Article Text

Abstract
Background The management of asymptomatic blunt cerebrovascular injury (BCVI) with respect to stroke prevention and vessel healing is challenging.
Objectives The aim of this systematic review was to determine if a specific treatment results in lower stroke rates and/or improved vessel healing in asymptomatic BCVI.
Data sources An electronic literature search of MEDLINE, EMBASE, Cochrane Library, CINAHL, SCOPUS, Web of Science, and ClinicalTrials.gov performed from inception to March 2020.
Study eligibility criteria Studies were included if they reported on a comparison of any treatment for BCVI and stroke and/or vessel healing rates.
Participants and interventions Adult patients diagnosed with asymptomatic BCVI(s) who were treated with any preventive medication or procedure.
Study appraisal and synthesis methods All studies were systematically reviewed and bias was evaluated by the Newcastle-Ottawa Scale. No meta-analysis was performed secondary to significant heterogeneity across studies in patient population, screening protocols, and treatment selection. The main outcomes were stroke and healing rate.
Results Of 8781 studies reviewed, 19 reported on treatment effects for asymptomatic BCVI and were included for review. Any choice of medical management was better than no treatment, but no specific differences between choice of medical management and stroke outcomes were found. Vessel healing was rare and the majority of healed vessels were following low-grade injuries.
Limitations Majority of the included studies were retrospective and at high risk of bias.
Conclusions or implications of key findings Asymptomatic BCVI should be treated medically using a consistent, local protocol. High-quality studies on the effect of individual antithrombotic agents on stroke rates and vessel healing for asymptomatic BCVI are required.
- carotid artery injuries
- vertebral artery
- vascular system injuries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Blunt cerebrovascular injury (BCVI) encompasses injury to the carotid and/or vertebral arteries resulting from high-speed deceleration or direct blunt trauma.1 The resulting injury confers significant risk of stroke and potential for devastating neurologic deficit.2 Historically BCVI was rarely diagnosed due to a lack of accessible, non-invasive imaging and minimal use of screening protocols.3 Often BCVI was not diagnosed until the patient had a stroke. Underdiagnosis of BCVI in older series led to a reported stroke rate of ~50% and a mortality of 25%.4 Modern series using screening protocols and CT angiography screening report an incidence of asymptomatic BCVI from 1% to 3%, with much lower stroke rates, owing to established management protocols.5–11
An evidence-based approach to stroke prevention for asymptomatic BCVI is challenging. The diagnosis is rare and often concomitant with other devastating injuries, such as severe traumatic brain injury (TBI), which may preclude intervention for BCVI. Additional challenges include patient identification, with screening protocols missing 20% of BCVIs,3 12 and the diverse medical and surgical management during the past 40 years.2 4–7 9–11 13–24 The modern management of BCVI is therefore largely born from single-center retrospective reviews over the span of many years. Rare diagnoses generally require large, multicenter studies over many years to accrue patients for a well-powered study on treatment, but these are resource-intensive. Major trauma society guidelines recommend antithrombotic therapy, but evidence regarding specific agents, dose, and duration has not been established.25 26 Clear indications for more invasive therapies, such as endovascular repair or surgery, are also not well established.
The aim of the current review was to collate the existing literature on the medical, surgical, and endovascular management of asymptomatic BCVI. Our goal was to determine if there is a clear ‘best’ therapy with respect to both stroke prevention and vessel healing. We hypothesized that medical therapy with an antithrombotic agent, regardless of choice of agent, would result in less strokes compared with no treatment.
Methods
MEDLINE, EMBASE, Cochrane Library, the Cumulative Index of Nursing and Allied Health Literature (CINAHL), SCOPUS, Web of Science, and ClinicalTrials.gov were searched from inception to August 2018 and updated to March 2020 to identify studies analyzing the effects of any intervention on asymptomatic BCVI outcomes. Search terms were identified by a trained librarian running the search in conjunction with the PI, and duplicated in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses minimum set of items for reporting. The search strategy for PubMed MEDLINE is detailed in online supplemental appendix 1.
