Article Text

Abstract
Background and purpose To investigate early clinical surrogates for long-term independency of patients treated with thrombectomy for large vessel occlusion stroke in daily clinical routine.
Methods All patients with anterior circulation stroke enrolled in the German Stroke Registry-Endovascular Treatment from 07/2015 to 04/2018 were analysed. National Institute of Health Stroke Scale (NIHSS) on admission, NIHSS percentage change, NIHSS delta and NIHSS at 24 hours as well as existing binary definitions of early neurological improvement (ENI; improvement of 8 (major ENI)/10 (dramatic ENI) NIHSS points or reaching 0/1 were compared for predicting functional outcome at 90 days using the modified Rankin Scale (mRS). Excellent and favourable outcome were defined as 0–1 and 0–2, respectively.
Results Among 2262 endovasculary treated patients with acute ischaemic anterior circulation stroke, NIHSS at 24 hours had the highest discriminative ability to predict excellent (receiver operator characteristics (ROC)NIHSS 24 hours area under the curve (AUC) 0.86 (0.84–0.88)) and favourable long-term functional outcome (ROCNIHSS 24 hours AUC 0.86 (0.85–0.88)) in comparison to NIHSS percentage change (ROC% change AUC mRS ≤1: 0.81 (0.78–0.83) mRS ≤2: 0.81 (0.79–0.83)), NIHSS delta change (ROCΔ change AUC mRS ≤1: 0.74 (0.72–0.77), mRS ≤2: 0.77 (0.74–0.79)) and NIHSS admission (ROCAdm AUC mRS ≤1: 0.70 (0.68–0.73), mRS ≤2: 0.67 (0.68–0.71)). Advanced age was the only independent predictor (adjusted OR 1.05, 95% CI 1.03 to 1.07, p<0.001) for turning the outcome prognosis from favourable (mRS ≤2) to poor (mRS ≥4) at 90 days.
Conclusion The NIHSS at 24 hours postintervention with a threshold of ≤8 points serves best as a surrogate for long-term functional outcome after thrombectomy for anterior circulation stroke in daily clinical practice. Only advanced age significantly decreases its predictive value.
Statistics from Altmetric.com
Introduction
Various definitions of early neurological improvement (ENI) have been used in the literature to predict long-term favourable outcome after acute ischaemic stroke.1 Even though the relation of ENI and functional outcome is well established it is still matter of current debate what definition of ENI surrogates best long-term functional independence, especially after mechanical thrombectomy (MT) for large vessel occlusion (LVO) stroke. Nevertheless, a considerable percentage of patients still suffer from functional dependency at 90 days follow-up despite achieving ENI after MT.2 Accordingly, treatment effects are not only restricted to technical success of MT with complete reperfusion but also determined by non-influenceable patient characteristics.3 Thus, it remains unclear which factors might impact early clinical improvement predicting functional outcome after endovascular stroke treatment in daily clinical routine outside of large randomised trials.4
The purpose of this study was to investigate early clinical surrogates together with procedure-related and individual characteristics of patients treated with thrombectomy for LVO stroke in a daily clinical routine to better estimate the odds for long-term functional independency and to improve patient selection.
We hypothesised twofold: (1) the National Institute of Health Stroke Scale (NIHSS) serves for a reliable surrogate of long-term functional independency after MT for LVO and (2) procedure-related and individual patient characteristics impact the surrogates and subsequently the outcome prediction.
