Article Text

Abstract
Aims To report outcomes with selective intra-arterial chemotherapy (SIAC) using simultaneous carboplatin, topotecan, and melphalan for advanced intraocular retinoblastoma.
Methods A retrospective chart review was conducted of patients who received three-drug (melphalan, topotecan, and carboplatin) SIAC during 2006–2011.
Results Twenty-six eyes of 25 patients received the three-drug chemotherapy for treatment of advanced retinoblastoma. Reese-Ellsworth group was 5b in 21 eyes, 5a in 2, 4a in 2, and 3a in 1. Seventeen patients (68%) had recurrence after prior intravenous chemotherapy with or without radiotherapy. In the three-drug therapy, dose ranges were 2.5–7.5 mg for melphalan, 0.3–0.6 mg for topotecan, and 25–50 mg for carboplatin, and median infusions per eye was 2 (range 1–4). At a mean follow-up of 14 months (range 1–43 months), all patients are alive and no patient developed metastatic disease. Twenty-three of 26 eyes (88%) survived. Eleven of the 26 eyes (35%) developed recurrent disease and were treated with enucleation (n=3) or with focal therapy (n=8) with or without plaque brachytherapy (n=3). The Kaplan-Meier estimate of ocular survival at 24 months was 75% (95% CI). Electroretinogram showed improvement greater than 25 µV in 4 eyes (15%), loss greater than 25 µV in 12 eyes (46%), and no change greater than 25 µV in 10 eyes (39%).
Conclusions Three-drug SIAC has been used successfully to rescue eyes after treatment failure of intravenous chemotherapy and/or single- or double-agent SIAC. Twenty-three of 26 eyes avoided both enucleation and external beam radiotherapy and retained electroretinogram function.
- Retina
Statistics from Altmetric.com
Introduction
Selective intra-arterial chemotherapy (SIAC), sometimes termed ‘chemosurgery’, is an accepted technique for treating intraocular retinoblastoma.1–8 SIAC with single-agent melphalan has produced remarkable success. Munier et al6 reported success in eye salvage of 85% in their initial cohort and similar findings have been reported by other centres.5–7 The success of melphalan monotherapy SIAC is speculated to be related to the high intraocular concentrations obtained with this technique. SIAC has been accomplished with acceptable systemic toxicity and tolerable local ophthalmic toxicity. In our hands, systemic toxicity in treated children with advanced intraocular retinoblastoma was most frequently asymptomatic Grade III neutropenia and was related to the total dose of melphalan given.4
Intravenous chemotherapy (IVC) for retinoblastoma and other cancers commonly employs multiple agents with different mechanisms or targets designed to work synergistically and prevent resistance. In contrast, SIAC has been successful using a single agent in as few as one dose. However, single-agent SIAC is not successful in all patients, and systemic toxicity limits the dose that can be applied to an eye, especially in patients with bilateral retinoblastoma. In an attempt to minimise systemic toxicity and expand efficacy, we have given multiple agents intra-arterially. Topotecan and carboplatin were chosen for a three-drug combination with melphalan because they have been used successfully as single agents to treat both intraocular and metastatic retinoblastoma.9 ,10 Here we report our experience using the three-drug combination given intra-arterially for advanced cases of intraocular retinoblastoma.
Materials and methods
After approval by the Memorial Sloan-Kettering Cancer Center Institutional Review Board, a retrospective chart review was performed of patients receiving three-drug (melphalan, topotecan, and carboplatin) SIAC. All eyes receiving at least one session of three-drug SIAC between May 2006 and June 2011 were included in this review; the study set consisted of 26 eyes of 25 patients. Initially, we reserved this triple therapy for cases that had proven refractory to IVC or external beam radiotherapy and single- or double-agent SIAC in an attempt to rescue these eyes. Sixteen of the 25 children (64%) had bilateral disease and were monocular or had macular tumours in their opposite eye. After some of the initial favourable responses, we extended its use for primary treatment of eyes with diffuse vitreous disease, because these eyes were less likely to have a complete response with IVC or single- or double-agent SIAC.
