Article Text

Abstract
Background and objective CT perfusion (CTP) is rapid and accessible for emergency ischaemic stroke diagnosis. The feasibility of introducing CTP and diagnostic accuracy versus non-contrast CT (NCCT) in a tertiary hospital were assessed.
Methods All patients presenting <9 h from stroke onset or with wake-up stroke were eligible for CTP (Siemens 16-slice scanner, 2×24 mm slabs) unless they had estimated glomerular filtration rate (eGFR)<50 ml/min or diabetes with unknown eGFR. NCCT was assessed by a radiologist and stroke neurologist for early ischaemic change and hyperdense arteries. CTP was assessed for prolonged time to peak and reduced cerebral blood flow. Technical adequacy was defined as 2 CTP slabs of sufficient quality to diagnose stroke.
Results Between January 2009 and September 2011, 1152 ischaemic stroke patients were admitted, 475 (41%) were <9 h/wake-up onset. Of these, 276 (58%) had CTP. Reasons for not performing CTP were diabetes with unknown eGFR (48 (10%)), known kidney disease (36 (8%)), established infarct on NCCT (27 (6%)), posterior circulation syndrome (25 (5%)) and patient motion/instability (16 (3%)). Clinician discretion excluded a further 47 (10%). CTP was more frequently diagnostic than NCCT (80% vs 50%, p<0.001). Non-diagnostic CTP was due to lacunar infarction (28 (10%)), infarct outside slab coverage (21 (8%)), technical failure (4 (1%)) and reperfusion (2 (0.7%)). Normal CTP in 86/87 patients with stroke mimics supported withholding tissue plasminogen activator. CTP technical adequacy improved from 56% to 86% (p<0.001) after the first 6 months. Median time for NCCT/CTP/arch-vertex CT angiogram (including processing and interpretation) was 12 min. No clinically significant contrast nephropathy occurred.
Conclusions CTP in suspected stroke is widely applicable, rapid and increases diagnostic confidence.
- Stroke
- Cerebrovascular Disease
Statistics from Altmetric.com
Introduction
Brain imaging with multimodal CT has great potential to provide pathophysiological information in acute ischaemic stroke that may be relevant to treatment decisions. There are substantial advantages over MRI in availability of CT scanners in emergency departments and in speed of imaging. Additionally there are fewer contraindications, such as metallic implants, which can be difficult to assess in acute stroke patients. However, CT perfusion (CTP) remains a relatively unfamiliar technique to many radiographers and there remain some patients with poor renal function or contrast allergy who are unable to undergo CTP. Additionally, there has been concern that adding CTP to the diagnostic work-up may unnecessarily delay thrombolysis.1 ,2
Previous studies have demonstrated increased diagnostic sensitivity using CTP compared with non-contrast CT (NCCT).2–4 One study of 65 patients using diffusion MRI as the reference standard found a sensitivity of 26% for NCCT and 65% for CTP within the first 3 h after stroke onset. Subsequently, qualitative diagnostic confidence was examined in a consecutive series of 191 patients.5 At a confidence level of ‘probable stroke’, NCCT had a sensitivity of around 50% compared to 70% when CTP was also considered. It was calculated that CTP was 13 times more likely to confirm stroke diagnosis. Other studies have examined a more extended time window up to 12 h when NCCT has a higher sensitivity.6 The observed pitfalls with CTP have included incomplete brain coverage and difficulty identifying lacunar infarcts.
Despite the proven benefits of tissue plasminogen activator (tPA), thrombolysis remains underutilised. Some of the relative contraindications that were derived from the pivotal trials such as ‘seizure at onset’ were designed chiefly to avoid inclusion of stroke mimics into the trials. Patients with so-called ‘mild stroke’ are often not felt to warrant thrombolysis but are at risk of poor outcome in up to 30% of cases.7 ,8
We prospectively investigated the feasibility and technical success of CTP as it was introduced in a tertiary hospital and explored the impact on diagnostic confidence and management in a large series of consecutive patients with acute ischaemic stroke and mimics. The aim was to improve stroke diagnosis and expand thrombolysis by reducing treatment uncertainty regarding stroke mimics and mild/improving stroke.