Supplemental material
All abstracts were reviewed independently by two reviewers (PBM and SS in August 2018; PBM and EH in March 2020) and data abstracted in duplicate. Any disagreements were resolved by consensus. Included were studies reporting on comparisons of any treatment compared with any other treatment or no treatment in adult trauma patients (≥18 years of age). Excluded were studies that did not differentiate between symptomatic and asymptomatic patients, did not report on stroke rates related to treatment, or were case series (≤10 patients). The references of included studies were manually reviewed, and additional studies were included as appropriate. Studies with clear double-cohorting (overlapping time periods at the same institution) were included but patients were only included once.
The primary outcome of interest was stroke rate stratified by treatment. Vessel healing was included as a secondary outcome.
Study quality was assessed using the Newcastle-Ottawa Scale as recommended by the Cochrane Collaboration (version 5.1).27 Quality assessment was completed independently by two reviewers (SS and PBM, EH and PBM) and a discussion with consensus by a third author (BLZ) for any disagreements. Studies were then assigned a risk of bias of ‘high’, ‘moderate, or ‘low’ based on points in each domain. Given the heterogeneity of the included studies with respect to inclusion criteria, screening protocols, time frames, and outcome definitions, a meta-analysis was not possible.
Results
Study selection and demographics
The literature search returned 8781 abstracts (through March 2020). After removing duplicates and reviewing the abstracts for relevance, 185 articles were selected for full-text review. After applying the inclusion criteria, 19 studies remained (figure 1). There were no randomized control trials comparing the various treatment options. As shown in table 1, majority of the studies (14) were retrospective. Further, there was significant bias toward two centers, Denver and Memphis (n=11), as well as overlap in patient cohorts (n=8). All but three studies were from the USA. Eighteen studies reported on stroke rate and four studies reported on vessel healing.
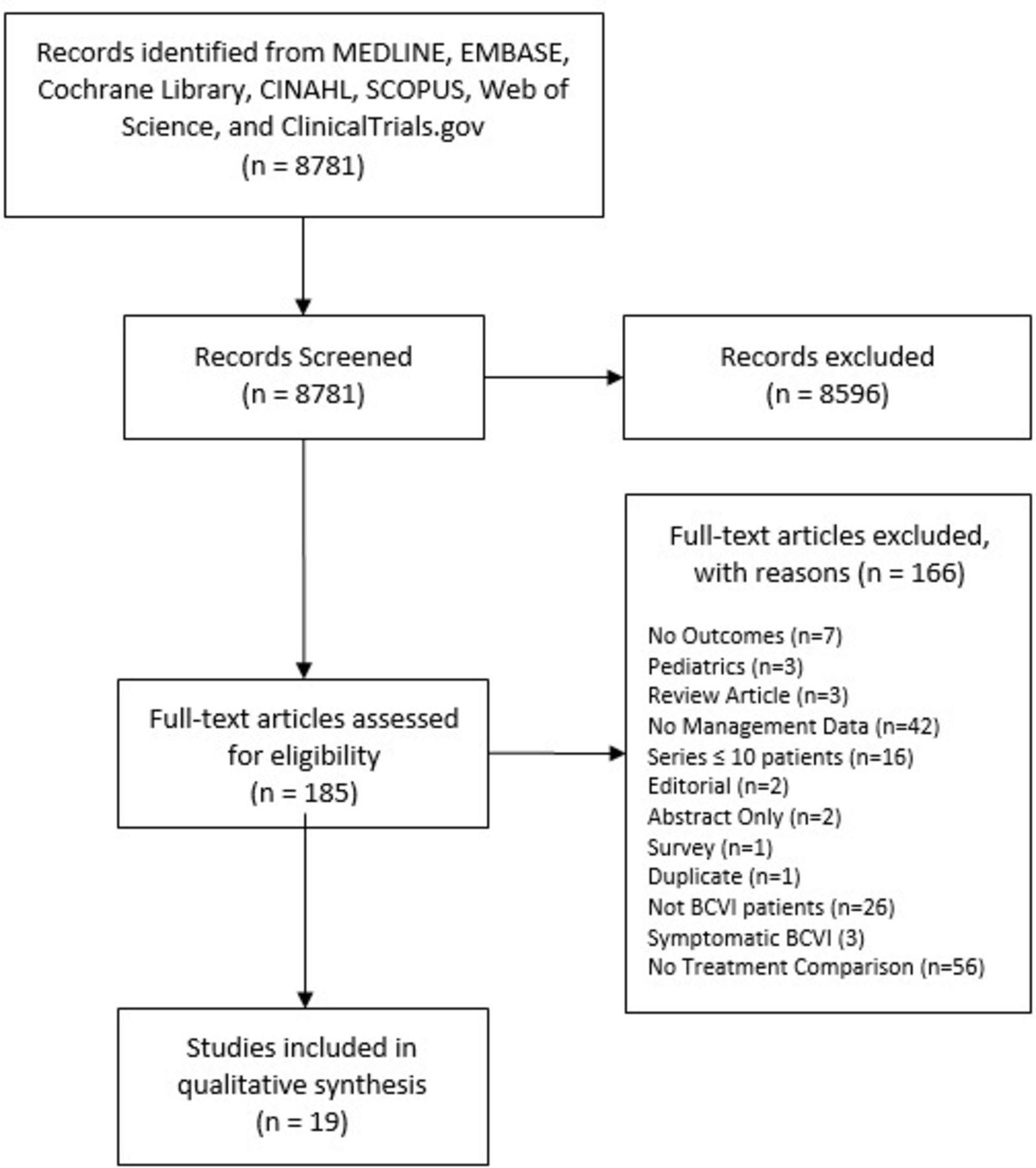
PRISMA flow diagram of study selection. BCVI, blunt cerebrovascular injury; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Studies reporting on treatments of asymptomatic BCVI and stroke/healing outcomes
Study quality and heterogeneity
The studies were heterogeneous and small in size. Only eight studies had more than 100 patients. The median number of patients was 76 per study. Majority of the studies were at a high risk of bias and only three were prospective (table 2). Studies were rated as high risk of bias largely due to limitations inherent in retrospective reviews and inability to control for potential confounders due to small sample sizes. There was inconsistency across studies in reporting of location (carotid artery injury (CAI) vs. vertebral artery injury (VAI)), grade of injury, treatment choice, and outcomes. Given the heterogeneity of studies with respect to population, geography, screening protocols, and treatment choices, a meta-analysis was not performed.