Selective delivery of chemotherapy in the eyes of children with retinoblastoma was performed as previously described.1 ,3 ,4 Each of the chemotherapy drugs was diluted with saline in a 10-ml solution and injected in a pulsatile fashion consecutively over 10 min for a total infusion time of 30 min. Doses (table 1) were adapted from standard dose according to clinical results and toxicity as assessed by electroretinogram (ERG). Follow-up examinations under anaesthesia were performed every 3–4 weeks to assess tumour response, and fluorescein angiograms were not routinely performed. Retinal function was assessed using a modified International Society for Clinical Electrophysiology of Vision standard ERG protocol, as described previously.11 We report only the amplitudes of the responses to 30-Hz flicker, as all the ERG response parameters were highly correlated, and the response to 30-Hz flicker is the most easily distinguishable from noise, especially in cases of significant response attenuation.
Standard drug dosages used according to age
Eye survival was defined as eyes salvaged without enucleation or external beam radiotherapy.
Results
The characteristics of the patients and the treated eyes are presented in table 2. Seventeen (68%) of the patients had treatment failure (disease recurrence) after prior IVC and/or radiotherapy. Of these 17, 14 patients had IVC, two IVC and external beam radiotherapy, and one IVC and plaque brachytherapy. All 17 of these patients (18 eyes) also had prior one- or two-drug SIAC. The remaining eight patients received three-drug SIAC as primary treatment.
Characteristics of patients and eyes treated
There were a total of 61 three-drug (melphalan, carboplatin, and topotecan) infusion sessions. The mean number of three-drug sessions per eye was 2.3 (range 1–4). The 18 eyes (72%) that had three-drug sessions after failure of one- or two-drug SIAC received a mean of 2.5 sessions of three-drug treatment, with a mean of 6.3 total sessions of SIAC. The eight eyes that had three-drug sessions as their primary SIAC received an average of 1.8 sessions per patient. The ophthalmic artery was used in 45 of the 61 infusions, the middle meningeal artery in 11, and the balloon catheter in the remaining 5.
Standard drug dose was dependent on patient's age as shown in table 1. Dose was adjusted from the standard dose as previously described4 based on clinical and anatomical factors and ranged from 2.0 to 7.5 mg for melphalan, 0.2 to 0.5 mg for topotecan, and 20 to 50 mg for carboplatin.
There were no procedure-related vascular complications, and catheterisation was successful in all patients. There were no seizures, strokes, or hospitalisations after the procedure. Eleven of the 25 patients (44%) had no systemic toxicity. Of 61 total SIAC sessions, toxicity data was available on 43 sessions; 16/43 (37%) were followed by grade III haematologic toxicity. Ten sessions (23%) were followed by grade IV toxicity, but no patients required a transfusion.
Five patients (20%) required no supplemental antitumor therapy. Among the 20 patients treated with supplemental therapy, all received either diode laser therapy or cryotherapy or both and three required plaque brachytherapy. Plaque brachytherapy was used for a large area of tumour recurrence or treatment of localised seeds.
