Article Text

Abstract
Background Venous sinus stenting for dural sinus stenoses is an emerging alternative to cerebrospinal fluid diversion in cases of medically refractory idiopathic intracranial hypertension. Juxta-stent ‘re-stenoses’ have been reported and managed alternatively with ventricular shunting or stent revision. Identification of factors that might predispose patients to recurrent narrowing may help to select or exclude patients with idiopathic intracranial hypertension for venous sinus stenting.
Methods We retrospectively reviewed a prospectively maintained database spanning December 2011 to May 2015 of all patients with idiopathic intracranial hypertension who were screened for possible venous sinus stenting, including only patients who received a stent, noting symptomatic improvements, changes in opening lumbar puncture pressure, demographic characteristics, and any subsequent intervention after stent placement. Fisher's exact test and logistic regression were used to test each of seven potential predictors for retreatment.
Results There were eight revisions in 31 patients (25.8%). Among Caucasians, 8.0% required a revision compared with 100% of African-Americans (p<0.001). The c-index for race was 0.857. Body mass index (BMI) was also a significant predictor of revision (p=0.031): among class III obese patients the revision rate was 46.2% compared with 16.7% among class I and II obese patients and 0% among overweight to normal weight patients.
Conclusions BMI was a significant predictor of revision, suggesting that higher BMI may have a higher risk of revision. The small number of African-Americans in the study makes interpretation of the practical significance of the revision rate in these patients uncertain. None of the other studied factors was statistically significant.
- Angiography
- Device
Statistics from Altmetric.com
Introduction
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, is a disease characterized by increased intracranial pressure (ICP) without evidence of a primary intracranial disease such as a mass, hemorrhage, or other space-occupying or obstructive lesion. IIH is seen most frequently in young women with higher body mass index (BMI), which is thought to result in cerebral venous hypertension due to increased pressures throughout the thoracic and abdominal cavities,1 and manifests with headaches and visual obscuration related to papilledema. Prolonged elevated ICP may result in optic nerve damage and irreversible loss of vision.
Presently, first-line therapy for IIH is weight loss, as well as symptomatic treatment with medication. Carbonic anhydrase inhibitors such as acetazolamide and topiramate have been used to reduce cerebrospinal fluid (CSF) production2 ,3 in order to reduce intracranial hypertension-related symptoms. However, both medications have side effects and may be ill-tolerated. Patients with continued symptoms while on medication and attempting weight loss, particularly visual obscurations, may require CSF diversion via either shunt placement4 or optic nerve sheath fenestration.5 Although the former may be complicated by shunt malfunction such as infection or occlusion, it is very effective at reducing ICP. Optic nerve sheath fenestration involves perforating the optic nerve sheath by creating slit-like longitudinal incisions, allowing flow of CSF out of the nerve sheath and into the orbit and periorbita. Another option is surgical weight loss with a gastric bypass procedure, which has been shown in small series to be effective although it may be complicated by nutritional compromise and anastomotic leaks.6 ,7
Venous hypertension has been implicated as a primary mechanism for IIH,8 which may arise from either intracranial (venous stenoses) or intrathoracic sources (obesity and central venous hypertension). Venous stenoses have been described in up to 90% of patients with IIH,9 which may improve after reduction of CSF pressure via CSF drainage.10 Controversy as to whether venous stenoses and venous hypertension are the cause or effect of increased ICP remains.11 In addition, venous thrombosis, rather than merely stenosis, has also been implicated as a cause for increased CSF pressure,12 ,13 although the pathomechanism for this may involve CSF or ICP disequilibria or both. Dural arteriovenous fistulas, which cause venous hypertension, have also been shown to result in increased ICP.14
Experience with venous sinus stenting to relieve ICP gradients has increased over the past years, demonstrating high safety and efficacy15–22 as well as durable results19 ,22 (table 1). Moreover, cost analysis may favor stenting over CSF diversion in certain healthcare models.23
Summary of idiopathic intracranial hypertension stenting studies
However, in these reports, juxta-stent narrowing has been reported as well as subsequent intervention with CSF diversion or additional stents when there are recurrent headaches or further visual compromise. If such a patient population can be prospectively defined, stent procedures may be obviated, proceeding directly to a different form of CSF diversion. The goal of this study is to identify baseline predictors of retreatment after endovascular dural sinus stenting for the medical treatment of refractory IIH cases.
