns of PMMA in the intravertebral cleft area using different puncture techniques. (A, B) Group A: cleft filling pattern of PMMA before (A) and after (B) percutaneous kyphoplasty (PKP). (C, D) Group B: interdigitated filling pattern of PMMA before (C) and after (D) PKP. (E, F) Group C: overfilling pattern of PMMA before (E) and after (F) PKP.
After PKP, self-ambulation was permitted as soon as possible after surgery. Back braces were applied to all patients for 1–2 months post-procedure. All patients used osteoporotic medications postoperatively; bisphosphonates and raloxifen were used in 13 and 5 patients in Group A, 32 and 18 patients in Group B, and 23 and 13 patients in Group C, respectively.
Evaluation of radiological parameters
We retrospectively measured preoperative and postoperative (day 1, 1 and 2 years) radiological parameters including vertebral height and kyphotic angle (KA) from sagittal radiographs. The vertebral height and KA were measured in accordance with previous methods described by Ha and Kim17 and Linn et al.13 Vertebral height was measured at the point of maximal compression of the augmented vertebrae. The vertebral compression ratio (CR) at each follow-up was measured as the ratio of the vertebral height of the augmented vertebrae to the mean vertebral height of the upper and lower vertebrae at the same site. The reduction rate (RR) was calculated using the difference between preoperative and immediate postoperative CR. The progressive height loss (PHL) was calculated using the difference between the immediate postoperative and last follow-up period. The KA was measured using Cobb's method, which is the angle between the upper endplate of the upper vertebra and the lower endplate of the lower vertebra. The reduction angle (RA) was calculated using the difference between the preoperative and immediate postoperative KA. The progressive angle (PA) was calculated using the difference between the immediate postoperative and last follow-up period. Additionally, the frequency and types of cement leakage and adjacent vertebral fractures were also determined postoperatively.
Evaluation of clinical parameters
Several preoperative clinical parameters including age, sex, bone mineral density (BMD), visual analog scale (VAS) score of back pain, and Oswestry Disability Index (ODI) were evaluated. Immediate postoperative and 1- and 2-year VAS and ODI scores were compared.
Statistical analysis
SPSS V.11.0 statistical software (SPSS, Chicago, Illinois, USA) was used for analysis. Comparisons were made before and at each postoperative follow-up appointment. Qualitative characteristics of groups were assessed using a one-way or repeated measures ANOVA and t-test. χ2 tests were performed for categorical variables. p<0.05 was considered statistically significant.
Results
One hundred and four patients (M/F 36:68) were categorized into the three groups as follows: 18 patients in Group A, 50 in Group B, and 36 in Group C. The mean age of the patients was 74.32±9.34 years and the length of follow-up ranged from 24 to 37 months (median 28 months). There was no significant difference between the three groups in baseline parameters including age, sex, BMD, VAS, ODI, vertebral height, and KA (p>0.05, table 1).
Baseline characteristics of the three groups by choosing different puncture techniques
Clinical findings
Compared with preoperative baseline values, the mean BMD had improved in all patients at 1 and 2 years after surgery, from −4.13±0.76 to −4.01±0.83 in Group A, from −4.11±0.76 to −3.97±0.69 in Group B, and from −4.23±0.93 to −4.01±0.78 in Group C. There was no significant difference in BMD at the same follow-up stage between the three groups.
The data presented in figure 3 show the change in VAS and ODI scores at 2-year postoperative follow-up. Immediately after surgery the mean VAS and ODI scores of all patients decreased significantly (p<0.001), with no significant difference between the three groups (p>0.05). However, we observed a gradual significant increase in VAS and ODI scores at 1 and 2 years after surgery in Group A. The VAS and ODI scores were significantly higher in Group A than in the other two groups at the 2-year postoperative follow-up (p<0.05). The VAS and ODI scores in Group A immediately after surgery were 1.88±1.14 and 28.09±6.03, respectively, and increased to 2.48±1.55 and 34.11±8.7 at 1 year and continued to increase to 3.08±1.55 and 41.03±8.9 at 2 years.