Methods
Study population
All patients with anterior circulation stroke enrolled in the German Stroke Registry-Endovascular Treatment (GSR-ET) (July 2015 to April 2018; ClinicalTrials.gov Identifier: NCT03356392) were analysed (online supplementary figure 3). The GSR-ET is an ongoing, open label, prospective, multicentre registry of 25 sites in Germany collecting consecutive patients undergoing MT. A detailed description of the GSR-ET study design and the major findings have been published recently.5 6
Supplemental material
Early neurological improvement
Two binary definitions of ENI were applied according to previous studies based on the NIHSS 24 hours after MT: (1) NIHSS improvement ≥8 points from baseline or reaching ≤1 (major ENI (mENI)),7 8 (2) NIHSS improvement ≥10 points from baseline or reaching 0 (dramatic ENI (dENI)).9 10 Based on receiver operator characteristics (ROC) we calculated the cut-off values for absolute NIHSS change (ΔNIHSS) and NIHSS percentage change (%NIHSS: 1-NIHSS 24 hours/NIHSS admission) with the predictive values of highest sensitivity and specificity (Youden Index) for favourable functional outcome (modified Rankin Scale (mRS 0–2)) and excellent functional outcome (mRS 0–1) at 90 days follow-up. Area under the curve values (AUC) and 95% CI together with sensitivity and specificity values of all definitions were compared and stratified by different levels of stroke severity (mild: NIHSS 0–5; moderate: 6–15; severe: ≥16)
Individual and procedure-related characteristics
In a first step, a multivariable logistic regression analysis was performed to identify independent predictors for reaching the cut-off with the highest predictive value for long-term functional outcome in the study cohort. In a second step, a subgroup analysis was performed to identify characteristics that have a significant impact on prediction reversion in patients with poor outcomes (mRS 4–6) at 90 days despite reaching the threshold at 24 hours.
Statistical analysis
Univariable distribution of metric variables is described by median and IQR. For categorical data, absolute and relative frequencies are given. Receiver operating characteristics (ROC) curve analyses and the respective AUC were used to assess the performance of NIHSS admission, NIHSS delta and NIHSS percentage change to discriminate between favourable, excellent and non-favourable of long-term functional outcome. ROC curves were stratified by different stroke severities on admission and subsequently analysed using the DeLongs test11 for AUC value comparison. Thresholds of highest sensitivity and specificity were calculated for each continuous ENI parameter (Youden index).12 Multivariable model building was performed using a stepwise variable selection procedure: first, all factors were fitted together by a stepwise forward selection (inclusion: p value of the score test ≤0.05 and exclusion: p value of the likelihood ratio test >0.1). Then, all resulting significant factors of the model were fitted together with all pairwise interactions in a second block using stepwise backward selection (inclusion: p value of the score test ≤0.05 and exclusion: p value of the likelihood ratio test >0.1).
Given for selected variables are odds ratios with 95% CI and p value of likelihood ratio test. For non-selected variables, p value of score test is displayed. No adjustment for multiple testing was performed, and analyses are regarded as explorative. Local, unadjusted p values <0.05 were considered as statistically noticeable. All data were analysed using the Statistical Package for Social Science (SPSS) software V.25.0 (IBM).
Results
A total of 2262 patients enrolled in the GSR-ET and treated endovasculary for acute ischaemic stroke within the anterior circulation were analysed. Baseline characteristics and major outcome findings are provided in online supplementary table 1.
Receiver operating characteristic curves analysis
All analysed ENI definitions were significantly associated with long-term excellent (mRS 0–1) and favourable (mRS 0–2) functional outcome at 90 days follow-up. Analysing the whole study cohort, receiver operating characteristic (ROC, AUC (95% CI)) curves showed (figure 1) that NIHSS 24 hours had the highest discriminative ability to predict excellent (ROCNIHSS 24 hours, 0.86 (0.84–0.88)) and favourable long-term functional outcome (ROCNIHSS 24 hours, 0.86 (0.85–0.88)) in comparison to NIHSS percentage change (ROC%change, mRS ≤1: 0.81 (0.78–0.83) mRS ≤2: 0.81 (0.79–0.83)), NIHSS delta change (ROCΔchange, mRS ≤1: 0.74 (0.72–0.77), mRS ≤2: 0.77 (0.74–0.79)) and NIHSS admission (ROCAdm, mRS ≤1: 0.70 (0.68–0.73), mRS ≤2: 0.67 (0.6–0.71)). Comparing both discriminators with the highest AUCs, NIHSS 24 hours was significantly better (p<0.001) in outcome prediction than NIHSS percentage change. This finding was stable across the subanalysis stratified for stroke severity (table 1). In patients with severe strokes (NIHSS admission ≥16) NIHSS 24 hours and NIHSS percentage change showed similar AUC values (mRS ≤1: ROCNIHSS 24h, 0.89 (0.86–0.93); ROC% change, 0.89 (0.86–0.92); mRS ≤2: ROCNIHSS 24h, 0.87 (0.83–0.90); ROC% change, 0.86 (0.83–0.89)).

Comparison of National Institute of Health Stroke Scale (NIHSS) 24 hours and per cent change (NIHSS % change) based on receiver operator characteristic (ROC) curves for predicting excellent (modified Rankin Scale (mRS) 0–1) and favourable functional outcome (mRS 0–2) at 90 days. AUC, area under the curve.