Methods
Patients
Routine CTP as part of multimodal CT (NCCT brain, CTP, CT angiogram (CTA)) was introduced at the Royal Melbourne Hospital in January 2009. All patients presenting with stroke symptoms within 9 h of onset or wake-up stroke were potentially eligible for multimodal CT regardless of time of day. This time window was chosen due to the availability of several clinical trials and open label intra-arterial interventions in our centre. Patients were clinically assessed by the stroke team prior to choice of imaging protocol which prevented many patients with obvious alternative diagnoses from receiving multimodal CT. Patients were excluded if they had known allergy to iodinated contrast, known renal dysfunction with estimated glomerular filtration rate (eGFR)<50 ml/min (modification of diet in renal disease formula, arbitrary institutional threshold) or unknown renal function in patients with a history of diabetes. These renal function criteria were deliberately conservative given the large (150 ml) contrast dose. Patients were also excluded if agitation led to significant motion degradation of the NCCT or if they were medically unstable.
Multi-modal CT acquisition
Standard NCCT was acquired (4.5 mm slices) followed by CTP using a Siemens Somatom 16-slice multidetector scanner (Siemens, Erlangen, Germany). Two separate acquisitions were obtained, each formatted as 2×12 mm thick slices. Images were obtained every 1 s for 40 s after an initial 4 s delay. In patients with poor cardiac output, the second CTP slab could be delayed further based on the timing of the first slab at the discretion of the attending doctor. Contrast was injected (40 ml at 8 ml/s) into an 18 g intravenous cannula located in the cubital fossa whenever possible. A small number of patients had a 20 g intravenous cannula (contrast injection reduced to 30 ml at 6 ml/s) or more distal cannulae. Following CTP, a CTA was obtained using 70 ml contrast at 5 ml/s with timing based on the peak enhancement of the CTP acquisition. Perfusion maps (time to peak (TTP), cerebral blood flow (CBF), cerebral blood volume (CBV)) were produced using the Siemens on-console software (Siemens Syngo NeuroPCT, Siemens). This software calculates CBF using the ‘maximum slope’ method—a delay-insensitive algorithm that does not involve deconvolution. Maps were generated and interpreted by the stroke neurologist while the patient was being scanned to avoid delay.
Image analysis
The NCCT and CTA were reported by the radiologist on duty and retrospectively independently reviewed (blinded to CTP/CTA and clinical data) by a stroke neurologist (BC) as a control to examine whether the rate of radiologists reporting subtle NCCT abnormalities might have been increased by the presence of CTP maps. The rate of hyperdense artery signs and early ischaemic change was assessed both from the radiologist's report and by independent stroke neurologist review. The presence of vessel occlusion on CTA was recorded based on the radiologist's report. The CTP maps (CBV, CBF and TTP) were reviewed separately by the stroke neurologist to identify abnormalities diagnostic of acute ischaemic stroke. These maps were not routinely reported on by the radiologists during the period of the study. A technically adequate CTP for the purposes of this study was defined as two slabs of sufficient quality for diagnosis of a perfusion abnormality. All patients had follow-up neuroimaging (CT or MRI). The reference standard for diagnosis of ischaemic stroke was the discharge diagnosis (opinion of consultant neurologist based on all available information). Formal assessment of ‘mismatch’ between likely irreversibly injured tissue and potentially salvageable tissue was not performed during the period in which these data were acquired. The time of the scout view (start) and CTA (finish) were recorded to calculate scan duration. Ethical approval for the study was obtained from the Melbourne Health Human Research Ethics Committee, Melbourne, Australia.
Statistical analysis was performed using Minitab V.16. Mild stroke was defined as National Institutes of Health Stroke Scale (NIHSS) ≤79 for a pre-specified subgroup analysis. Fisher's exact test was used for dichotomous comparisons, the Wilcoxon test for continuous variables and κ for inter-rater agreement.