Analysis of variance models for the visual analog scale of back pain (VAS) scores and Oswestry Disability Index (ODI) indices (mean±SD): significant differences between groups at each time point and significant changes within groups over time are shown.
Radiological findings
The data presented in figure 4 show that CR and KA were significantly corrected immediately after surgery in all three groups (p<0.05), but had worsened at the 2-year follow-up. Among the three groups, the progression of CR and KA in Group A was significantly higher than that in Groups B and C 2 years after surgery (p<0.05). There was no significant difference between Groups B and C (p>0.05). RR and RA showed no significant difference among the three groups (p>0.05, table 2). However, PHL and PA were significantly higher in Group A than in the other two groups (p<0.05). There was no significant difference in PHL and PA between Groups B and C. Progression of recollapse of the augmented vertebrae in Group A was confirmed by analysis of radiological films from 2 years serial follow-up (figure 5).
Comparison of common complications and radiological parameters among the three groups
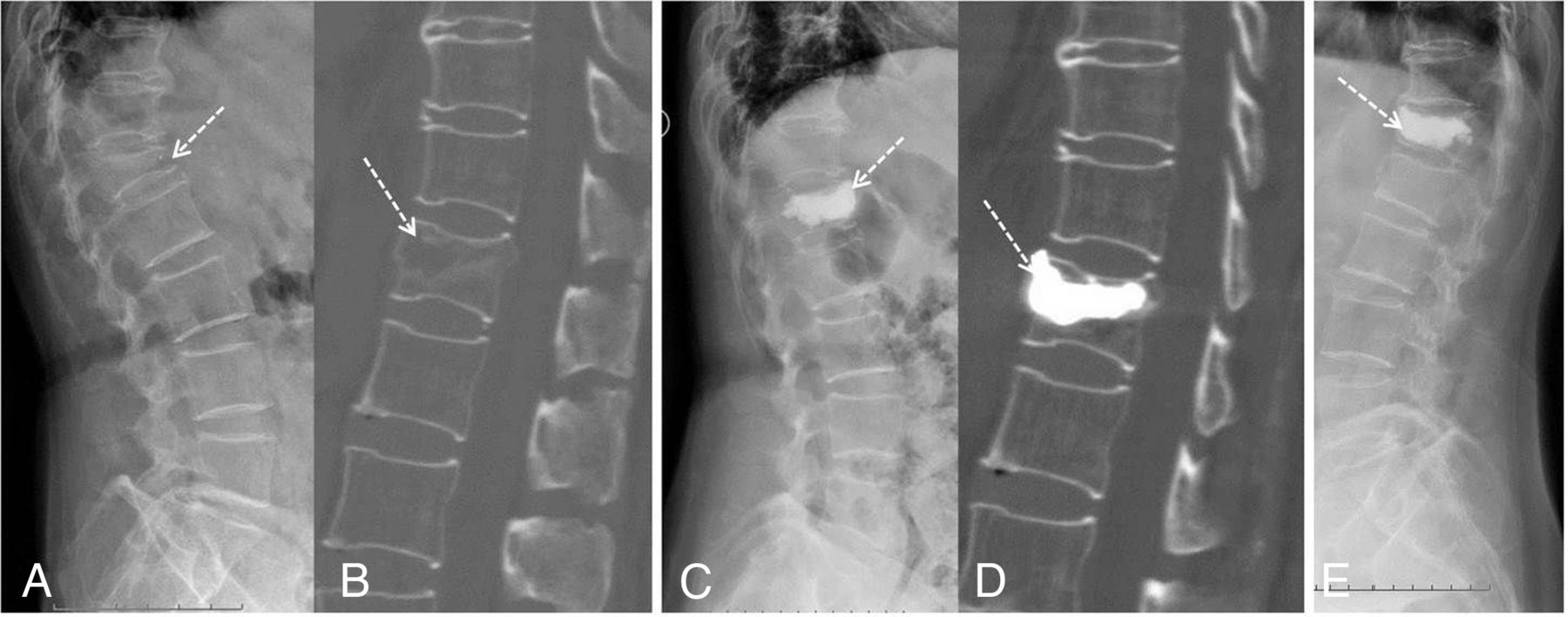
A 76-year-old female patient with an acute L1 osteoporosis vertebral compression fracture. Preoperative sagittal X-ray (A) and CT image (B) demonstrated intravertebral cleft sign adjacent to the superior endplate. (C, D) Immediate postoperative sagittal X-ray (C) and CT image (D) showed the cleft filling pattern of cement and re-expansion of the compressed vertebral body. (E) Severe recollapse of the augmented vertebrae developed at last follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Analysis of variance models for the vertical compression ratio (CR) and kyphotic angle (KA) values (mean±SD): significant differences between groups at each time point following the procedure and significant changes within groups over time are shown.
