Article Text

Abstract
Background Modern stent retriever-based embolectomy for patients with emergent large vessel occlusion improves outcomes. Techniques aimed at achieving higher rates of complete recanalization would benefit patients.
Objective To evaluate the clinical impact of an embolectomy technique focused on continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE).
Methods A retrospective review was performed of 95 consecutive patients with intracranial internal carotid artery or M1 segment middle cerebral artery occlusion treated with stent retriever-based thrombectomy over an 11-month period. Patients were divided into a conventional local aspiration group (traditional group) and those treated with a novel continuous aspiration technique (CAPTIVE group). We compared both early neurologic recovery (based on changes in National Institute of Health Stroke Scale (NIHSS) score), independence at 90 days (modified Rankin score 0–2), and angiographic results using the modified Thrombolysis in Cerebral Ischemia (TICI) scale including the TICI 2c category.
Results There were 56 patients in the traditional group and 39 in the CAPTIVE group. Median age and admission NIHSS scores were 78 years and 19 in the traditional group and 77 years and 19 in the CAPTIVE group. Median times from groin puncture to recanalization in the traditional and CAPTIVE groups were 31 min and 14 min, respectively (p<0.0001). While rates of TICI 2b/2c/3 recanalization were similar (81% traditional vs 100% CAPTIVE), CAPTIVE offered higher rates of TICI 2c/3 recanalization (79.5% vs 40%, p<0.001). Median discharge NIHSS score was 10 in the traditional group and 3 in the CAPTIVE group; this difference was significant. There was also an increased independence at 90 days (25% traditional vs 49% CAPTIVE).
Conclusions The CAPTIVE embolectomy technique may result in higher recanalization rates and better clinical outcomes.
- Stroke
- Technique
- Thrombectomy
Statistics from Altmetric.com
Introduction
Embolectomy in combination with IV tissue plasminogen activator (tPA) is now the standard of care for patients with emergent large vessel occlusion (ELVO) in the anterior circulation who present within 6 hours from symptom onset.1–5 Several techniques for embolectomy are currently employed, including the use of primary local aspiration or stent retriever-based embolectomy. When stent retrievers are used there are options of using a guide catheter alone (placed in the cervical internal carotid artery (ICA)), a balloon guide to arrest flow during retrieval, or a local aspiration catheter. With regard to the latter, flow control with either a balloon guide or local aspiration catheters significantly decreases the number of small emboli compared with embolectomy without flow control,6–8 but there is one common feature—that is, the initial deployment of the stent retriever is performed without flow control.
Because we believe emboli can be released during initial stent retriever deployment and when withdrawn into a distal aspiration catheter, we developed a novel modification of the local aspiration stent retriever technique, which has four key components: continuous local aspiration prior to initial deployment and throughout embolectomy; engagement of the face of the embolus with the aspiration catheter; removal of the microcatheter to improve aspiration; and removal of the aspiration catheter and stent retriever as a single unit into the cervical sheath. We wanted to study the effect of this technique on recanalization and clinical outcomes.
Methods
Procedural technique
Conventional aspiration technique
In this group, a triaxial (or quadraxial) catheter system was used. A 6 Fr 90 cm Shuttle Sheath (Cook, Bloomington, Indiana, USA) was placed in the appropriate ICA. In cases of significant aortic tortuosity, an 8 Fr 45 cm sheath was initially placed in the thoracic aorta. Subsequently, a coaxial configuration of a Penumbra 5Max ACE64 (Penumbra, Alameda, California, USA) aspiration catheter, microcatheter, and microwire were advanced intracranially. After the microcatheter was advanced across the occlusion, the stent retriever of choice was deployed. Both Trevo (Stryker, Kalamazoo, Michigan, USA) and Solitaire (Medtronic, Irvine, California, USA) devices were used. In many cases, a gentle contrast injection was performed through the microcatheter to confirm placement beyond the clot and a more formal angiographic acquisition from the aspiration catheter after deployment of the stent retriever to assess for a flow channel. After a period of 3–5 min had passed and the stent retriever had a chance to integrate into the embolus, retrieval was performed. At this point the aspiration pump was turned on, when there was straightforward cervical segment anatomy, the aspiration catheter, microcatheter and stent retriever were removed as a single unit into the cervical sheath. Alternatively, the stent retriever and microcatheter were withdrawn into the aspiration catheter which was left in place, typically in the cavernous ICA. Control angiograms after each pass were performed to assess the degree of reperfusion. Repeat passes were at the discretion of the treating neurointerventionalist, but our institutional practice is to attempt to obtain at least Thrombolysis in Cerebral Ischemia (TICI) 2b flow, with the intent to perform embolectomy if there is residual occlusion of a proximal M2 branch. We do not routinely treat emboli beyond the proximal M2, and no patients had adjunctive IA tPA administered.
Continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) technique
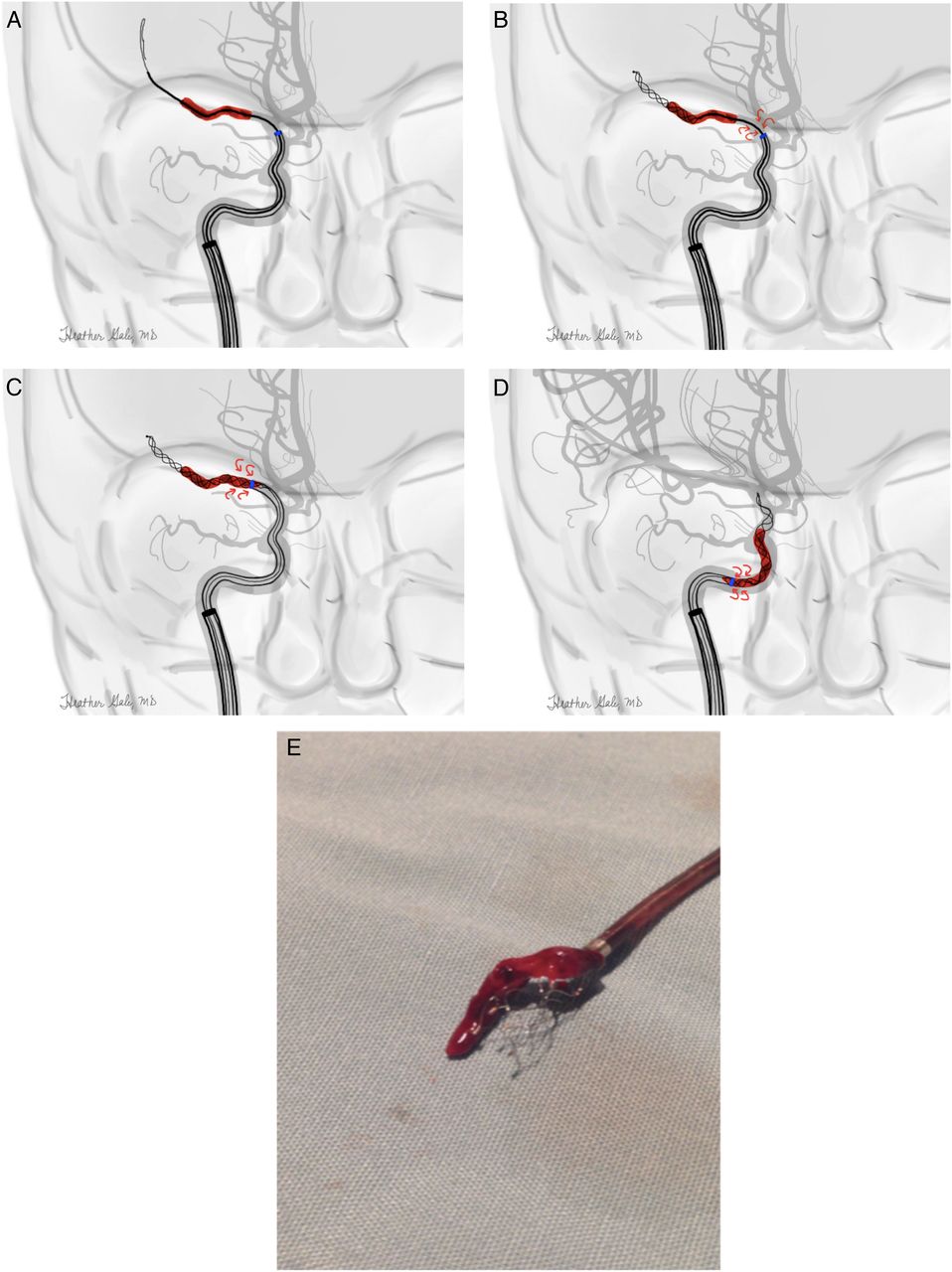
In order to potentially decrease the release of emboli which may occur during initial stent retriever deployment and improve the degree of reperfusion, we modified the technique, focusing on four major changes (see figure 1):
After the thrombus has been crossed with the microcatheter, the local aspiration catheter is connected to the continuous aspiration pump immediately prior to deployment of the stent retriever. This maneuver is postulated to improve flow control prior to deployment and may reduce the dispersion of emboli. While balloon guide catheters are commonly used in thrombectomy, balloon inflation is typically during withdrawal rather than deployment. In addition, they only control the inflow from the ipsilateral ICA whereas local aspiration allows for control of inflow from the posterior communicating artery and anterior communicating arteries.
Once fully deployed, the aspiration catheter is advanced over the stent retriever and microcatheter to just adjacent to the face of the thrombus. In cases with tortuous anatomy, the stent retriever often acts as a ‘grapple hook’, facilitating navigation around the ophthalmic segment of the ICA. During this process we monitor the drip rate on the aspiration tubing. Once the drip rate on the tubing has slowed or stopped, we feel as though the thrombus has been ‘engaged’ (‘corked’ or ‘held captive’ are other descriptive terms we use). At this point, no further advancement of the aspiration catheter is performed.
Now that the aspiration catheter has been placed near the face of the thrombus, we remove the microcatheter to improve aspiration performance. This has been shown experimentally to significantly increase the suction force.9 Again, we monitor the drip rate on the aspiration tubing to ensure near stasis.
We then retrieve the thrombus by removing the aspiration catheter and stent retriever as a single unit into the cervical guide catheter. It is helpful to place the torque device on the stent retriever delivery wire to fix the position of the stent retriever relative to the aspiration catheter in order to minimize the risk of a portion of the thrombus being sheared off. The aspiration catheter and stent retriever are then removed as a single unit in a slow controlled fashion into the sheath positioned in the cervical ICA.

Continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) technique. Illustrative example of the use of the CAPTIVE technique to treat an M1 segment occlusion. We routinely place the large guiding sheath in the cervical internal carotid artery. (A) The triaxial system including the distal aspiration catheter, microcatheter, and microguidewire are advanced as a unit, with the microcatheter and guidewire traversing the occluded segment. (B) In the next step, local aspiration is turned on (red arrows) prior to deployment of the stent retriever. (C) The stent retriever is then completely deployed and the microcatheter removed in order to improve the aspiration force. After the microcatheter has been removed, the distal aspiration catheter is advanced over the stent retriever wire until the drip rate slows, indicating the thrombus has been ‘engaged’ or ‘held captive’ by the aspiration catheter. (D) In the withdrawal step, it is critical to remove the aspiration catheter and stent retriever as a single unit into the cervical sheath. (E) Gross specimen picture shows how the stent retriever has captured the embolus, with a portion held ‘captive’ within the distal aspiration catheter.
With regard to changes 1 and 2 above, microcatheter contrast injections to document a position beyond the clot were typically deferred when continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) was employed and runs through the aspiration catheter after stent retriever deployment were never performed. With regard to change 4 above, it is important not to allow the aspiration catheter to advance appreciably over the stent retriever/embolus complex. Doing so may result in shearing of a portion of the embolus as it is withdrawn into the aspiration catheter (figure 2). Greater fragmentation and the dreaded embolization to a new vascular territory will likely occur if the stent retriever is withdrawn completely into the aspiration catheter intentionally rather than into the cervical sheath.