Results
A total of 1152 patients presented to the Royal Melbourne Hospital Emergency Department with acute ischaemic stroke between January 2009 and September 2011; 194 (16.8%) received intravenous tPA. There were 475 patients presenting <9 h from onset or wake-up stroke and therefore potentially eligible for multimodal CT imaging. The majority (468/475, 99%) were notified to the stroke team by the emergency department as a ‘code stroke’ and CTP was performed in 277/475 (58%). The clinical characteristics of patients who did and did not undergo CTP are listed in table 1. Patients who had CTP were significantly younger and presented to hospital earlier. Although patients who had CTP received tPA more often (62% vs 41% of those imaged within 4.5 h of stroke onset, p<0.001), this ceased to be significant in logistic regression after adjustment for baseline NIHSS and premorbid mRS. Despite diabetes with unknown eGFR being an exclusion for CTP, this did not lead to a significant imbalance in the prevalence of diabetes between the two groups.
Clinical characteristics of patients
The reasons for patients not undergoing CTP are listed in table 2. In the first 6 months, the proportion of patients not undergoing CTP due to ‘clinician discretion’ was 13/59 (22%). As familiarity increased, this reduced to 34/416 (8%, p=0.004). Although 48 patients were excluded on the basis of diabetes and unknown creatinine, only 14 actually had eGFR<50 ml/min and none had eGFR<30 ml/min.
Reasons for patients not undergoing CT perfusion imaging
Technical quality
The proportion of patients with CTP slabs deemed adequate to make a positive diagnosis of ischaemic stroke was 228/277 (82%) overall and increased from 15/27 (56%) to 214/250 (86%) after the first 6 months (p<0.001). Four patients had complete acquisition failure for technical reasons (3 contrast injection or timing errors, 1 severe motion leading to no interpretable images), and an additional 45 patients had a significant technical issue (49/277=18%). Of these, 22 patients had only one usable slab (3 severe motion, 2 subcutaneous contrast extravasation, 17 clinician discretion). Motion degradation significantly affected image quality in another 11 patients. Contrast bolus delay led to some degree of truncation of the concentration–time curve in 59/277 (21%) patients but was severe enough to impair image quality in 12 patients. The distribution of reasons for technical errors appeared similar between the first 6 months and subsequent period. Median acquisition time for scout, NCCT, 2 CTP slabs and arch-vertex CTA (including CTP processing and interpretation) was 12 min (IQR 9–16). Median door to needle time was 63 min (IQR 35–86) in 57 tPA patients without CTP and 67 min (IQR 51–87) in 137 with CTP (p=0.15).
Diagnostic sensitivity
The diagnostic sensitivity of NCCT reported as a relevant hyperdense artery or early ischaemic change by the radiologist was 131/277 (47%) in patients who had CTP and 210/475 (44%) overall. Independent retrospective assessment of the NCCT by a stroke neurologist blinded to all clinical and other imaging information was performed to examine whether the availability of CTP maps may have increased the rate of reported early ischaemic changes on NCCT. However, the sensitivity was unchanged: 127/277 (46%) in those who had CTP and 216/475 (45%) overall. Agreement between radiologist and neurologist was substantial (κ=0.85 for NCCT in CTP patients and 0.80 in all patients). Review of discrepant cases revealed a description by the radiologist (often relatively junior) of ‘early ischaemic change’ outside the region of subsequent diffusion MRI abnormality in 10 cases, indicating the difficulties in accurately identifying early ischaemic change. A relevant intra-cranial occlusion was visible on CTA in 117/277 patients. The addition of CTA to NCCT increased the sensitivity to 162/277 (58%, p=0.01; table 3).
Diagnostic sensitivity in patients who underwent the full multimodal CT protocol
The diagnostic sensitivity of CTP (222/277, 80%) was significantly greater than NCCT alone (p<0.001, figure 1) or NCCT+CTA (p<0.001)). There were no cases where CTA provided information that was not readily apparent using CTP alone. The false negative CTP were due to lacunar infarction (28 (10%)), infarct outside CTP slab coverage (21 (8%)), technical failure (4 (1%)) and reperfusion (2 (0.7%)). A sub-analysis restricted to patients imaged within 4.5 h produced similar results, with CTP sensitivity of 83% compared with 50% using NCCT (p<0.001).