Complications
There was a significant difference in the amount of cement injected in the three groups (4.72±1.2 mL in Group A, 5.43±1.05 mL in Group B, and 6.42±1.2 mL in Group C; p<0.001). The frequency and type of cement leakage observed was as follows: 2/18 vertebrae in Group A (intradiscal in 1 (50%), perivertebral venous in 1); 10/50 vertebrae in Group B (intradiscal in 6 (60%), perivertebral venous in 3 (30%), epidural in 1 (10%)); 6/36 vertebrae in Group C (intradiscal in 3 (50%), perivertebral venous in 2 (33.3%), epidural in 1 (16.7%)). The most frequent leakage type was intradiscal in all three groups and there was no significant difference in the frequency and types of cement leakage among the three groups (p>0.05). Adjacent vertebral fracture was observed in 1/18 vertebrae in Group 1, 5/50 vertebrae in Group B, and 10/36 vertebrae in Group C. The incidence of adjacent vertebral fracture in Group C was significantly higher than in the other two groups (p=0.04, table 2). No other procedure-related complications occurred and the perioperative mortality was 0%.
Discussion
IVCs may be considered to be a sign of avascular necrosis of the vertebrae.2 ,3 Maldague et al 18 first associated avascular necrosis with the IVC sign in 1978. They collected the histologic data of one patient and radiological data of six patients and presumed that IVCs were a specific sign of local bone ischemia. Anatomic studies also supported the relationship between IVCs and avascular necrosis.19 The vertebral ventral zone at the thoracolumbar region is only supplied by anterior peripheral and metaphyseal arteries. When OVCFs occur, these weak arteries are insulted. Furthermore, insufficient revascularization and a bone fracture healing process occur.20 In addition, Dupuy et al 21 conducted a study of the substance compositions in the IVC area during CT-guided biopsies. They found that the substances in the IVC area were composed of necrotic cancellous bone, hyaline cartilage with fractured callus and fluid collections, which were associated with underlying avascular necrosis. Other workers also thought the presence of IVCs correlated with non-union and pseudoarthrosis of the affected vertebrae.22
According to previous reports,23 ,24 IVCs create instability within the fractured vertebral body which can be detected on radiographs comparing neutral with flexion and extension views. Hence, patients with IVCs usually have severe back pain and do not respond to conservative treatments such as bed rest and medication.6 ,20 It is therefore necessary to treat such patients by surgical intervention with PKP to restore spinal stability and stop progressive collapse of the affected vertebrae.6–8
In our study, all patients showed a significant improvement in both radiological and clinical evaluations at the initial follow-up period. However, several studies have reported a high incidence of recollapse of the augmented vertebrae after PKP for treatment of OVCFs with IVCs during long-term follow-up.9–11 Kim and Rhyu11 reported that 10 out of 24 patients with IVCs had a recollapse. Heo et al 9 reported 6 out of 21 IVCs. They thought that it was possible that the fibrocartilaginous membrane at the periphery of the IVC prevents cement being interdigitated with the surrounding cancellous bone and, hence, cement injected was mainly filled with a solid lump. This solid lump may induce greater stress upon the already weakened surrounding cancellous bone, causing a recollapse of the ‘PMMA-non supported’ area.9–11 In order to decrease recollapse of the augmented vertebral body, Niu et al 25 also thought that cement injected should fill the IVC area and be interdigitated with the surrounding cancellous bone through the diffusion of cement. However, the needle tip in their study was still traditionally placed in the IVC area and had a similar high incidence of recollapse (5/15 patients). We therefore considered that interdigitation with the surrounding cancellous bones was still insufficient when the traditional puncture technique was adopted (Group A).
