Article Text

Summary
Operators commonly encounter difficulty maneuvering a microcatheter beyond the distal lip of wide neck aneurysms and aneurysms in challenging locations. Few techniques have been described to guide operators in these particular situations. In this case report of a 56-year-old woman with a 16 mm ophthalmic artery aneurysm, the microcatheter continually snagged the distal aneurysm lip, preventing delivery of a flow diverter into the distal parent vessel. In troubleshooting this obstacle, a second microguidewire was introduced alongside the microcatheter and was used to cover the distal lip of the aneurysm to prevent further snagging. The second guidewire successfully deflected the microcatheter into the distal vessel, a technique that we have aptly dubbed the ‘bumper technique’.
- Aneurysm
- Angiography
- Catheter
- Flow Diverter
- Technique
Statistics from Altmetric.com
Background
The development of novel endovascular devices and techniques has greatly increased the range of aneurysms treatable by endovascular methods. With the development of balloon assisted coiling, stent assisted coiling, and flow diversion, wide neck and large aneurysms in difficult locations become possible to treat, but pose novel challenges to the operator. One such challenge is the task of maneuvering a large bore microcatheter, such as the Excelsior XT-27 (Stryker, Fremont, California, USA) or the Marksman (Covidien, Irvine, California, USA), past the distal lip of an aneurysm in order to unsheathe a stent or flow diverter. Here we describe a novel technique to approach this challenge using a second microguidewire to act as a bumper to deflect the microcatheter beyond the distal aneurysm lip.
Case presentation
The patient was a 56-year-old woman who underwent non-invasive imaging to work up chronic headaches, and jaw and neck pain. MRI imaging demonstrated a large left internal carotid artery aneurysm measuring 16×14 mm. Diagnostic angiography was performed that clearly showed a narrow neck 16 mm ophthalmic artery aneurysm (figure 1A). The patient was selected for aneurysm coil embolization with flow diversion. Coil embolization, in addition to flow diversion, was chosen to induce early complete occlusion and avoid the risk of post-procedural aneurysm rupture.1 ,2 A guide catheter was advanced over a Synchro 2 (Stryker) microguidewire into the distal cervical internal carotid artery. An XT-27 microcatheter was advanced over the Synchro 2 into the aneurysm and two long coils were injected (figure 1B).

(A) Diagnostic angiography demonstrating a large 16 mm narrow neck aneurysm arising from the left ophthalmic artery prior to treatment. (B) Angiography following coiling of the aneurysm. (C) To facilitate placement of a pipeline stent, advancement of the microcatheter past the neck of the aneurysm was attempted but initially not possible. The microcatheter repeatedly became caught on the distal lip of the aneurysm. (D) A second microwire was introduced adjacent to the first and positioned to cover the distal lip of the aneurysm. Acting as a bumper, the second microwire was used to successfully guide the microcatheter overlying the first microwire past the distal aneurysm lip. (E) The microguidewire was successfully advanced beyond the distal aneurysm lip and the second ‘bumper’ microguidewire was retracted. (F) Fluoroscopy following deployment of the flow diverter demonstrating completed treatment of the aneurysm.
The Synchro 2 was then advanced past the neck of the aneurysm to guide the XT-27 into the distal vessel for delivery of the pipeline flex embolization device. The Synchro 2 advanced into the distal internal carotid artery with some maneuvering, but the XT-27 repeatedly caught on the distal lip of the aneurysm neck, despite its narrow dimensions. Although the aneurysm neck was narrow, the morphology of the aneurysm relative to the parent vessel was such that the aneurysm was located on the outside edge of a long curve and therefore the microcatheter was unable to negotiate the turn. The aneurysm location was likely the dominant contributor to the problem in this particular case. In an attempt to address the difficulty, the Synchro 2 was exchanged for a Fathom 16 (Boston Scientific, Marlborough, Massachusetts, USA) microguidewire, which also advanced past the aneurysm without difficulty, but the XT-27 again became caught on the distal lip of the aneurysm (figure 1C).
The Synchro 2, already available on the back table, was brought up in the guide catheter alongside the XT-27. The Synchro 2 was advanced past the aneurysm and permitted to rest on the distal aneurysm lip (figure 1D). The XT-27 was again advanced distally, deflected off the Synchro 2, and easily passed beyond the distal lip of the aneurysm neck for deployment of the pipeline flex embolization device (figure 1E, F).