{kind=link}
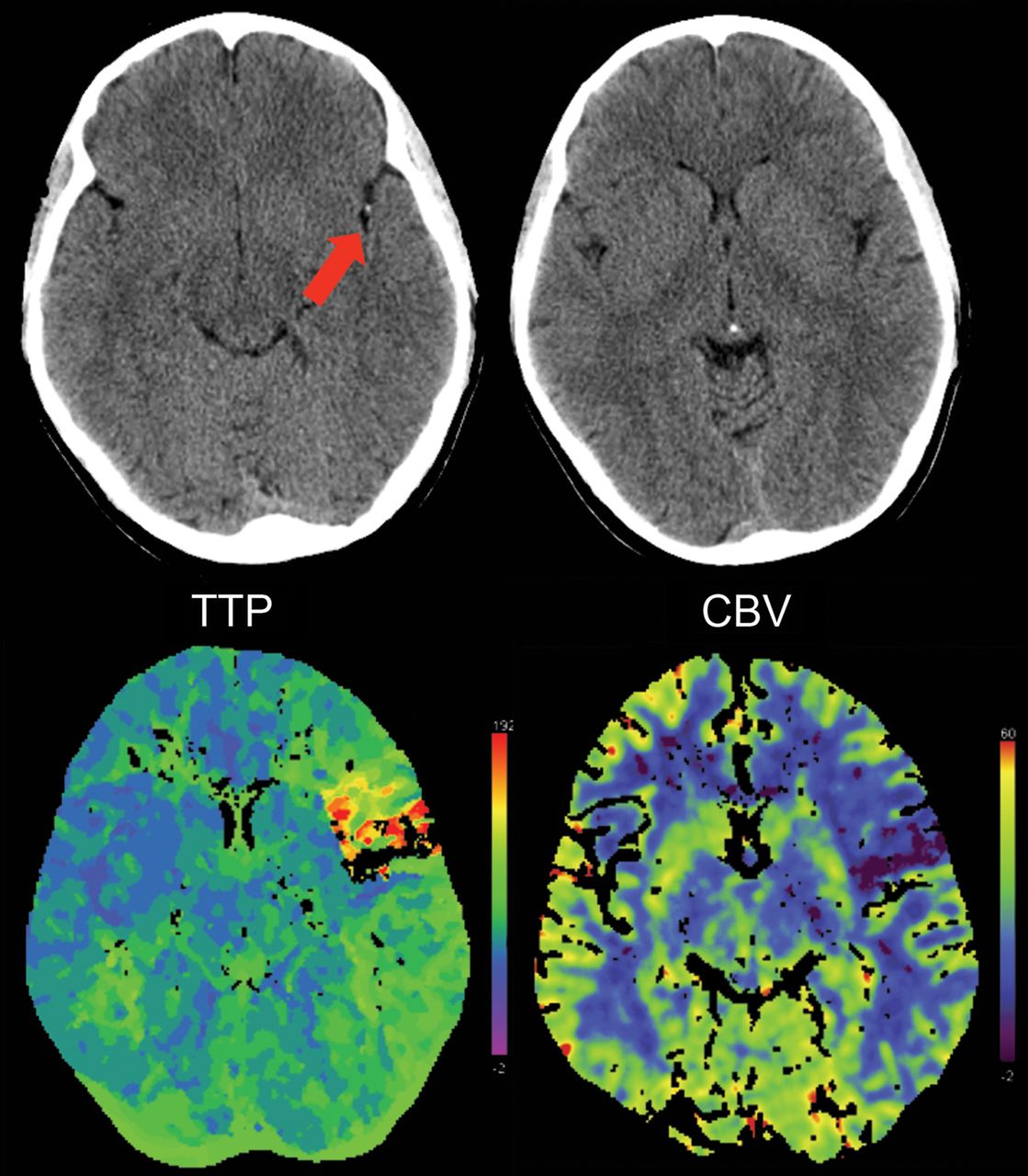
An example of increased diagnostic confidence using CT perfusion. A young patient presented to the emergency department 1.5hr after onset of right arm weakness and speech disturbance. However, the examination features were atypical, eg apparent weakness on examination was inconsistent with use of the affected limb to transfer between stretchers which lead to diagnostic uncertainty. Non-contrast CT demonstrated subtle hyperdense Sylvian ‘dot sign’ (arrow) in a branch of the middle cerebral artery but the CTP abnormality was more obvious. Time to peak (TTP) was delayed in the left frontal region with a smaller region of reduced cerebral blood volume (CBV) confirming an ischaemic stroke and the patient received thrombolysis.