Incorrect technique (‘De-Captive Shear’) showing withdrawal into aspiration catheter instead of guiding catheter. In this process the aspiration catheter is advanced over a portion of the embolus (A), with the potential for a ‘shoulder’ effect to develop along the edges of the aspiration catheter. As the embolus is withdrawn into the distal catheter, small fragments may break off and embolize to the distal territory (B). While this may still allow for Thrombolysis in Cerebral Ischemia (TICI) 2b recanalization, the likelihood of TICI 2c or 3 recanalization may be less.
Data analysis
Institutional review board approval was obtained for a retrospective review of all patients undergoing mechanical thrombectomy at a single comprehensive stroke center between 1 July 2015 and 31 May 2016. We included all patients with an occlusion of the ICA terminus or M1 segment of the middle cerebral artery. In order to facilitate comparison between these two techniques, we excluded patients with more distal occlusions, posterior circulation stroke, or those with tandem extracranial and intracranial occlusions. All patients were treated with conscious sedation, except those who had been intubated previously for airway concerns. We did not electively intubate any patients. Patients were divided into conventional aspiration or CAPTIVE groups depending on the procedural technique used. In cases were both techniques were used, the patient was considered to be in the CAPTIVE group.
The stroke center quality database was searched for the following: patient age, gender, site of intracranial location, admission National Institute of Health Stroke Scale (NIHSS) score, Alberta Stroke Program Early CT Score (ASPECTS) on non-contrast CT scan (NCCT), and whether or not IV tPA was administered. We also assessed key time intervals including time from symptom onset, NCCT and CT angiography to start of angiography, as well as time from groin puncture to final recanalization.
Image analysis
All post-procedural angiograms were reviewed independently by two experienced interventional neuroradiologists (RAM, MVJ) in a delayed fashion, blinded to treatment technique. They were scored using the traditional modified TICI (mTICI) incorporating the 2c category.10 This new category has been proposed to represent a degree of near complete reperfusion. In cases of disagreement, a consensus was obtained at a later date. We also scored for embolization to new territory, blinded to the technique used.
Statistical methods
All analyses were conducted using SAS Software V.9.4 (SAS, Cary, North Carolina, USA). Baseline differences between the CAPTIVE and traditional techniques were examined using a Pearson's χ2 test or Fisher's exact test with PROC FREQ for count data and Wilcoxon test for ordinal and continuous data with PROC NPAR1WAY. Time intervals were estimated using Kaplan-Meier estimation; because there were no censored events, differences between the CAPTIVE and traditional techniques were examined using a Wilcoxon test with PROC LIFETEST. Clinical outcomes for NIHSS and mRS were assessed using both a Wilcoxon test and a Fisher exact test. NIHSS was also examined relative to baseline between the CAPTIVE and Traditional techniques using generalized mixed modeling assuming a binomial distribution (0–42) with PROC GLIMMIX using classic sandwich estimation. Statistical significance was defined at the 0.05 level and all interval estimates were calculated for 95% confidence.
Results
Demographics and time intervals
As indicated in table 1, few differences were observed at baseline between patients undergoing the traditional technique (n=57) and those who received the CAPTIVE technique (n=39), except for a higher rate of pretreatment with IV tPA in those receiving the traditional technique than in patients receiving the CAPTIVE technique (68% vs 44%). In addition, 28% of those receiving the traditional technique had diabetes compared with 10% of those receiving the CAPTIVE technique. No differences were observed in time between the CAPTIVE and traditional techniques, with the exception of recanalization time where median time was reduced from 31 min (traditional technique) to 14 min (CAPTIVE technique).
Demographic characteristics of the two patient groups
As shown in table 2, the median NIHSS scores after 24 hours and discharge were both significantly lower in patients treated with the CAPTIVE technique than in those treated with the traditional technique; likewise, the decrease between admission and 24 hours and discharge were both significantly larger for the CAPTIVE group than for the traditional technique. In addition, median mRS scores were significantly lower for patients treated with the CAPTIVE technique than for those undergoing the traditional technique; likewise, favorable outcome was almost double for those receiving the CAPTIVE technique compared with the traditional technique (49% vs 25%).