Methods
This is a retrospective study of patients undergoing transverse sinus stent placement to treat pseudotumor cerebri in a single center. We retrospectively reviewed a prospectively maintained database spanning December 2011 to May 2015 of all patients with idiopathic intracranial hypertension who were screened for possible venous sinus stenting. Included in this analysis are patients who received an endovascular dural sinus stent placement. The patients' gathered data included: demographics, relevant medical history, symptomatic improvements, intrinsic cause of venous pressure hypertension (ie, arachnoid granulation or thrombosis), change in venous pressure measurements, and any subsequent intervention after stent placement. Magnetic resonance venography was used to evaluate the patients prior to the intervention.
Endovascular dural sinus stenting
Intracranial stenting was performed alongside venous pressure monitoring in the same setting. Venous pressure was measured under light sedation with a Renegade Hi-Flo microcatheter (Boston Scientific, Natick, Massachusetts, USA) advanced through a 5 F vertebral catheter. Venography was performed through the microcatheter.
If a measured gradient exceeded 8 mm Hg across a venous narrowing, the patient was placed under general anesthesia for treatment via endovascular stenting. A 6 F guide sheath was then advanced into the ipsilateral jugular vein with an internal 0.070 inch intermediate catheter and Renegade Hi-Flo microcatheter over microwire in a coaxial technique. The intermediate catheter was then advanced to the torcula to perform high volume venographic injection. With the intermediate catheter across the stenosis and the inflow of the vein of Labbe, the selected stent (self-expanding Zilver biliary stent; Cook Medical, Bloomington, Indiana, USA; 7, 8 or 9 mm×30, 40 or 60 mm depending on the extent of the stenosis) was advanced within the intermediate catheter into a position across the stenosis under roadmap guidance, followed by unsheathing of the stent delivery system and delivery of the stent itself (figure 1). A repeat venous pressure measurement was performed after stent deployment. The dominant sinus was chosen for stenting. Post-stenting venoplasty has not been required for any patient. All patients received dual antiplatelet inhibition therapy with daily aspirin 325 mg and clopidogrel 75 mg for 3 months after stent placement, then only daily aspirin 325 mg for another 3 months. Thereafter, patients were kept on aspirin 81 mg for life. Follow-up consisted of clinical and imaging evaluation (either CT or MR venography). Upon recurrent symptoms, patients had a repeat lumbar puncture and, when >25 cm H2O, the endovascular pressure gradient across the transverse sinus stenosis was remeasured.
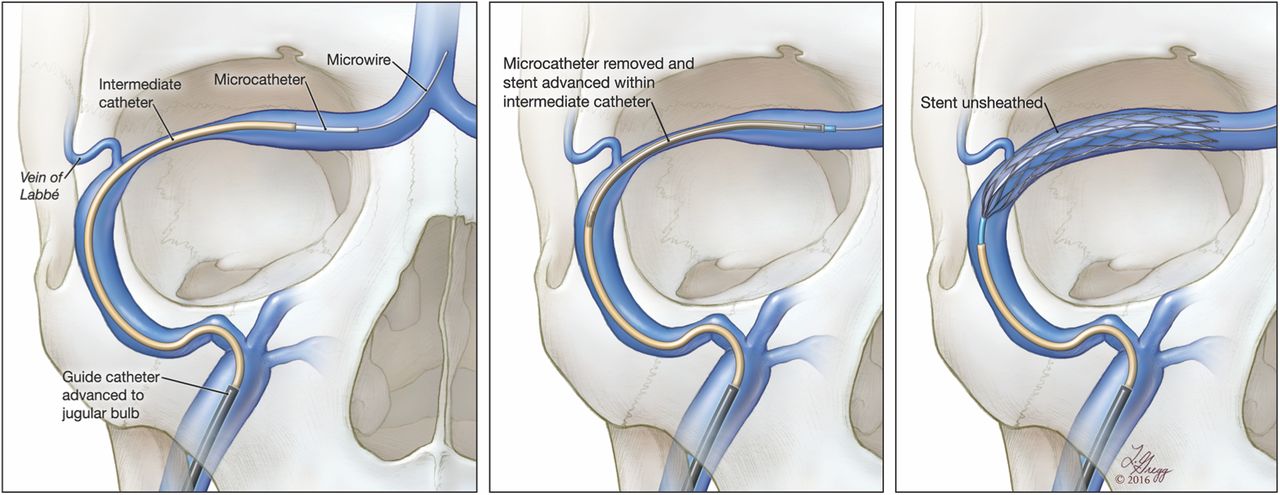
(A) Artist's drawing of intermediate catheter and stent delivery catheter across the stenotic segment and entry point of the vein of Labbe. Guide sheath is in place for support in the sigmoid–jugular junction. This technique shields the rigid stent delivery complex from exposure to the endothelium. (B) Intermediate catheter has been withdrawn exposing the stent catheter across the stenotic segment. (C) Stent catheter has been withdrawn exposing the stent, deploying the device across the stenotic segment. Reproduced by Lydia Gregg.