In our series, 115 patients presenting within 4.5 h had ‘mild or improving stroke’ (NIHSS≤7), of whom 57 (50%) received tPA. As expected, the sensitivity of CTP (performed in 73/115, 63%) was lower in these milder patients (50/73, 68%). However the rate of diagnostic abnormalities on NCCT was also lower (22/115, 19%) and the difference remained significant (p<0.001, table 3). Stroke severity was not significantly different between those with and without CTP abnormalities (median NIHSS 5 vs 4, p=0.26). Of those who received tPA, 42 had CTP which confirmed the diagnosis of stroke in 30/42 (71%) patients compared with 10/57 (18%), using NCCT (p<0.001).
There were an additional 87 patients who had CTP on presentation but the final diagnosis was not ischaemic stroke. These represented 5% of the 1589 referrals from emergency doctors with suspected stroke and no haemorrhage on CT, and only 20% of the 437 who had a final diagnosis of a stroke mimic. These were patients with significant neurological signs (and otherwise eligible for thrombolysis) but where there was some clinical suspicion of a stroke mimic which, when combined with normal CTP, became sufficiently convincing to withhold tPA which would otherwise have been given. The final diagnosis was conversion disorder (non-organic) in 31 (36%), migraine with focal neurological deficit in 23 (26%), seizure with Todd's paresis in 15 (17%, including 3 new diagnoses of cerebral tumour), with other miscellaneous diagnoses comprising 21% (exacerbation of old deficit after syncope (5), metabolic derangement (4), systemic sepsis (4), peripheral nerve compression (3), encephalitis (2)). In these patients, NCCT was universally unremarkable. CTP was also normal with the exception of one patient with dysphasia related to migraine. The abnormality in this case was a pan-hemispheric subtle (1–2 s) delay in relative TTP. This is not the typical CTP appearance of a stroke and was not accompanied by vascular occlusion or stenosis. However, the patient was treated with tPA due to relative unfamiliarity with CTP at the time. Subsequent diffusion MRI was normal.
Complications
Subcutaneous contrast extravasation occurred in two patients without long term consequences. No allergic reactions were observed. Renal function was monitored as part of routine care and no clinically significant renal dysfunction was reported.
Discussion
In this, the largest reported series of CTP in suspected stroke, we have shown that CTP is clearly feasible in clinical practice and significantly contributes to diagnostic confidence in both stroke and mimics. The magnitude of the superior sensitivity afforded by CTP presented in this analysis is probably conservative given the often equivocal nature of early ischaemic change on NCCT. Furthermore, it is difficult to quantify the difference between recognition of, for example, loss of insular ribbon on NCCT compared with demonstration of the quality of perfusion throughout the entire middle cerebral artery territory. We were able to obtain this extra information (including processing and interpretation) in a median of 12 min.