Outcome and follow-up
The patient was successfully extubated postoperatively, brought to the intensive care unit, and discharged home the following day without complications, at her neurological baseline.
Discussion
Difficulty positioning the microcatheter beyond an aneurysm neck commonly arises when performing stent assisted aneurysm coiling or during placement of a flow diverter because these situations require a larger bore microcatheter. Aneurysm morphology becomes more challenging when the aneurysm neck is wider and the aneurysm is located on the outside of a sharp turn or at a bifurcation, such as the basilar artery, middle cerebral artery bifurcation, or the ophthalmic artery. The case presented describes a patient with a narrow neck aneurysm located in a challenging area of vasculature. A wide neck would have likely compounded the navigation difficulty. Whether the cause of difficulty is a wide neck or challenging location, the inability to navigate beyond these challenging segments can result in the need to abandon the preferred treatment approach or change the components of the coaxial system.
Microcatheter bore size is an important factor to consider when attempting to maneuver beyond the distal lip of an aneurysm. The XT-27 and Marksman microcatheters are often used to deliver intracranial stents used in stent assisted coiling as well as the pipeline embolization device. These catheters have a 0.027 inch inner diameter, which has a large step off when used with common microguidewires, such as the Synchro 2 Standard or Fathom 16, as described in this case example. One solution would be to begin with a smaller microcatheter with less of a step off, such as the XT-17 with a 0.014 inch microguidewire. After this system is past the aneurysm, however, it would need to be exchanged for a larger bore microcatheter capable of delivering the device of interest.
A second option is to loop the wire and microcatheter in the aneurysm to approach the distal parent vessel more directly. Wang et al3 described a strategy in which the microcatheter is looped within the aneurysm and tension is pulled on the microcatheter with the wire at various positions within the looped segment to straighten the microcatheter. Reported variations on this include use of a balloon or stent, partially or fully deployed, in the distal parent vessel to anchor and straighten the microcatheter and wire in the aneurysm after distal access is obtained.4 ,5 There is likely to be some risk to this technique given that the wire and microcatheter must travel along the wall of the aneurysm. This looping technique is not possible if an aneurysm has already been treated or if the aneurysm is treated with coils early in the procedure, as in the case presented above.
Another solution, suggested by Adrianto et al, called the parallel wire technique, is to use two microguidewires within the microcatheter. In the description of their technique, the authors postulated that the combination of two microguidewires, with purchase beyond the aneurysm neck, acts to straighten the microcatheter in relation to the branching vessel and guide it more effectively past the distal lip.6 This technique provides an adequate solution in many cases, but requires the operator to use two microguidewires that will both fit within a 0.027 microcatheter.
Others have reported similar techniques that utilize a ‘buddy wire’ for parallel use within a guide catheter to provide proximal stability to the microcatheter or the guide catheter itself while navigating tortuous regions of the internal carotid artery.7 ,8 However, these techniques do not focus on navigation of the distal aneurysm lip.