Statistical methods
In order to assess whether a documented variable might predict such a recurrence of symptoms, the prospectively collected data were retrospectively analyzed to assess whether BMI, concomitant medical condition, pre-procedural internal jugular pressure, post-procedural torcular pressure, post-procedural torcular–internal jugular pressure gradient, post-procedural internal jugular pressure, or stent size might be used as a predictor for need for subsequent therapy, be it an additional stent or CSF diversion.
Fisher's exact test (for categorical variables) and logistic regression were used to test each of the potential predictors of retreatment. BMI was assessed both as a continuous variable and as an ordinal variable based on the WHO classification where <30 kg/m2 is normal to overweight, 30–34.9 kg/m2 is obese class I, 35–39.9 kg/m2 is obese class II, and ≥40 kg/m2 is obese class III. A significance level of 0.05 was used for each predictor with no multiplicity adjustment, given the small sample size and exploratory nature of the study. The c-index was used to characterize the discrimination ability of the predictor. A c-index of 1.0 indicates perfect discrimination between patients who require a revision versus those who do not whereas a c-index of 0.5 indicates chance guessing. Note that, because of the small sample size, particularly the small number of cases requiring a revision, a multivariable analysis to assess the simultaneous effects of various predictors could not be performed.
Results
Data were available for 31 patients. The mean (SD) age of the patients was 33.9 (11.5) years (range 18–67 years). There were 29 women (93.6%) and two men (6.4%). Five were African-Americans and 26 were Caucasians. Eight patients (25.8%) had an endocrine disorder and four (12.9%) were steroid immunosuppressive. Regarding relevant medical history, the relationship with connective tissue disease was analyzed but only one patient was positive and no statistical analysis was possible. Table 2 summarizes the characteristics of the study population. The mean (SD) venous pressure gradient was successfully reduced from 20.1 (10.7) mm Hg pre-stenting to 2.4 (2.9) mm Hg post-stenting. Seventeen patients (54.9%) received an 8 mm stent, nine (29%) received a 7 mm stent, and five (16.1%) received a 9 mm stent; five patients received double stenting. Twenty-three (74.2%) were treated successfully with endovascular stenting while eight patients (25.8%) had symptomatic recurrence of IIH necessitating a revision. All eight patients who required retreatment presented with recurrent headache symptoms within 6 months of endovascular stenting, while none presented with recurrent papilledema.
Description of study sample
Table 3 summarizes the results for each potential predictor of a revision. Race and BMI were the only significant predictors of retreatment. Among Caucasians, 8.0% required a revision compared with 100% of African-Americans (p<0.001). The c-index for race as a predictor was 0.857, indicating that race is a strong predictor for the need of revision.