Assessment of study quality
Stroke
Patients with asymptomatic BCVI without treatment had an overall stroke rate of 25% as compared with antiplatelets (8%), anticoagulation (7%), endovascular (5%), or any treatment (3%) (table 3, figure 2). Studies reporting on treatment were mixed and often multiple treatments (acetylsalicylic acid (ASA), Plavix, warfarin, heparin) were reported together for the outcome of stroke (table 4). Most often patients with TBI were not treated for asymptomatic BCVI and were allocated to the ‘no treatment’ group. Only one study, by Callcut et al,16 examined the treatment of BCVI in the setting of TBI. This study was also the only study rated as low risk of bias. Of the treated patients in this study, half were treated with ASA and half were treated with heparin, with 84% of patients on a medical treatment by the seventh day of admission. The stroke rate in treated patients with TBI was 4% compared with 57% in untreated patients with TBI with concomitant BCVI.

{kind=link}
{kind=link}
Aggregate stroke rate for preventive treatment strategies in patients with asymptomatic blunt cerebrovascular injury. *No treatment often due to contraindications such a concomitant traumatic brain injury. ASA, acetylsalicylic acid.
Summary of outcomes by treatment
Results and conclusions of included studies for stroke rates
Six additional studies compared aspirin, heparin, and no treatment. Two studies by Miller et al6 23 using similar cohorts protocolized treatment of BCVI to unfractionated heparin unless anticoagulation was contraindicated, in which case patients received ASA 325 mg. Patients receiving no treatment had a high bleeding risk or withdrawal of care. The stroke rate was similar for ASA (4%) and heparin (3%). Cothren9 examined a 10-year cohort of patients diagnosed with BCVI. Heparin or ASA was given based on judgment of the attending surgeon. No patient treated with ASA (0%) and 1 patient (0.5%) treated with heparin progressed to stroke compared with 23 (23.5%) of patients who did not receive treatment (due to contraindication to antithrombotic). Biffl et al7 used a similar cohort as Cothren9 and the same treatment protocol. Similar stroke rates for ASA (9%) and heparin (1%) were found. Lebl et al15 examined the treatment effect of ASA and heparin on VAIs only. The decision to treat with ASA 81 mg or 325 mg, heparin, or to not treat was not clear for the methods. Overall stroke rates were 16% for ASA, 25% for heparin, and 5% for ‘no treatment’. Finally, Hwang et al18 favored ASA as the primary treatment in 34% of patients receiving treatment. There were no statistical differences in outcomes for those treated with ASA (6%), heparin (0%), or ‘no treatment’ (0%).