ROC-based analysis of different surrogates for long-term functional outcome stratified by stroke severity
Binary thresholds
In comparison to preexisting binary ENI definitions mENI and dENI with sensitivities and specificities of 52.7% and 85.6% and 34.4% and 91%, respectively, an 8-point NIHSS threshold at 24 hours postintervention reached a sensitivity and specificity of 81.3% and 80% (figure 2), respectively, identifying 71% of patients with mRS 0–2 in this subgroup (online supplementary figure 2). Multivariable stepwise logistic regression (online supplementary figure 1 & additional discussion) revealed several independent individual (age, NIHSS on admission, Alberta Stroke Programme Early CT Score on admission) and procedural predictors (intravenous thrombolysis, anaesthesia, number of thrombectomy manoeuvres, final thrombolysis in cerebral infarction (TICI) scale scores that were significantly associated with reaching the 8-point NIHSS threshold. Vice versa, within this subgroup of patients, multivariable logistic regression analysis revealed that advanced age was the only independent predictor (adjusted OR 1.05, 95% CI 1.03 to 1.07, p<0.001) for turning the outcome prognosis from favourable (mRS 0–2) to poor (mRS 4–6) at 90 days follow-up with stepwise declining positive predictive values stratified across age groups (figure 3).
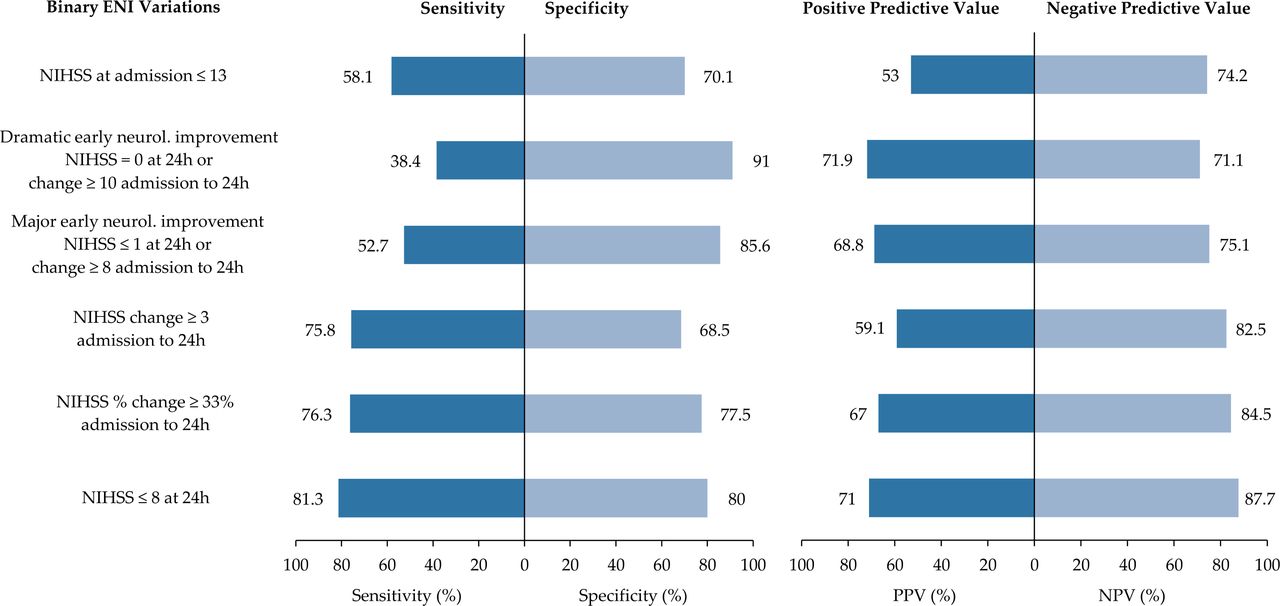
Sensitivity and specificity values together with their positive and negative predictive values of early neurological improvement threshold definitions for predicting favourable functional outcome (modified Rankin Scale (mRS) 0–2) at 90 days follow-up. ENI, early neurological improvement; NIHSS, National Institute of Health Stroke Scale.