There was clear evidence of a ‘learning curve’ over the first 6 months. This is not surprising as more than 40 radiographers rotating through emergency CT were required to become familiar with dynamic perfusion imaging. Although ∼40% of stroke patients did not undergo CTP, the proportion who could not have tolerated the procedure was low (table 2). Posterior circulation stroke was only excluded due to the limited coverage of the CT scanner used, patients with established stroke on NCCT have little to gain from added CTP, and ‘clinician discretion’ included a range of pragmatic considerations such as after-hours scans ordered by the emergency department and completed before arrival of the stroke team and the need to rapidly vacate CT for incoming trauma patients. Once the routine protocol became established, the major reasons for patients not proceeding to CTP related to potential contrast nephropathy risk. Our protocol of excluding patients with eGFR <50 ml/min or diabetics with unknown eGFR was deliberately conservative while introducing this new technique. Although formal monitoring of renal function was not undertaken in this cohort of patients, there were no clinically relevant episodes of renal failure following CTP, even with the large dose (150 ml) administered with this protocol. This is consistent with several previous studies.10–14 Notably, although 24% of the patients excluded from CTP had diabetes with unknown eGFR, only 14/48 had eGFR <50 ml/min and none had eGFR <30 ml/min—the usual threshold below which contrast is contraindicated at our institution. One option to increase access to CTP is point-of-care creatinine measurement. However, our data suggest that unrecognised severe renal disease is uncommon. Furthermore, newer scanners can acquire simultaneous whole brain CTP and dynamic CTA with much lower contrast volume. A recent guideline has recommended that in emergency situations where creatinine is unknown, it is reasonable to proceed with imaging and ensure adequate hydration following the scan.15 This approach has been taken in other institutions with a very low rate of significant renal complications.12–14
Provided the acquisition is technically adequate, CTP has excellent sensitivity for ischaemic stroke. Most false negative cases occurred in lacunar stroke, in patients with complete reperfusion or when the stroke lay outside the slab coverage acquired (eg, some anterior cerebral artery infarcts). Lacunar stroke is also difficult to detect using MR perfusion, with reports in the literature varying from 0% to 68% of diffusion weighted imaging positive patients having a detectable hypoperfused region.16 ,17 Inability to identify regions of reperfused infarction is a potential safety concern. Although distal clot migration and fragmentation of the perfusion lesion is increasingly common as time from onset increases,18 our data suggest that complete reperfusion of the infarcted territory is relatively rare. A fragmented CTP pattern should prompt particularly careful examination of the NCCT for evidence of early ischaemic change that would indicate more extensive infarction than detected by CTP.
The variety of stroke mimics encountered in our series was similar to previously published data.19 Subtle perfusion abnormalities in migraine patients are well recognised, with reduced CBF the most commonly described.20–22 One recent report suggested that TTP asymmetry was the most sensitive parameter23 and matches our experience. It would appear that the frequency of abnormalities (1/23 in our series) is quite low, but this may relate to timing as the majority of reports relate to the aura phase. Apart from the single patient with migraine who received tPA before the significance of migraine CTP abnormalities was appreciated, there were no false positive lesions in stroke mimics.
While detecting an abnormality that proves the presence of a stroke may assist in the decision to treat a patient when there has been a possible seizure or when symptoms are mild or improving, the question arises whether a patient with normal CTP should be excluded from thrombolysis within 4.5 h. Although the chances of missing a treatable large vessel stroke are negligible, lacunar strokes may benefit from tPA. A sub-analysis of National Institute of Neurological Diseases and Stroke (NINDS) trial data suggested that patients with clinically defined lacunar syndrome had similar tPA response to large vessel strokes24 as have other small uncontrolled case series,25 ,26 and the risk of symptomatic haemorrhage appears very low. However, clinical differentiation of true single perforator infarction from striatocapsular infarction due to parent vessel disease is difficult and this may have confounded these analyses. Interestingly, some studies have suggested that those lacunar stroke patients with detectable perfusion abnormalities are at higher risk of clinical deterioration, implying that CTP may have a role in risk stratification.17 ,27 Many stroke mimics also have a very low risk of harm from tPA provided standard bleeding contraindications are observed28 and so any steps to exclude them would need to ensure that treatment is not delayed for the majority of stroke patients.