Potential predictors for retreatment
BMI classified using the WHO groups was also a significant predictor, showing that patients with higher BMIs had a higher likelihood of a revision (p=0.031). BMI class was also a significant predictor of revision (p=0.031). Among class III obese patients, 46.2% (6/13) required a revision compared with 40% (2/5) of class II obese patients, 0% (0/7) of class I obese patients, and 0% (0/6) of normal weight patients. The c-index for BMI class was 0.793. Note that mean BMI was significantly higher for African-Americans than Caucasians (47.0 vs 36.3, p=0.035), thus in this small study it is difficult to separate the effects of race and BMI on revision rate.
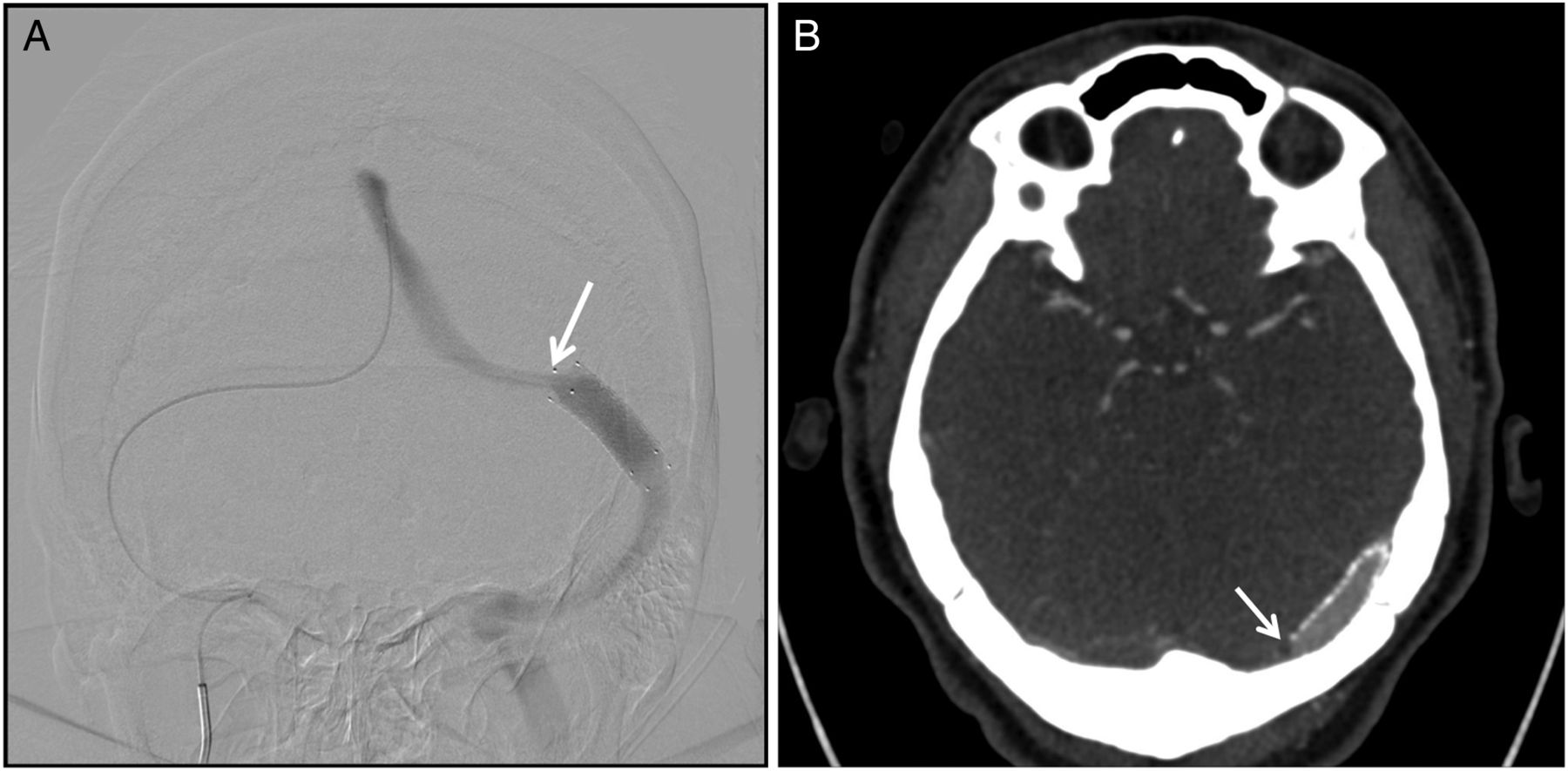
Review of treatment results were as follows: improvement in papilledema in 30/31 (96.8%), improved lumbar puncture (LP) pressures in 15/22 (68.2%) who had repeat LP pressure measurements, resolution of tinnitus in 18/19 (94.7%) who reported tinnitus, and improvement in headaches in 23/31 (74.2%) of patients. There were no significant complications. One patient had a small subdural contrast collection associated with microcatheter injection against the wall of the sinus. There were no incidences of in-stent thrombosis. All retreatment cases (seven patients received ventriculoperitoneal shunt and one patient had a re-stenting) were associated with a narrowing of the sinus proximal to the dural stent, as defined by the direction of blood flow (figure 2). The repeat endovascular pressure gradient measurement in these patients revealed comparable gradient before stenting (data not shown).