In our study we adopted a target puncture technique in Groups B and C in which the inflated balloon could break through the periphery of the cleft and communicate with the IVC area. It could perform extensive interdigitation between the cement in the cleft and the cement in the cavity created by the balloon. When comparing the efficacy and safety of different cement filling patterns in the IVC area by different puncture techniques during PKP for treatment of OVCFs with IVCs, we found that there was no significant difference in the initial correction of vertebral height and KA immediately after surgery between the three groups. There was also no significant difference in the immediate postoperative VAS and ODI scores. However, during long-term follow-up we found that there was a significant difference in both clinical and radiological parameters between the three groups. The loss of correction in vertebral height and KA in Groups B and C by our target puncture technique was significantly lower than in Group A by the traditional puncture technique at final follow-up. The VAS and ODI scores also showed the same pattern. Furthermore, there was no significant difference in radiological and clinical parameters between Groups B and C. Finally, we demonstrated that cement filling patterns by our target puncture technique could improve the stability of the augmented vertebral body, causing less recollapse and better clinical outcomes.
Two common complications of PKP are cement leakage and adjacent vertebral fracture. Krauss et al 26 reported that cement leakage occurred in 18.2% of patients during PKP, and we found a similar incidence (17.3%). There was no significant difference between the three groups (11.1% in Group A, 20.0% in Group B, 16.7% in Group C). The most frequent leakage type was intradiscal leakage in all three groups, with no significant difference in the types of cement leakage. Yoshimura et al 27 reported that the cumulative incidence of new adjacent fracture ranged from 5.1% to 22.2% at >10 years follow-up. Trout et al 28 also stated a similar incidence (19.9%), and our result was similar to their results (16/104 patients). In our study the incidence of new adjacent vertebral fracture in Group C was significantly higher than in the other two groups (p=0.04). The biomechanical changes reported by Kim et al 29 and Wilke et al 30 also supported the results. They found that the stiffness of the augmented vertebra with overfilling distribution of cement was significantly higher than with solid lump filling of cement. This might induce a higher risk of a new fracture of the adjacent vertebral bodies in Group C.
In our study we have demonstrated the efficacy and safety of the target puncture technique in OVCFs with IVCs treated by PKP compared with the traditional puncture technique. We found that, compared with the cleft filling pattern of cement by the traditional puncture technique, the interdigitated and overfilling distribution pattern by our target puncture technique improves the stability of the augmented vertebral body, causing less recollapse and better clinical outcomes at final follow-up.
However, our study has some limitations. First, we used strict criteria for patient selection. We sought to evaluate results associated with the bony condition itself and to minimize extravertebral factors. Our efforts resulted in well-selected but small patient groups, especially in Group A. Second, we did not evaluate the adjacent cancellous bone edema on MRI,31–33 which possibly had an effect on our results. Finally, this was a retrospective study. A prospective study with a larger sample and longer-term follow-up is needed to verify the conclusion.
Conclusion
In this study different puncture techniques were initially effective for all patients during PKP for treatment of OVCFs with IVCs. However, compared with the cleft filling pattern of cement by the traditional puncture technique, both the interdigitated filling and overfilling patterns of cement by our target puncture technique improved the stability of the augmented vertebral body, causing less recollapse and better clinical outcomes at the final follow-up. Both the interdigitated filling and overfilling patterns had similar efficacy when our target technique was adopted.
References
Footnotes
WY and DL contributed equally.
Contributors WY, DL and XJ contributed to the conception and design of the study. ZY and WY performed the experiment. WY, LY, TQ analyzed the data. WY played the main role in writing the manuscript.
Funding This work was supported by projects of The Health Ministry of China (NO.W2012ZT07, NO.W2014ZT256) and Guangdong Province Medical Science and Technology Research Program (NO.B2014175).
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.