Clinical outcomes in all patients

{kind=link}
{kind=link}
{kind=link}
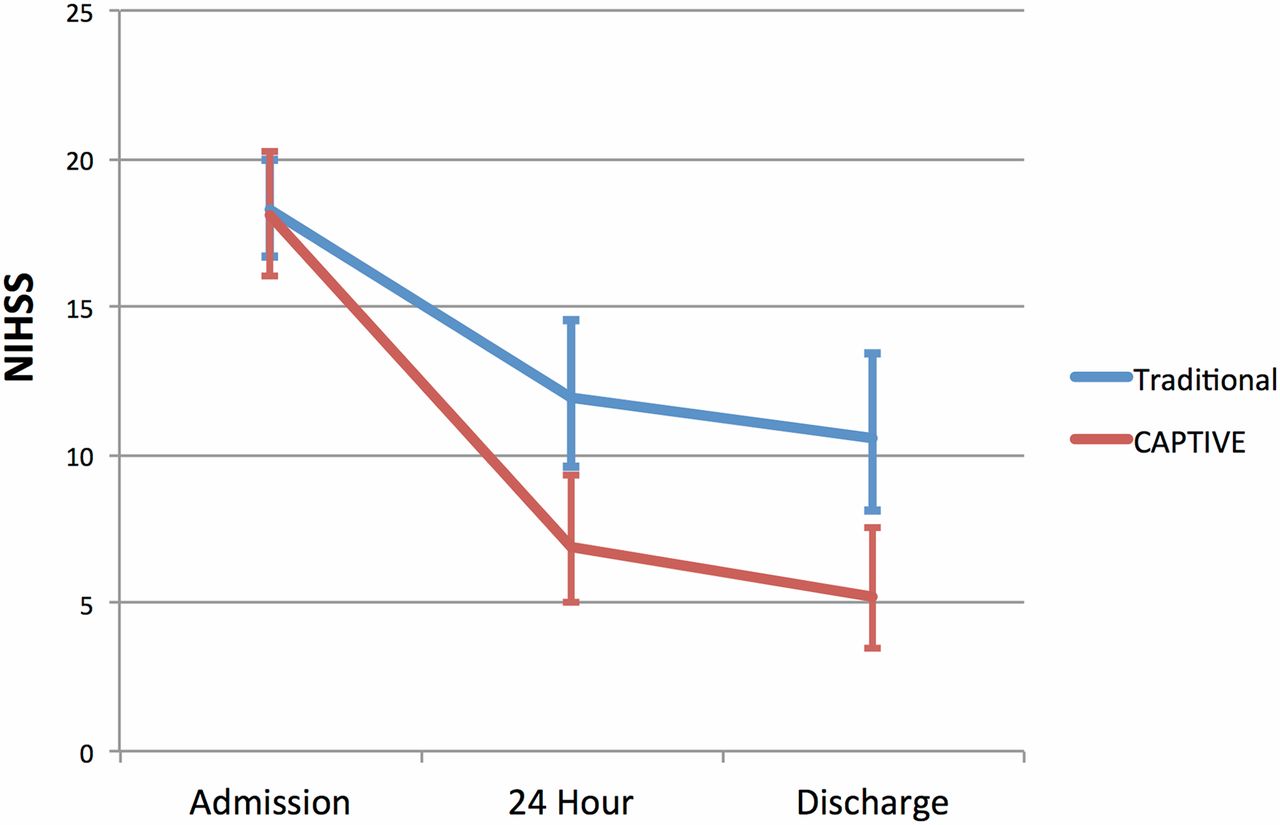
Comparison of clinical improvement in National Institute of Health Stroke Scale (NIHSS) score at 24 hours and at discharge between the traditional and continuous aspiration prior to intracranial vascular embolectomy (CAPTIVE) groups.