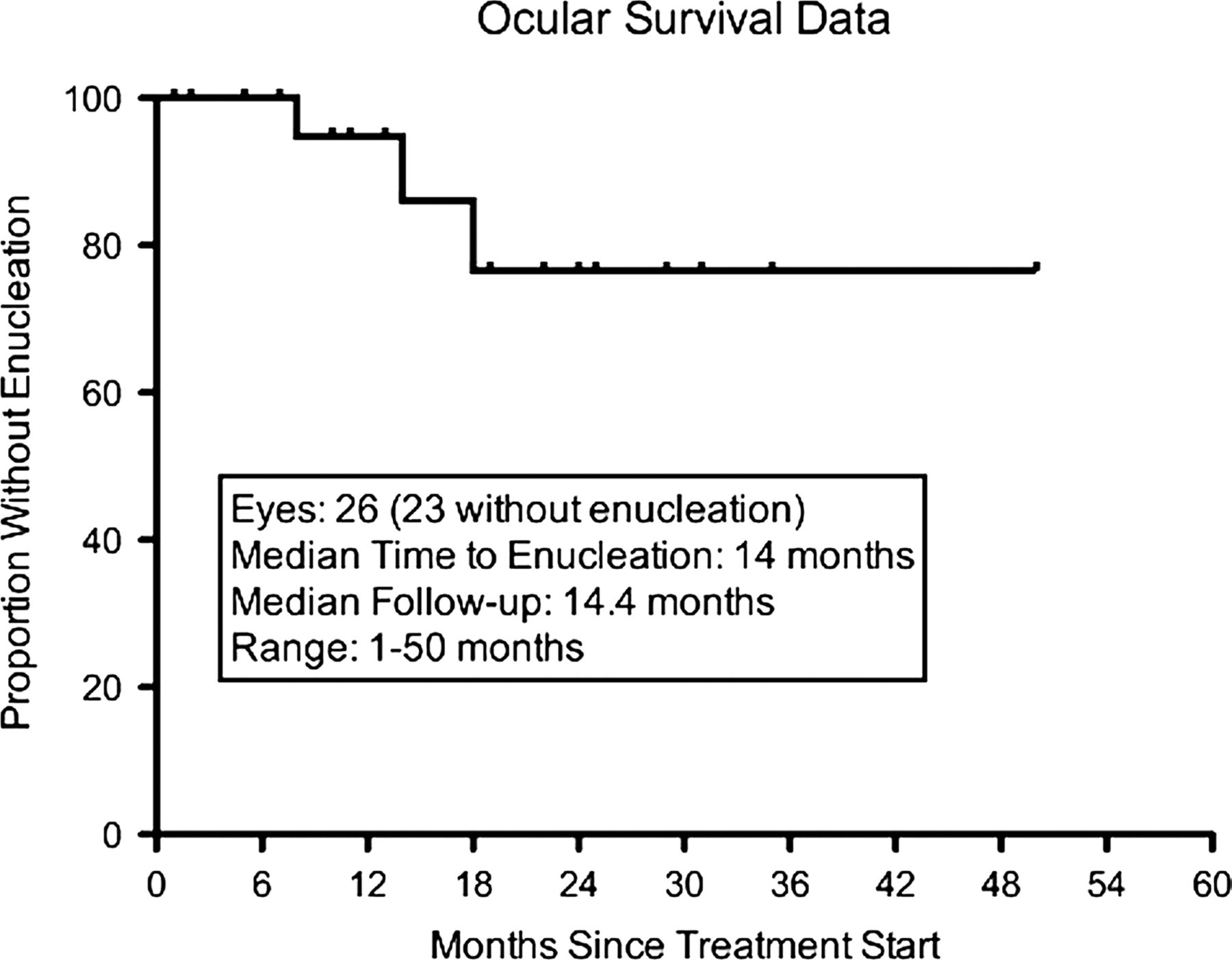
At a mean follow-up of 14 months (range 1–50 months), there have been no cases of metastatic disease, and all patients are alive. Twenty-three eyes (88%) survive. Eleven of the 26 eyes (35%) treated with triple SIAC developed recurrent disease. Of these, 10 were Reese Ellsworth group 5b and 1 was group 5a. Ten were International Classification of Retinoblastoma Group D, and 1 was group E. The non-enucleated eyes required focal therapy (laser or cryotherapy), and three required brachytherapy as well. The mean time from the last triple SIAC to plaque brachytherapy was 4.3 months (range 2–6). The Kaplan-Meier estimate of ocular survival at 24 months is 75% (95% CI; figure 1).

Kaplan-Meier graph of ocular survival.