Eleven studies reported on the use of endovascular treatments for asymptomatic BCVI, often for higher grade injuries. Unfortunately, no stratification by grade of BCVI, treatment, and stroke rates was possible. One study stopped performing endovascular treatment during the study period.9 The largest study on endovascular therapy was by DiCocco et al.17 All patients in this study underwent traditional angiography to establish the diagnosis of BCVI. Grades II, III, and V lesions were treated with endovascular therapy and grades I and IV treated with medical management. Stroke rates were similar in patients treated with endovascular therapy (2.5%) compared with medical therapy (1.6%).
Vessel healing
The impact of therapy on vessel healing was reported by three studies, and all but one stratified healing by grade of BCVI and treatment (table 5).7 10 24 The follow-up protocol for identification of vessel healing was consistent between studies. Biffl et al24 performed repeat arteriography at 7 to 10 days in 63% of patients. In a follow-up study,7 the same authors performed repeat arteriography at 7 to 10 days for 73% of CAIs and 67% of VAIs. Finally, Wagenaar et al10 performed repeat imaging (unspecified type) at a mean of 11±0.9 days (range 1–220 days) in 66% of patients. Patients without repeat imaging were either discharged or died prior to the protocolized 7 to 10 days repeat imaging period. There were not enough data to compare individual therapies, but similar to patients who underwent any treatment 68% of vessels demonstrated healing compared with 43% undergoing ‘no treatment’. Grade I injuries were more likely to heal even if not treated (table 5).
Results and conclusions of included studies for vessel healing
Discussion
Our systematic review of the impact of medical therapies for asymptomatic BCVI demonstrates two main findings. First, any medical treatment (ASA, Plavix, heparin, warfarin) is likely better than no treatment for the prevention of stroke. Second, there is a paucity of high-quality evidence to guide the specific choice of medical treatment of asymptomatic BCVI to prevent stroke and/or promote vessel healing. Due to limitations inherent in retrospective reviews, only a single study was rated as at a low risk of bias. Overall reporting of screening protocols, treatment choice, and stratification by grade of injury was poor. Although we planned to conduct a meta-analysis, heterogeneity of included studies prevented this aim.
Overall, patients who received any treatment had lower stroke rates compared with patients who did not receive treatment. The allocation to treatment group was not randomized, or in many instances protocolized, which led to selection bias. Caution should be used when interpreting the results. Most patients who received ‘no treatment’ did so because other injuries such as TBI precluded antithrombotic therapy or the patient’s injuries were so devastating that care was transitioned to focus on comfort rather than survival. Similar challenges were seen when examining treatment effect on vessel healing. Only three studies assessed vessel healing, most often in grade I injuries, where healing rates were >50% even in patients not receiving treatment.7 10 24 The low rate of stroke and high rate of vessel healing in low-grade injuries may suggest the need for a more nuanced assessment of risks and benefits for antithrombotic therapy, especially in the setting of relative contraindications such as TBI.
The most common reason identified for not initiating medical therapy for asymptomatic BCVI was risk of bleeding, related to TBI. Only one study specifically included patients with TBI and demonstrated no progression of TBI on follow-up imaging prior to initiating therapy for BCVI.16 Untreated patients had higher grades of BCVI compared with treated patients, as well as a significantly higher stroke risk. The study did not control for baseline patient or injury characteristics, which may explain the results given the median time to stroke for BCVI is ~40 hours. With the high correlation of BCVI and TBI, future studies need to assess the risks and benefits of early antithrombotic therapy in patients with TBI.