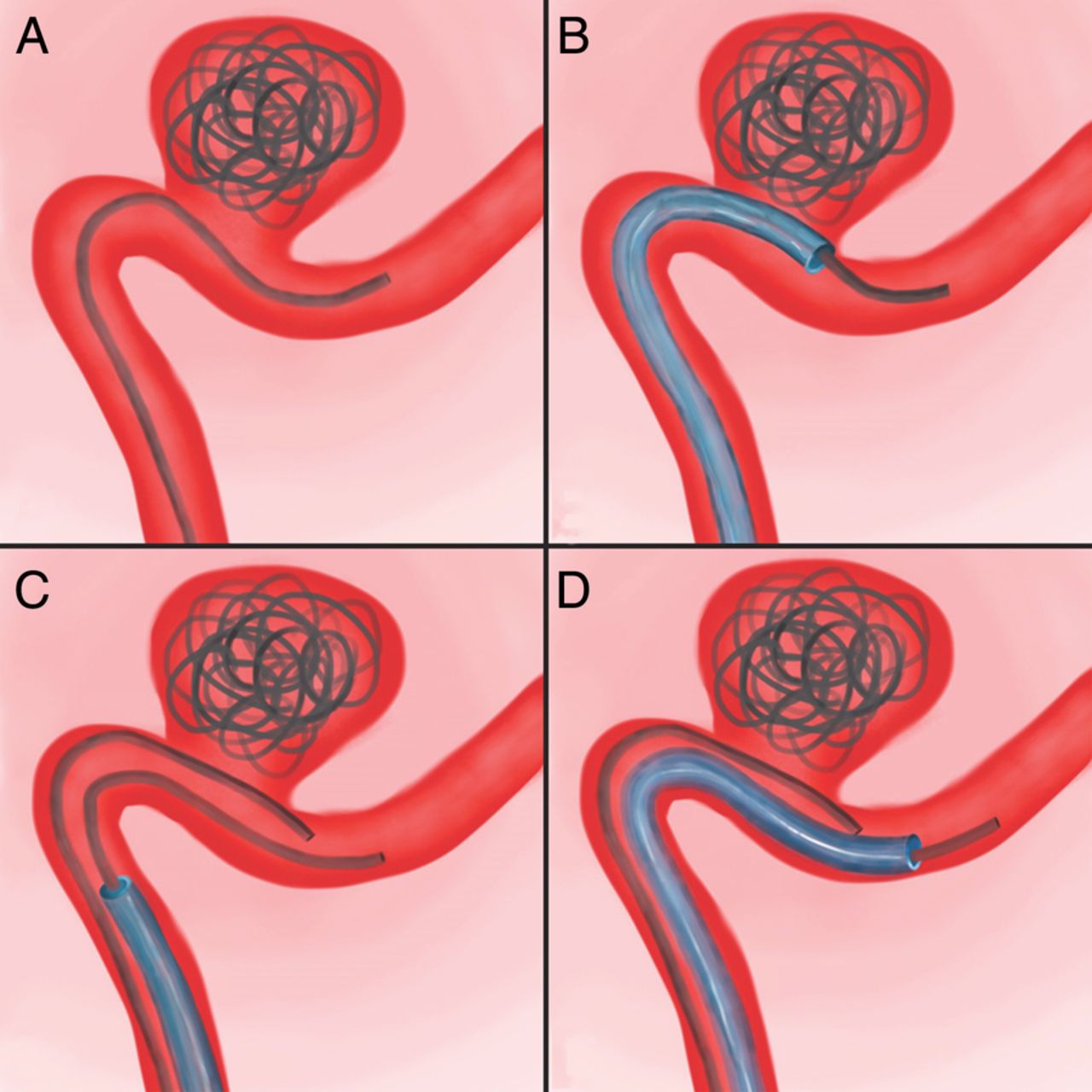
In the bumper technique, in contrast with the Adrianto et al parallel wire technique, a second microguidewire is introduced alongside the microcatheter, rather than within it. As such, the second microguidewire does not act to straighten the microcatheter in relation to the parent vessel, as it is thought to do in the parallel wire technique. Rather, in the bumper technique, the second microguidewire is positioned such that it rests on the distal lip, acting as a bumper to shield the microcatheter from the step off and prevent any further snagging (figure 2). With the microguidewire bumper set in place, the microcatheter is easily deflected into the distal parent vessel. The bumper technique is elegant in its simplicity in that it does not require passage into the aneurysm and can be performed with commonly used microguidewires. As it may be challenging to reproduce, it is likely valuable as a bailout option rather than as a firstline technique. It may be a handy technique for cases in which aneurysms have a distal lip that is difficult to overcome and may add a useful tool to the neurointerventionalist's armamentarium in these scenarios.

{kind=link}
{kind=link}
(A) The microguidewire is positioned beyond the aneurysm lip. (B) Due to the aneurysm position and morphology, the microcatheter became caught on the distal aneurysm lip and was unable to be advanced. (C) A second microguidewire was positioned such that it rested on the distal aneurysm lip. (D) The second microguidewire acted as a bumper, deflecting the microcatheter into the distal parent vessel.
Acknowledgments
This paper was supported in part by a grant from Arminio and Lucyna Fraga. We would like to thank Sophie Greenberg for providing illustrations of the bumper technique.
Footnotes
Twitter Follow Christopher Kellner @chriskellnerMD
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.