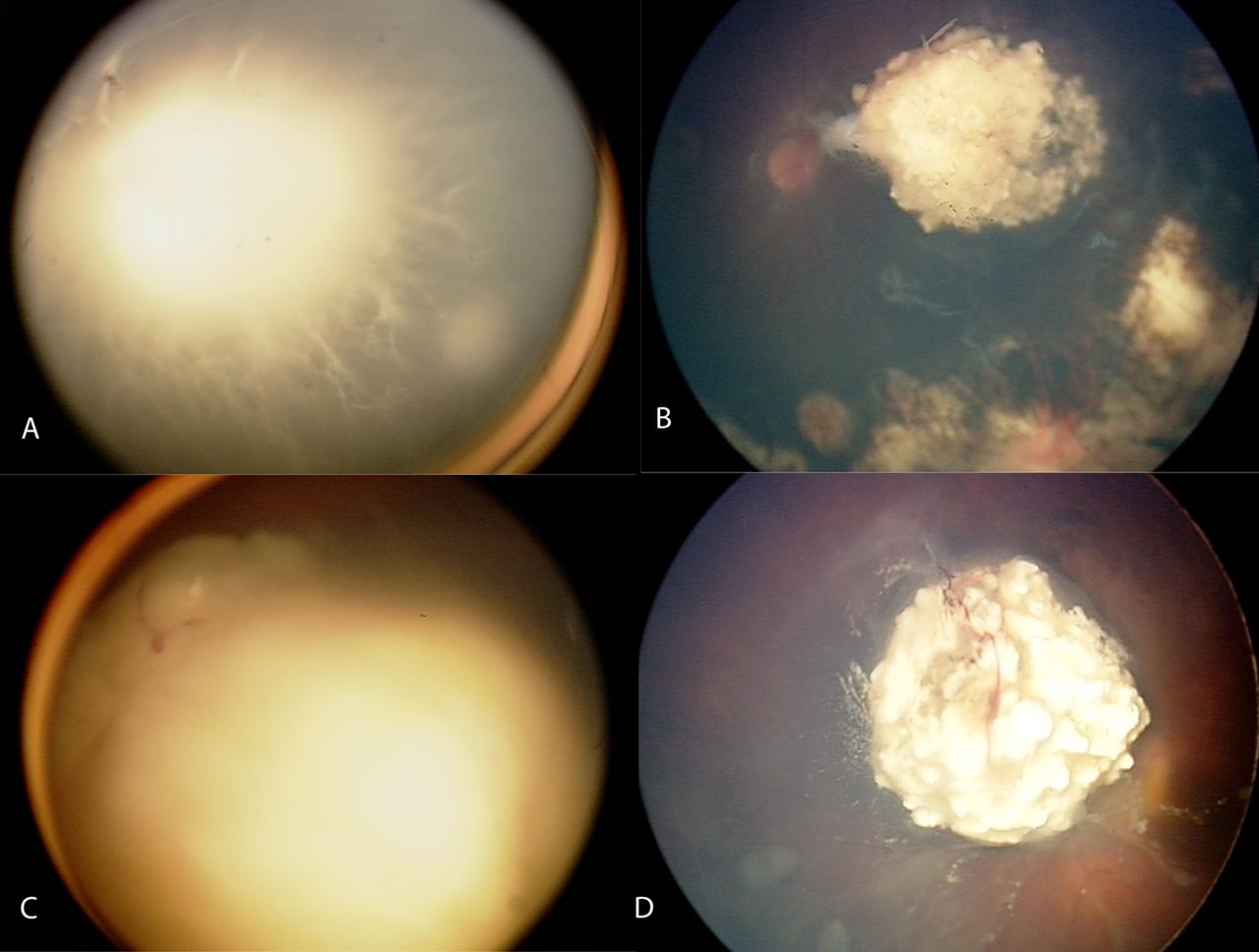
The three eyes enucleated in this series were all removed for recurrent disease (tumour re-growth or recurrent diffuse vitreous seeding) figure 2D. All three were Reese-Ellsworth group 5b and International Classification of Retinoblastoma group D with diffuse vitreous seeding. In one of the enucleated eyes, five cycles of IV chemotherapy had failed, and all three patients had received three or more sessions of single- or double-agent SIAC before triple therapy was given. The mean time to enucleation following the last triple SIAC was 3 months (range 1–4).