{kind=link}
{kind=link}
{kind=link}
Positive and negative predictive values together with sensitivity and specificity in the subgroup of patients reaching the 8-point NIHSS threshold (24 hours after thrombectomy) stratified by age groups for achieving favourable outcome (modified Rankin Scale (mRS) 0–2). NIHSS, National Institute of Health Stroke Scale.
Discussion
Currently, it remains unclear which definition of early neurological recovery serves best as a surrogate for long-term favourable functional outcome after MT for anterior circulation stroke in daily clinical practice and which individual and procedural variables have the highest impact on outcome prediction. Our retrospective registry analysis revealed that (1) the NIHSS at 24 hours (with a threshold of NIHSS ≤8) regardless of baseline scores outperforms other early clinical surrogates including NIHSS delta and percentage change from baseline for predicting excellent (mRS 0–1) and favourable (mRS 0–2) outcome, (2) advanced age has the highest impact on reversing the prognosis from good to poor outcome (mRS 4–6) despite reaching the threshold of 8 NIHSS points at 24 hours after MT.
Based on past thrombolysis studies, neurological improvement after thrombectomy has been defined as an NIHSS point decrease 24 hours after treatment of 10 (dENI) or 8 (mENI) points or reaching 1/0 with regard to baseline scores.8 13–15 According to the NINDS study these definitions were found best to discriminate between treatment effects of the alteplase and the placebo group.10 16 However, past representative thrombectomy cohorts focusing on patients with proximal LVOs included a wide range of stroke severities with comparatively higher NIHSS scores on admission.13 Even though it has been shown that ENI and its variations, are linked significantly to functional independency (mRS 0–2) after MT within 6 hours from onset and beyond, some patients do not reach long-term favourable outcomes despite substantial early clinical improvement postintervention.2 4 Thus, dENI and mENI might rather serve as a binary treatment effect measure than a reliable outcome predictor in representative thrombectomy cohorts. Our results are in line with these findings showing an association of ENI with favourable outcome at 90 days but only with comparatively low sensitivities of 38% to 53%. To better discriminate and increase predictive values of ENI, previous studies investigated absolute and percentage change of NIHSS scores at 24 hours with regard to baseline observing a superiority of these measures.17–19 Recently, Rudilosso et al 2 investigated the timing (day 0, day 1, day 7) of ENI and found that 30% NIHSS decrease compared to baseline scores at day 0 had the highest value for long-term outcome prediction after MT. However, their prediction was based on a rather unrepresentative MT cohort for current daily clinical practice with a 79% rate of favourable functional outcome (mRS 0–2) at 90 days. Additionally, the assessment at day 0 possibly excludes patients that are treated with general anaesthesia attributed to possible prolonged effects of sedatives.20 21 In our study on outcome prediction analysis for functional independency at 90 days the NIHSS percentage change (ROC%change AUC 0.81) outperformed the NIHSS delta change (ROCΔchange AUC 0.77). This finding highlights the limitation of absolute NIHSS point changes that reflect disproportionally the improvement in patients with severe strokes reducing marginally the NIHSS without impact on functional outcome prediction. However, in our study the NIHSS at 24 hours regardless of baseline scores significantly outperformed (p<0.001) both aforementioned measures with ROC24 hours AUC of 0.86. This finding emphasises the importance of the clinical evaluation 24 hours after MT and shows that NIHSS at 24 hours as neurological assessment measure discriminates patients benefiting the most from MT at that time regardless of baseline scores and thus, provides predictive insights for treating physicians.22 Furthermore, clinical assessments 24 hours after MT might be of value in clinical research: future study designs 24 hours assessments might serve as study endpoints or as mRS 90 days surrogate for data samples with no availability of the 90 days follow-up. Multivariable logistic regression corroborated this finding, revealing independent individual and procedural-related predictors for reaching the threshold of 8 NIHSS points at 24 hours after MT. Nevertheless, in severely affected patients (initial NIHSS scores ≥16) NIHSS percentage change had a similar predictive value as the NIHSS 24 hours (ROC%change AUC 0.86 vs ROCNIHSS 24 hours AUC 0.88) most likely attributed to the realistic reflection of patients with highly dynamic NIHSS changes in this subgroup.