{kind=link}
{kind=link}
(A) Digital subtraction venography demonstrates narrowing of the transverse sinus adjacent to the previously placed stent compatible with a proximal ‘juxta-stent’ stenosis. (B) CT venography demonstrates abrupt narrowing of the transverse sinus proximal to the stent.
Discussion
There is increasing experience with transverse sinus stenting as an alternative to CSF diversion for the treatment of medically refractory IIH. This treatment approach is based on the theory that venous hypertension is one of the primary pathomechanisms for IIH,8 as well as the observed high frequency of venous stenosis in these patients.9 Extant case series have reported excellent efficacy and safety for endovascular venous stenting, suggesting that transverse sinus stenting may be a treatment option after weight loss and medical therapy have been exhausted. However, failure of treatment has been reported (table 3), and may be associated with ‘juxta-stent’ narrowing. The nature of these narrowings is probably different from in-stent stenosis described in arterial intracranial stent literature,24 which is typically due to neointimal hyperplasia. In all patients retreated in this series there was a proximal juxta-stent narrowing, separate from the narrowing treated with stent placement. Given the position outside of the stent and the fact that these segments are easily distensible by balloon or a new stent, these re-narrowings are likely to be a result of extrinsic compression similar to the lesions described in figure 1A (a long narrowed segment of the transverse sinus on catheter venography) of the case series presented by Ahmed et al.16
This finding does not resolve the ‘chicken or egg problem’ that is often raised regarding IIH and accompanying venous stenosis,11 ,25 ,26 but it is the opinion of the authors that juxta-stent narrowings point to the dynamic nature of venous caliber and the pressure in the intracranial environment. Indeed, rather than chicken or egg, there are likely subpopulations where the key factor for IIH is central venous hypertension, others where it is local intracranial venous hypertension due to an endoluminal defect such as thrombus or an arachnoid granulation either in both transverse sinus or on the dominant side with hypoplastic contralateral side, and still others where it is a combination of any or all of the above factors resulting in the altered homeostasis of elevated CSF pressure.
There is no consensus for the management of symptomatic post-stent, juxta-stent narrowing with renewed papilledema. Revisions with additional stenting may be an option as well as CSF diversion, but optimal management is undefined. The identification of patients who are likely to develop symptomatic juxta-stent narrowing and require additional treatment may be helpful in the selection of patients with IIH for venous stenting.
In this series two factors demonstrated statistical significance: race and BMI. The data on race should be viewed with the caveat that only five patients of African-American descent were included in the study and all required additional treatment. Larger populations of African-American patients with IIH should be assessed before concluding that this finding holds true for the general population. Multivariable analysis was not possible given the small size of the dataset, therefore adjusting for patient BMI was not feasible. It should also be noted that the mean BMI of these five patients was 47.0 kg/m2 (range 37–67 kg/m2), which was higher than the overall sample mean of 38.7 kg/m2. It is possible that, with correction for BMI in multivariable analysis, the effect of race may disappear.