Recently two other systematic reviews have examined the management of BCVI.26 28 The Eastern Association for the Surgery of Trauma in 2020 summarized results from 10 studies on the role of antithrombotics compared with no antithrombotics, favoring antithrombotics for stroke prevention with an OR of 0.20 (95% CI 0.06 to 0.65).26 Our review clearly agrees with this finding, although we chose not to perform a meta-analysis due to the high risk of bias and heterogeneity of study patients. We found that not treating asymptomatic BCVI had a stroke rate as high as 25%, compared with almost any other treatment modality where the stroke rate was <10%. Again, it is unclear whether this is entirely due to selection bias and the likelihood of more severely injured patients with head trauma to receive no treatment or delayed treatment. Similar recommendations were given recently by a group of Scandinavian neurosurgeons.28 This group went further to recommend commencing antithrombotic therapy early, even in the setting of TBI or solid organ injury. Indeed, the authors recommended low molecular weight heparin (LMWH) at an antithrombotic dose with transition to ASA 75 mg if feasible. Few studies have investigated the use of LMWH as part of a protocol for asymptomatic BCVI management, and to our knowledge no study has specifically investigated the use of LMWH in the treatment of asymptomatic BCVI.19 29 The risks and benefits for patients with BCVI are high stakes. Delayed or no treatment may result in devastating stroke, whereas treatment with antithrombotic may lead to progression of head injury or bleeding. Without high-quality, properly powered studies, the risks and benefits should be weighed for each individual patient, with the understanding that at time the benefits of antithrombotic therapy for stroke prevention may outweigh the risk of bleeding progression.
Vessel healing is also an important aspect of treatment and may help determine optimal duration of therapy. Currently, the optimal duration of medical treatment is unknown and some patients may stay on lifelong antiplatelet medications. Laser et al30 demonstrated the variable healing rate, well with 30% of grade II injuries worsening but 50% improving. Of higher grade (III/IV) 70% are unchanged at up to 6 months of follow-up. This suggests that patients with low-grade injury could be reimaged, as treatment cessation may be possible. Significantly fewer studies report on healing rates and this is likely related to inconsistent use of follow-up imaging and notoriously poor follow-up of trauma patients. Future studies should include follow-up imaging to delineate time to vessel healing and optimal treatment duration.
Our review has several strengths. First, our search was comprehensive, identifying 19 studies comparing different treatments for BCVI. Further, we assessed the quality of individual studies in accordance with best practices for systematic reviews. Second, rather than perform a meta-analysis, we opted to report results based on specific treatment modalities. This allowed us to compare stroke rates for the two most common treatment choices, ASA, and heparin. The estimated treatment effect is important to establish for future study design, including sample size calculation. Finally, although the overall risk of bias for studies was moderate to high, our review outlines best practices for reporting in future studies on BCVI. We recommend clearly identifying patients with asymptomatic BCVI, stating grade of vessel injury, clearly stating treatment/follow-up protocols including contraindications to treatment, and reporting results both by treatment but also by the highest grade of BCVI in patients with more than one vessel injured.
As with any systematic review our results are limited by the quality of the literature. Given the rarity of BCVI, well-designed multi-institutional studies are required. A trial comparing ‘no treatment’ with treatment for asymptomatic BCVI is likely not ethical. Ideally a randomized non-inferiority trial would compare the two most common treatments, ASA (81 mg or 325 mg) with heparin, with clearly defined inclusion/exclusion criteria.
Although BCVI is uncommon, the potential outcome of stroke can be devastating. Any medical treatment is better than no treatment and future studies are needed to determine the ‘best’ treatment with respect to stroke prevention and vessel healing, as well as clearly define which patients have true contraindications to antithrombotic therapy.
Ethics statements
Ethics approval
Ethical approval was not required because in all the reviewed studies informed consent was obtained by the primary investigators.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conception and design: PBM, LM, SSe, SSa, BLZ. Acquisition of data: PBM, SSe, EH, LM. Analysis and interpretation of data: all. Drafting the article and revising it: PBM. Final approval of published version: all.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.