For thoroughness, a moderation model was examined for the NIHSS score between the CAPTIVE and traditional techniques over time. As shown in figure 3, no difference was observed in NIHSS score at admission between the traditional (18.3, 95% CI 16.7 to 19.0) and CAPTIVE (18.1, 95% CI 16.0 to 20.2) techniques. Although both groups experienced a reduction in NIHSS at 24 hours and discharge, patients treated with the CAPTIVE technique had a significantly lower NIHSS score at 24 hours (6.9, 95% CI 5.0 to 9.3 vs 11.9, 95% CI 9.6 to 14.6) and at discharge (5.2, 95% CI 3.5 to 7.7 vs 10.6, 95% CI 8.1 to 13.4) than patients treated with the traditional technique (p=0.0049). Specifically, those treated with the CAPTIVE technique experienced a reduction in NIHSS at discharge from admission of 71% while those treated traditionally experienced a reduction of only 42%.
Discussion
We show how a series of four simple modifications to the conventional local aspiration technique has the potential to result in near complete recanalization in significantly more patients. In addition, the CAPTIVE technique was faster, with a median groin puncture to recanalization time of just 14 min. These benefits also translated to dramatic improvements in early neurologic recovery, lower 24 hour and discharge NIHSS scores, and a higher rate of independence at 90 days.
It is possible that much of the improvement is due to a greater degree of recanalization. Given that most patients with ELVO do not have multifocal emboli, it is postulated that distal emboli likely result from clot fragmentation during thrombectomy. The modifications we describe in the CAPTIVE technique may play a role in minimizing fragmentation, both of fresh thrombi formed adjacent to the embolus and of the primary embolus itself. Indeed, our rates of mTICI 2c or 3 recanalization were nearly doubled with this technique, while the overall rate of TICI 2b/2c/3 rates in both groups were similar. This would suggest that our technique decreases the likelihood of embolus fragmentation.
The use of primary aspiration alone, termed ADAPT, has been well described, and has shown high rates of rapid recanalization.11–13 However, we feel our technique may represent a potential improvement over ADAPT as the use of the stent retriever provides an additional layer of mechanical capture of the thrombus. It is unknown whether CAPTIVE is superior to ADAPT, and a direct comparison may be warranted. However, both techniques use local aspiration with large-bore catheters, and therefore are likely more similar than the use of a cervical balloon guide catheter.
An in vitro analysis of the CAPTIVE technique seems warranted. It would be helpful to determine in a thrombectomy model if the concept of continuous local aspiration prior to stent retriever deployment results in fewer distal emboli, similar to a comparison that has been previously performed for other techniques.6 ,7
There are drawbacks to this analysis. This is a single-center retrospective series, with all patients treated by experienced operators. In addition, we did not compare CAPTIVE with ADAPT. Our overall rates of functional independence are slightly lower than some of the recent trials, but this may be reflective of real-world performance. Our median age is almost 10 years older than patients in the five recent trials, and this may contribute to the slightly lower rates of functional independence seen.14 In addition, we did not screen patients extensively for functional independence prior to thrombectomy. It is possible that many of our elderly patients with a baseline mRS >1 would have been excluded from these recent trials. We also limited our analysis to ICA terminus and M1 occlusions, excluding tandem (cervical plus intracranial) lesions, isolated M2 occlusions, and posterior circulation lesions. While the CAPTIVE technique can certainly be used in those situations, we felt that a more homogenous sample would facilitate comparison between the two techniques.
Conclusion
We describe a modification to the local aspiration and stent retriever-based thrombectomy techniques termed CAPTIVE. The primary modifications are the use of continuous local aspiration prior to stent retriever deployment, engagement of the face of the thrombus with the aspiration catheter, removal of the microcatheter to increase suction, and controlled deliberate removal of the stent retriever/embolus complex. This technique results in very high rates of TICI 2c/3 recanalization, decreases recanalization time, and improves the likelihood of early neurologic recovery and functional independence at 90 days compared with the traditional aspiration technique. Further study of the CAPTIVE technique is warranted.
References
Footnotes
Contributors All authors were responsible for substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None declared.
Ethics approval Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.