Otherwise, BMI was a statistically significant predictor for recurrent symptoms after venous stenting. The percentage of patients with a BMI >30 kg/m2 was larger in the present series than in previous series where proportionality was described. Thus, we maintain that larger series would be useful to assess these data for representativeness for the population at large. There may be a BMI value that predicts IIH that is refractory to stenting.
Venous hypertension and CSF resorption
Intrinsic narrowing, such as from an arachnoid granulation or thrombus, has been described in contrast to the Starling type extrinsic narrowing thought to result from raised ICP, which introduces uncertainty as to whether either or both types of lesions can be treated with transverse sinus stenting. Both types have been included in the series described by Ahmed et al,16 with reportedly good results. Unsurprisingly, relief of elevated ICP by CSF diversion results in reduction in transverse sinus narrowing in some of these patients.27 ,28
Despite the apparent efficacy of treatments targeting venous hypertension in improving CSF hypertension, the actual mechanism in which venous hypertension and venous outflow obstruction results in intracranial hypertension remains uncertain. In 1978, Marmarou et al 29 proposed a model describing CSF production, storage and resorption, which assumed that CSF drains into the sinuses into the jugular veins. The precise pathway that CSF enters the venous system is also unclear, and it is possible that some (if not much) of that flow is mediated by perivascular aquaporin 4-mediated transport mechanisms implicated in so-called ‘glymphatic drainage’.30 Based on work by Bateman et al, 31 resistors to resorption, such as in narrowed compressible transverse sinuses, may be modified by cerebral blood flow. These Starling type resistor models may explain why transient extrinsic compression may result in a feedback loop that leads to continuous elevated intracranial hypertension even when an inciting event ends.31
Venous outflow obstruction, venous hypertension, and elevated ICPs have also been described in association with venous thrombosis12 ,32 as well as dural fistulas.14 These may support a venous pressure mechanism for IIH pathology.
BMI and venous hypertension
BMI is a commonly used derived value calculated by dividing body mass by the square of body height, expressed in units of kg/m2, and has been used to assess risk for various disease states including cardiovascular disease. Obesity is typically defined as BMI >30 kg/m2. Sugerman et al 1 have shown that increased BMI results in increased intrathoracic and intra-abdominal pressures, which likely results in impaired venous return into the chest. If venous hypertension is a unifying mechanism for IIH,8 and high BMI may contribute to systemic venous hypertension, then it follows that particularly high BMI may result in impaired venous return from the brain and intracranial contents, with or without a transverse sinus narrowing. As CSF is retained, the venous sinus compression described by Bateman et al 31 may potentiate further elevation in venous pressures via the Starling resistor effect.
BMI, however, may not be the best index for assessing intrathoracic pressure as mass distribution may vary.33 Nutritional circles continue to investigate indices that best describe health risk,34 and it may follow that BMI does not adequately predict intrathoracic pressure for an individual.
Study limitations
This study was primarily limited by the small number of cases and retrospective analysis of the prospectively collected data.
Conclusion
In this small study, BMI was a significant predictor for symptomatic juxta-stent recurrence after transverse sinus stenting for IIH. There were no retreatments below a BMI of 35 kg/m2 (class 0 and I obesity) and 40% and 46.2% retreatments above a BMI of 35 kg/m2 (class II and III obesity, respectively). Race was also a statistically significant predictor, but the number of African-Americans in this study was small and the results regarding race should be interpreted with caution. Torcular pressure before and after stenting as well as the residual gradient were not significant predictors, nor was post-stenting internal jugular pressure. Further studies to evaluate which patient subgroup will benefit most from endovascular dural sinus stent placement are indicated.
Acknowledgments
The authors extend their gratitude to Lydia Gregg, Assistant Professor & Medical Illustrator at the Johns Hopkins University School of Medicine, for preparing the illustration.
References
Footnotes
Contributors Each author made a material contribution to the article, its revision, and the final approval of the article for submission.
Competing interests None declared.
Ethics approval Ethics approval was obtained from Cleveland Clinic Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.