The related issue of using multimodal CT to limit sub-4.5 h thrombolysis to patients with a favourable perfusion profile has also been debated.1 ,29 Treatment is already proven in this time window based on a normal NCCT. Apart from potential economic savings, the main justification for using imaging selection would be if it were demonstrated to reduce the risk of treatment. Given that symptomatic intracerebral haemorrhage only occurs in ∼2% of current tPA patients,30 ,31 restricting this treatment would seem counter-productive. Although it may be that the majority of benefit occurs in patients with favourable CTP profiles, it is virtually impossible to exclude more minor benefits in patients with a large infarct core or predominantly reperfused infarct. A more positive potential use for CTP is in identifying patients with large vessel occlusions and significant mismatch who have limited prospects of reperfusion with IV tPA but much to gain if reperfusion can be achieved using other approaches. This strategy has been tested in a phase 2 trial which compared tenecteplase to alteplase in patients with a dual target vessel occlusion and mismatch.32 The increased reperfusion with tenecteplase directly translated to a significant improvement in early neurological recovery and functional outcome in this carefully selected population enriched for the presence of salvageable tissue. Dual target CTA/CTP is also the approach to be utilised in the EXTEND-IA trial of intra-arterial clot retrieval after IV tPA (NCT01492725).
A limitation of this analysis was the use of a 16-slice CT scanner with limited spatial brain coverage and acquisition duration. This may increase the generalisability of our results as most institutions have technology of this level or better. However, it probably lead to a lower diagnostic sensitivity as 8% of patients had small lesions that fell entirely outside the available brain coverage. The acquisition duration was limited to 44 s including pre-scan delay, which was frequently insufficient to capture the entire contrast bolus transit in patients with poor cardiac output (21% of our series). Such truncation of the bolus curve leads to underestimated CBV and the potential to overestimate the infarcted region.33 International consensus guidelines recommend a total acquisition length of 70–90 s to avoid these problems.34 Fortunately, most newer scanners have whole brain CTP capacity and more sophisticated acquisition timing that allows variable interval scanning to focus high frequency acquisition during the arterial phase and lower frequency in the washout phase to minimise radiation exposure. In this study we used visual assessment of unthresholded TTP and CBV/CBF maps. This appears adequate for diagnostic purposes. However, this method has limitations if the aim is to assess mismatch.35 The technical quality required to perform an accurate assessment of mismatch is also greater than that required to simply make a positive diagnosis of stroke, and so the finding of adequate quality in 82% would be an overestimate if mismatch assessment was intended. A limitation of this study is that clinician discretion in selecting which patients had CTP strongly influenced the prevalence of stroke and non-stroke in the data and hence we have not attempted to analyse the overall specificity of CTP. The clinical decision to thrombolyse is complex and we were unable to accurately determine how often CTP altered management decisions, particularly as the guideline to treat all patients within 4.5 h with significant clinical deficit and normal NCCT was adhered to.
In conclusion, CTP is a rapid and accurate diagnostic test and, with improvements in technology, promises even greater diagnostic sensitivity with a faster and less complicated acquisition protocol. NCCT remains an important adjunctive investigation and, whenever possible within the 4.5 h treatment window, should be followed by administration of tPA without further delay. However, when there is diagnostic uncertainty or concern that the patient is ‘too mild’ or ‘rapidly improving’, CTP may be of use to add confidence that there is indeed a treatable stroke.
References
Footnotes
-
Contributors BC conceived the study, collected imaging data, performed the analysis and drafted the manuscript. He is guarantor. LW collected clinical data and revised the draft manuscript. HT, PH and BY assisted in data collection and revised the draft manuscript. PD, MP, GD and SD assisted in study design, infrastructure and revised the draft manuscript.
-
Funding BC receives research support from the NHMRC of Australia (postgraduate scholarship 567156, early career fellowship 1035688), the Heart Foundation of Australia, National Stroke Foundation, a Cardiovascular Lipid (CVL) Australia grant and the Neuroscience Foundation of the Royal Melbourne Hospital. Infrastructure support was received for these studies through the Victorian Government Operational Infrastructure Program to the Florey Institute of Neuroscience and Mental Health.
-
Competing interests None.
-
Ethics approval Melbourne Health Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.