In our cohort 15.5% (118/754) of patients had a poor outcome (mRS 4–6) despite reaching the threshold (≤8 NIHSS) at 24 hours. Accordingly, we identified age as the only independent predictor for reversion of the outcome prediction at 90 days in this subgroup of patients. This finding is in line with previous studies showing that good outcome appears to decline with advancing age despite procedural success with complete reperfusion. These outcome dynamics are probably attributed to the high rates of coexisting comorbidities in this subgroup leading to a substantial susceptibility for complications (eg, hospital-acquired pneumonia) during the hospitalisation and rehabilitation phase.23 24 Hence, the post-treatment phase might be an equally important influenceable variable as the treatment itself in the subgroup of elderly patients to maintain the positive outcome prediction at 24 hours after MT.25
Limitations
Our study has several limitations that derive from a retrospective registry study design. Furthermore, the mRS as a global functional outcome measure is focused on motor recovery and therefore, as a functional endpoint it does not represent the quality of life status poststroke treatment. Besides, multivariable prediction models including all available pre- and post-treatment variables might increase the outcome prediction but the complexity would exceed the daily clinical usefulness.
Conclusion
The NIHSS at 24 hours after thrombectomy for anterior circulation stroke with a threshold of ≤8 points serves best as a surrogate in daily clinical practice for 90 days functional outcome regardless of baseline scores. Thus, the neurological assessment at 24 hours postintervention seems to be of high value for physicians and relatives to estimate the odds for patients’ 90 days independency. Advanced age decreases the predictive value of NIHSS at 24 hours for a favourable outcome to 55% for octogenarians and 33% for nonagenarians.
References
Footnotes
Twitter @MDoctoronboard
HK and UH contributed equally.
Collaborators GSR-ET Collaborators Tobias Boeckh-Behrens; Silke Wunderlich; Arno Reich; Martin Wiesmann; Ulrike Ernemann; Till-Karsten Hauser; Eberhard Siebert; Sarah Zweynert; Georg Bohner; Alexander Ludolph; Karl-Heinz Henn; Waltraud Pfeilschifter; Marlis Wagner; Joachim Röther; Bernd Eckert; Jörg Berrouschot; Albrecht Bormann; Christian Gerloff; Elke Hattingen; Gabor Petzold; Sven Thonke; Christopher Bangard; Christoffer Kraemer; Martin Dichgans; Frank Wollenweber; Lars Kellert; Franziska Dorn; Moriz Herzberg; Marios Psychogios; Jan Liman; Florian Stögbauer; Martina Petersen; Peter Kraft; Mirko Pham; Michael Braun; Gerhard F. Hamann; Andreas Kastrup; Christian Roth; Klaus Gröschel; Timo Uphaus; Volker Limmroth.
Contributors LM, HK and UH made substantial contributions to the conception and design of the work. LM, GS and HK performed the data analysis. Interpretation of the data was done by JF, GT, AA, CB, FF, UH, MB, HL, MD-C and GB. LM drafted the manuscript and all of the other authors revised it critically for important intellectual content. All authors approved the final version to be published. They agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the manuscript are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JF: Research support from the German Ministry of Science and Education (BMBF), German Ministry of Economy and Innovation (BMWi), German Research Foundation (DFG), European Union (EU), Hamburgische Investitions-/Förderbank (IFB), Medtronic, Microvention, Philips, Stryker; consultancy appointments; Acandis, Bayer, Boehringer Ingelheim, Cerenovus, Covidien, Evasc Neurovascular, MD Clinicals, Medtronic, Medina, Microvention, Penumbra, Route92, Stryker, Transverse Medical; stock holdings for Tegus. GT: Consultant for Acandis, Bayer Healthcare, Boehringer Ingelheim, BristolMyersSquibb/Pfizer, Covidien, Glaxo Smith Kline; lead investigator of the WAKE-UP study; principal investigator of the THRILL study; Grants by the European Union (Grant No. 278276 und 634809) and Deutsche Forschungsgemeinschaft (SFB 936, Projekt C2).
GT: reports receiving consulting fees from Acandis, grant support and lecture fees from Bayer, lecture fees from Boehringer Ingelheim, BristolMyersSquibb/Pfizer, and DaiichiSankyo, and consulting fees and lecture fees from Portola and Stryker.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. The deidentified data analysed in this study will be available and shared on upon reasonable request from any qualified investigator for the purpose of replicating the results after clearance by the ethics and registry committee.
Linked Articles
- Editorial commentary