{kind=link}
{kind=link}
Fundus photographs of an eye before (A) and after (B) three-drug treatment, showing dramatic shrinkage of tumours and vitreous seeds after 12 months of follow-up. Pre-treatment (C) and post-treatment (D) fundus photographs of an eye in which three-drug selective intra-arterial chemotherapy failed. Note the persistent/recurrent vitreous disease. This figure is only reproduced in colour in the online version.
Compared with initial pre-triple SIAC measurements, 30-Hz ERG responses were improved by at least 25 µV in four eyes (15%), changed by less than 25 µV in 10 eyes (39%), and decreased by at least 25 µV in 12 eyes (46%). For four of the 12 eyes with decreased 30-Hz ERG response, the response remained greater than 75 µV, which most clinical laboratories considered to be within the normal range.
Discussion
SIAC is a valuable technique for treating advanced intraocular disease to preserve the globe and avoid the common systemic complications associated with systemic chemotherapy. Although SIAC with a single agent (melphalan) has produced remarkable success,5 ,6 ,9 it does not succeed in all patients, and the risk of neutropenia limits melphalan doses. To avoid systemic toxicity and maximise intraocular response, we have used SIAC in which melphalan is combined with topotecan and carboplatin.9 ,10 The use of additional chemotherapeutic agents has allowed us to limit each session's total systemic melphalan dose to under 0.4 mg/kg. In this study, we found that the three-drug SIAC can be used to rescue eyes after treatment failure of IVC and/or single- or double-agent SIAC. The majority of eyes retained ERG function, and 88% have avoided enucleation.
Initially, we used this triple therapy only for tumours in the remaining eyes of monocular patients that had proven refractory to IVC or external beam radiotherapy and to single- or double agent SIAC. Later, after some of the initial favourable responses, we expanded its use to primary treatment of eyes with extensive vitreous disease because these eyes were difficult to control with single- or double agent SIAC.
Of the eight eyes with no previous treatment that received only triple-drug SIAC, six (75%) had a decrease in their ERG of greater than 25 µV. However, of those ERGs that deteriorated, three remained greater than 70 µV, which is considered a normal 30-Hz ERG response amplitude in most clinical laboratories. The decreases in ERG may be related in part to toxicity of the multidrug chemotherapy. Clinically, these eyes had no signs of optic nerve pallor or retinal vascular occlusion, and there were no haemorrhages. Some eyes had areas of retinal pigment epithelia changes, especially in areas of previous retinal detachments, though these changes were not distinguishable from those in eyes treated with one- or two-drug SIAC.
In this series, 11 patients had recurrence of disease that was controlled with local therapy, 3 of which required plaque brachytherapy. Three eyes were enucleated for recurrent disease. All three of these eyes had treatment failure after three or more sessions of single- or double-SIAC; one had also had treatment failure after five cycles of IV chemotherapy.
The follow-up time is in this study is limited, and salvage rates may decrease with time. Nevertheless, this initial study demonstrates that three-drug SIAC can be delivered successfully, and that in the majority of cases it is useful in treating advanced disease and eyes in which single- or double-agent SIAC has failed. Its role in treatment requires further investigation with continued follow-up.
References
Footnotes
-
Contributors BPM, design of study, collection of data, and writing of paper; DHA, design of study, supervision, review of manuscript, funding; IJD, design of study, supervision, review of manuscript, data collection; SEB, design of study, critical review of manuscript, data collection; YPG, design of study, collection of data, review of manuscript, data collection.
-
Funding Supported in part by grants from the Fund for Ophthalmic Knowledge, Inc and the Alcon Research Institute.
-
Competing interests None.
-
Ethics approval Institutional Review Board of Memorial Sloan-Kettering Cancer Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance