Article Text

Abstract
Background Randomised controlled trials with perfusion selection have shown benefit of endovascular treatment (EVT) for ischaemic stroke between 6 and 24 hours after symptom onset or time last seen well. However, outcomes after EVT in these late window patients without perfusion imaging are largely unknown. We assessed their characteristics and outcomes in routine clinical practice.
Methods The Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands Registry, a prospective, multicentre study in the Netherlands, included patients with an anterior circulation occlusion who underwent EVT between 2014 and 2017. CT perfusion was no standard imaging modality. We used adjusted ordinal logistic regression analysis to compare patients treated within versus beyond 6.5 hours after propensity score matching on age, prestroke modified Rankin Scale (mRS), National Institutes of Health Stroke Scale, Alberta Stroke Programme Early CT Score (ASPECTS), collateral status, location of occlusion and treatment with intravenous thrombolysis. Outcomes included 3-month mRS score, functional independence (defined as mRS 0–2), and death.
Results Of 3264 patients who underwent EVT, 106 (3.2%) were treated beyond 6.5 hours (median 8.5, IQR 6.9–10.6), of whom 93 (87.7%) had unknown time of stroke onset. CT perfusion was not performed in 87/106 (80.2%) late window patients. Late window patients were younger (mean 67 vs 70 years, p<0.04) and had slightly lower ASPECTS (median 8 vs 9, p<0.01), but better collateral status (collateral score 2–3: 68.3% vs 57.7%, p=0.03). No differences were observed in proportions of functional independence (43.3% vs 40.5%, p=0.57) or death (24.0% vs 28.9%, p=0.28). After matching, outcomes remained similar (adjusted common OR for 1 point improvement in mRS 1.04, 95% CI 0.56 to 1.93).
Conclusions Without the use of CT perfusion selection criteria, EVT in the 6.5–24-hour time window was not associated with poorer outcome in selected patients with favourable clinical and CT/CT angiography characteristics. randomised controlled trials with lenient inclusion criteria are needed to identify more patients who can benefit from EVT in the late window.
- Thrombectomy
- Stroke
Data availability statement
Individual patient data cannot be made available, because no patient approval has been obtained for sharing data, even in coded form. However, syntax and output files of statistical analyses can be made available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Following the publication of the first positive randomised controlled trials in endovascular treatment (EVT) for acute ischaemic stroke,1 guidelines recommended EVT in patients with a large vessel occlusion of the anterior circulation if treatment could be initiated within 6 hours from symptom onset.2 3 However, this paradigm leads to exclusion from EVT of a significant number of patients who had a stroke, since an estimated 30% of them present between 6 and 24 hours after symptom onset or after the time that patients were last seen well (LSW).4 The 6-hour time window for EVT was based on the inclusion criteria used in previous trials and the observation that treatment effect decreased over time to non-significant at a time point beyond 6 hours.5 6 The HERMES collaborators demonstrated that treatment effect was still present up to 7.3 hours in included patients.5 However, some of the included trials used additional advanced imaging for patient selection. Therefore, these results cannot be generalised to all patients who had a stroke presenting beyond the 6-hour time window.
In 2018, two randomised controlled trials, DEFUSE 3 and DAWN, showed that EVT is safe and effective in patients treated in an extended time window of up to 16 or 24 hours after symptom onset or time LSW.7 8 In these trials, selection of patients was predominantly based on perfusion imaging. Following the publication of these trials, EVT for patients beyond 6 hours from symptom onset or LSW who meet the inclusion criteria of these trials with mandatory perfusion imaging is also recommended.9 However, on a global scale, software with automated perfusion analysis is currently offered to a minority of late window patients who had a stroke. Furthermore, the inclusion criteria used in these trials exclude a majority of late window patients of whom it is yet unknown if they may benefit from EVT.4 We describe characteristics, outcome and safety of patients treated with EVT within and beyond the 6.5-hour time window in clinical practice prior to the current guidelines with DAWN/DEFUSE 3 paradigms.
Methods
Patient inclusion
We analysed patients from the Multicenter Clinical Registry of Endovascular treatment for Acute ischaemic stroke in the Netherlands (MR CLEAN Registry), which was a national, prospective, observational stroke registry in 16 intervention centres that perform EVT in the Netherlands. Registration of patients treated with EVT started directly after the original Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) trial was finished, and was used to study safety and efficacy of EVT in routine clinical practice.10 All patients in whom EVT was considered indicated and who underwent an arterial groin puncture were included. EVT consisted of arterial catheterisation with a microcatheter to the level of the occlusion, followed by mechanical thrombectomy and/or thrombus aspiration, with or without delivery of a thrombolytic agent. The method of EVT was left to the discretion of the treating physician.
An independent core lab, blinded for all outcome measures, assessed imaging data, including early ischaemic changes with the Alberta Stroke Programme Early CT Score (ASPECTS) on baseline non-contrast CT,11 collateral status on baseline single phase CT angiography,12 and reperfusion status on digital subtraction angiography after EVT. Reperfusion was scored with the extended Thrombolysis in Cerebral Infarction (eTICI) score, which ranges from grade 0 (no reperfusion) to grade 3 (complete reperfusion).13 Data were collected before publication of the DAWN and DEFUSE 3 trials, and CT perfusion was not a standard imaging modality in our registry. None of the participating stroke centres used RAPID software in this time period. No records were kept concerning the use of CT perfusion imaging in patients who underwent EVT between March 2014 and June 2016, but this was documented for patients treated after June 2016 and for all late window patients. MR diffusion weighted imaging was performed only in two late window patients and therefore not used in the current analysis.
In the present study, we included all patients with an intracranial proximal occlusion in the anterior circulation (intracranial carotid artery, middle cerebral artery (M1/M2) or anterior cerebral artery (A1/A2)) demonstrated on CT angiography, treated with EVT between 16 March 2014 and 1 November 2017 in centres that had participated in the MR CLEAN trial. Exclusion criteria were age <18 years or an unknown time between onset or LSW and groin puncture. Although the recommended time window for EVT at the time of this study was 6 hours,9 in clinical practice the start of procedure (time of groin puncture) was sometimes slightly delayed due to logistical reasons. Therefore, late window patients were defined as patients in whom treatment was started at or beyond 6.5 hours after documented symptom onset or after time LSW in case of unknown stroke onset.
Outcome measures
Primary outcome was functional outcome at 3 months after stroke on the mRS, ranging from 0 (no symptoms) to 6 (death).14 Secondary outcomes were functional independence, successful reperfusion and clinical improvement after intervention. Functional independence was defined as a 3-month mRS score of 0–2. Successful reperfusion was defined as an eTICI score of 2B (reperfusion of >50% of the previously occluded area) or higher. If completion angiography was not performed in two directions, reperfusion status was graded 2A at most. A decrease of ≥4 points on the National Institutes of Health Stroke Scale (NIHSS) between presentation and 24–48 hours postintervention or complete recovery (NIHSS 0) was considered a significant early clinical improvement.15 Safety outcomes were peri-interventional complications such as vessel dissections, perforations or other vascular injuries, vasospasms or new clots in different vascular territories, symptomatic intracranial haemorrhage and mortality at 3 months. Symptomatic intracranial haemorrhage was defined as haemorrhage related to neurological deterioration (decline of at least four points on the NIHSS) or death.16
Missing data
Missing NIHSS scores were retrospectively scored with a standardised score chart that used the reported neurological examination information. The mRS score was assessed as part of usual care in all centres. Any follow-up mRS score of 0–5 assessed within 30 days was considered invalid and was replaced using multiple imputation. Multiple imputation was performed before selection of early and late window patients with the following variables: age, prestroke mRS, blood pressure, history of diabetes mellitus, myocardial infarction, previous stroke, atrial fibrillation or hypercholesterolaemia, NIHSS at presentation, ASPECTS at presentation, location of occlusion, collateral status, onset-to-groin time, reperfusion status, postintervention NIHSS and 3-month mRS.
Statistical analysis
Baseline characteristics of late time window patients treated at or beyond 6.5 hours after symptom onset or time LSW were compared with those of early time window patients treated within 6.5 hours using χ2 tests for categorical variables and independent t-tests or Mann-Whitney U tests for continuous variables. Nearest-neighbour propensity score matching of late window and early window patients in a 1:2 ratio with a calliper width of 0.2 was performed with five imputed datasets to minimise the risk of confounding by indication.17 Late window and early window patients were matched on age, prestroke mRS, baseline NIHSS, baseline ASPECTS, location of occlusion, collateral status and treatment with intravenous thrombolysis (IVT) prior to EVT.18 Unmatched patients were excluded from further analysis. In each matched imputed dataset, logistic regression analyses were used to determine ORs for patients treated beyond compared with patients treated within the 6.5-hour time window. Effect estimates of regression analyses were corrected for the same variables as those used for matching to further minimise the risk of confounding. We estimated the pooled common OR as a measure of shift in the direction of a better outcome on the mRS. Pooled ORs were obtained using Rubin’s rules. Statistical analyses, multiple imputation and matching procedure were conducted with SPSS for Windows, V.24.0.
Results
Patient characteristics
Of 3264 included patients, 3158 (96.8%) underwent EVT within 6.5 hours from symptom onset or LSW, of whom 842 (26.7%) had an unknown time of stroke onset. Of the 106 late window patients, the majority (n=93, 87.7%) had an unknown time of stroke onset (figure 1). Median time from onset or LSW to groin puncture was 195 min (IQR 150–250) for early window patients versus 508 min (IQR 415–637) for late window patients. Late window patients were slightly younger (67 vs 70 years, p=0.04) and received IVT less frequently (22.9% vs 76.8%, p<0.01) than early window patients. ASPECT-score at presentation was lower (median 8 vs 9, p<0.01) while collateral status was better for late window patients (dichotomised good collaterals filling >50%: 68.3% vs 57.7%, p=0.03). Of patients treated between 2016–2017, 15/65 late window patients (23.1%) underwent CT perfusion imaging prior to EVT versus 319/1673 (19.1%) in the early window (table 1).
Baseline characteristics
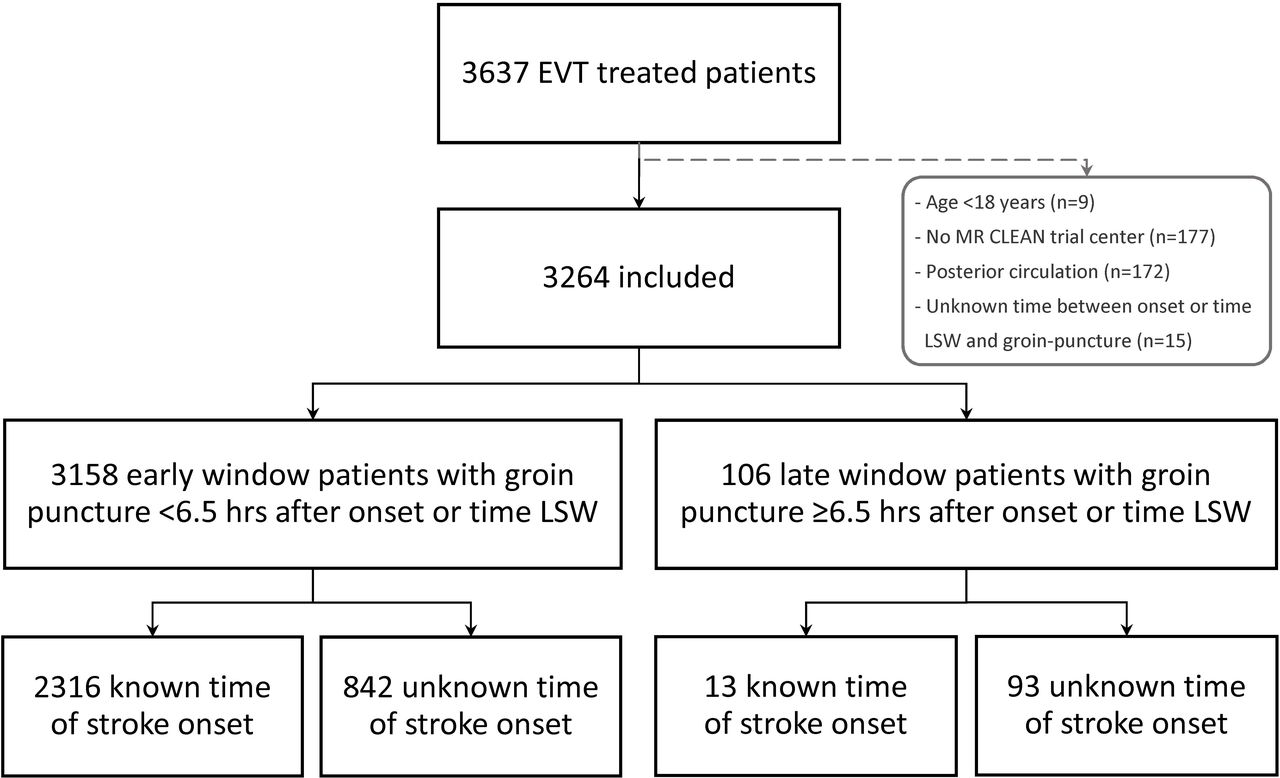
Flowchart of patients. EVT, endovascular treatment; LSW, last seen well; MR CLEAN, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands.

{kind=link}
{kind=link}
Distribution of mRS scores at 3 months. EVT, endovascular treatment; LSW, last seen well; mRS, modified Rankin Scale.
Of patients who underwent EVT outside the 6.5-hour time window, baseline characteristics were similar between those with known time of stroke onset and those with unknown time of stroke onset, except for a higher rate of IVT in known stroke onset patients (46.2% vs 19.6%, p=0.03) (online supplemental table 1). Patients treated beyond 6.5 hours who underwent CT perfusion imaging had lower NIHSS at presentation (median 13 vs 16, p=0.01) and appeared to have slightly lower ASPECTS at presentation (median 7 vs 9, p=0.09) compared with patients treated beyond 6.5 hours who did not undergo CT perfusion imaging, but all other characteristics were comparable (online supplemental table 2). Of all patients with a known time of stroke onset, there were no differences in baseline characteristics between those treated beyond versus within 6.5 hours, aside from a higher rate of IVT in the group treated in the early time window (79.0% vs 46.2%, p<0.01) (online supplemental table 3).
Supplemental material
Clinical outcomes
Proportions of functional independence at 3 months (43.3% vs 40.5%, p=0.57), successful reperfusion (56.9% vs 61.7%, p=0.33) and mortality (24.0% vs 28.9%, p=0.28) were comparable between late and early window patients (table 2, figure 2).
Outcome measures
Logistic regression analysis showed no difference in outcomes (online supplemental table 4). Overall, 4.0% of data points in the imputation model were missing, and the proportion of missing mRS scores was 6.5%. After nearest-neighbour propensity score matching of five imputed datasets in a 1:2 ratio, 96.4% of the late window patients could be matched to two early window patients. Baseline characteristics of the five matched datasets are described in online supplemental table 5. Adjusted logistic regression after matching showed no significant difference in distribution of the mRS between the late window patients and their matched early window patients (pooled adjusted common OR for a shift of 1 point improvement in mRS 1.04, 95% CI 0.56 to 1.93) (table 3). Furthermore, proportions of functional independence at 3 months (pooled adjusted OR (aOR) 1.17, 95% CI 0.58 to 2.37), successful reperfusion (aOR 0.75, 95% CI 0.41 to 1.39) and postintervention significant early clinical improvement (aOR 0.79, 95% CI 0.44 to 1.43) were similar. Concerning safety parameters, no significant difference was found in rates of peri-interventional complications (aOR 1.52, 95% CI 0.50 to 4.58), symptomatic intracranial haemorrhage (aOR 1.03, 95% CI 0.26 to 4.04) or mortality (aOR 0.76, 95% CI 0.32 to 1.79) (table 3).
Logistic regression analysis in matched patients
Of patients treated beyond 6.5 hours, there were no differences in outcomes between those with known and unknown time of stroke onset (online supplemental table 1). Those who underwent CT perfusion imaging more often had symptomatic intracranial haemorrhage (14.3% vs 2.4%, p=0.02), but all other outcomes were similar (online supplemental table 2). Finally, no differences were found between outcomes of patients with known time of stroke onset treated either beyond versus within 6.5 hours (online supplemental table 3).
Discussion
We observed similar rates of functional independence, successful reperfusion and safety outcomes in selected patients with favourable characteristics, such as good collaterals, treated with EVT beyond 6.5 hours from symptom onset or time LSW compared with patients treated within 6.5 hours without mandatory perfusion imaging.
Although several studies showed that EVT is safe and effective in late window patients selected using only non-contrast CT and CT angiography,19 20 the role of ASPECTS and collateral status compared with MR diffusion or CT perfusion imaging requires further study. Previous studies showed no additional value of CT perfusion imaging in either prognostication of 3-month mRS after EVT compared with non-contrast CT ASPECT score,21 or in selection of patients with good outcomes after EVT beyond 6 hours compared with selection using solely non-contrast CT and CT angiography.22–25 Two other studies showed that a substantial proportion of DAWN-ineligible and DEFUSE 3-ineligible patients also reached functional independence at 3 months after EVT.26 27 Our findings confirm that in clinical practice similar outcomes can be obtained in selected patients without additional determination of core and penumbra. Randomised trials without mandatory perfusion imaging, such as the ongoing pragmatic MR CLEAN-LATE,28 which is based on collateral and ASPECT scoring, may be able to identify more patients who can still benefit from EVT outside the 6-hour time window and deliver further modifications in guidelines for patients who had a stroke in the late time window.29
A previous analysis of the MR CLEAN Registry showed that in patients treated within 6.5 hours, every hour of delay resulted in a 5.3% decrease of probability of functional independence.6 However, that analysis excluded late window patients treated beyond 6.5 hours after onset and only patients treated before June 2016 were included. In the present study, only 3.2% of patients were treated beyond 6.5 hours and we observed similar outcomes compared with patients treated within 6.5 hours, which suggests patient selection. Although the specifics of CT perfusion scans of patients have not yet been assessed, it is unlikely that these had much influence on patient selection or outcome since we found similar low rates of the use of CT perfusion in early and late window patients. Furthermore, our patients were treated before the publication of the DAWN/DEFUSE 3 trials, in a time when perfusion imaging was not common practice and patients presenting beyond 6 hours of onset or time LSW were generally excluded from EVT, which may also explain the low proportion of late window patients. We found that late window patients were younger and had better collateral status. This suggests selection on increased collateral supply, which a post hoc analysis of the original MR CLEAN study showed to be strongly associated with better outcome after EVT,30 and may imply that those patients have more salvageable tissue.
The majority of late window patients in this study had an unknown time of stroke onset. This is similar to the population treated in the DAWN and DEFUSE 3 studies (respectively, 90% and 66% unknown onset). There are indications that in wake-up strokes, stroke onset occurs shortly before awakening.31 This implies that the actual time between onset and EVT may well be within the accepted time window. Therefore, it would be interesting to see if similar results can be obtained in known stroke onset patients treated >6 hours after onset and wake-up patients who had a stroke treated >6 hours after awakening. Although we found no differences between characteristics and outcomes of patients with known versus unknown time of stroke onset treated beyond 6.5 hours, nor of known-onset patients who had a stroke treated either beyond versus within 6.5 hours, our study is limited by the fact that only 12.3% of patients had documented known-onset stroke in the late window.
The main strength of our observational study is that it was performed with data from a large, nationwide EVT registry from routine clinical practice without prespecified imaging selection other than an anterior circulation occlusion. Furthermore, we used adjusted logistic regression after propensity score matching to minimalise the risk of differences in outcome between patients treated within versus beyond the 6.5-hour time window due to differences in baseline characteristics. An important limitation of this study is that no records were kept of the group of untreated late window patients. Therefore, the exact level and method of patient selection cannot be assessed and, although outcomes are similar to those of early window patients, no evidence of clinical benefit can be established without a control group. Furthermore, since there is currently no data available concerning the specific CT perfusion results, it is not possible to compare penumbra and core status between early and late window patients. However, it is unlikely that this influenced overall outcomes, since only a small minority of patients underwent CT perfusion imaging.
Conclusions
Without the use of the DAWN or DEFUSE 3 trial CT perfusion selection criteria, EVT in the 6.5–24-hour time window was safe and not associated with poorer outcome in selected patients with favourable clinical and CT/CTA characteristics. Randomised controlled trials with more lenient inclusion criteria than the DAWN and DEFUSE 3 are needed to identify more patients who can benefit from EVT in the late window.
Data availability statement
Individual patient data cannot be made available, because no patient approval has been obtained for sharing data, even in coded form. However, syntax and output files of statistical analyses can be made available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was conducted using observational data obtained in context of the MR CLEAN Registry. The MR CLEAN Registry protocol was reviewd by the Erasmus University Medical Center Central Ethics Committee, which served as the central review board for all participating centers. The requirements for written informed consent was waived, but patients or their representatives were provided with information on the study orally and in writing.
Acknowledgments
We acknowledge the support of the Netherlands Cardiovascular Research Initiative which is supported by the Dutch Heart Foundation, CVON2015-01: CONTRAST, and the support of the Brain Foundation Netherlands (HA2015.01.06).
References
Supplementary material
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators The MR CLEAN Registry investigators: Jan Albert Vos, (Radiology, Sint Antonius Hospital, Nieuwegein); Kars C.J. Compagne, (Radiology, Erasmus MC University Medical Center); Manon Kappelhof (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Josje Brouwer (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Sanne J. den Hartog (Department of Neurology, Radiology, Public Health, Erasmus MC University Medical Center); Wouter H. Hinsenveld (Department of Neurology, Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Bob Roozenbeek (Department of Neurology, Erasmus MC University Medical Center); Jonathan M. Coutinho (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Marianne A.A. van Walderveen (Radiology, Leiden University Medical Center); Julie Staals (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Jeannette Hofmeijer (Department of Neurology, Rijnstate Hospital, Arnhem); Jasper M. Martens (Radiology, Rijnstate Hospital, Arnhem); Sebastiaan F. de Bruijnl (Department of Neurology, HAGA Hospital, the Hague); Lukas C. van Dijk (Radiology, HAGA Hospital, the Hague); H. Bart van der Worp (Department of Neurology, University Medical Center Utrecht); Rob H. Lo (Radiology, University Medical Center Utrecht); Ewoud J. van Dijk (Department of Neurology, Radboud University Medical Center, Nijmegen); Hieronymus D. Boogaarts (Neurosurgery, Radboud University Medical Center, Nijmegen); J. de Vries (Department of Neurology, Isala Klinieken, Zwolle); Paul L.M. de Kort (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Julia van Tuijl (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Jo P. Peluso (Radiology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Puck Fransen (Department of Neurology, Isala Klinieken, Zwolle); Jan S.P. van den Berg (Department of Neurology, Isala Klinieken, Zwolle); Boudewijn A.A.M. van Hasselt (Radiology, Isala Klinieken, Zwolle); Leo A.M. Aerden (Department of Neurology,Reinier de Graaf Gasthuis, Delft); René J. Dallinga (Radiology, Reinier de Graaf Gasthuis, Delft); Maarten Uyttenboogaart; Omid Eschgi (Department of Neurology, University Medical Center Groningen); Reinoud P.H. Bokkers (Radiology, University Medical Center Groningen); Tobien H.C.M.L. Schreuder (Department of Neurology, Atrium Medical Center, Heerlen); Roel J.J. Heijboer (Radiology, Atrium Medical Center, Heerlen); Koos Keizer (Department of Neurology, Catharina Hospital, Eindhoven); Lonneke S.F. Yo (Radiology, Catharina Hospital, Eindhoven); Heleen M. den Hertog (Department of Neurology, Isala Klinieken, Zwolle); Emiel J.C. Sturm (Radiology, Medical Spectrum Twente, Enschede); Paul J.A.M. Brouwers (Department of Neurology, Medical Spectrum Twente, Enschede); Marieke E.S. Sprengers (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Sjoerd F.M. Jenniskens (Radiology, Radboud University Medical Center, Nijmegen); René van den Berg (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Albert J. Yoo (Department of Radiology, Texas Stroke Institute, Texas, United States of America); Ludo F.M. Beenen (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Alida A. Postma (Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Stefan D. Roosendaal (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Bas F.W. van der Kallen (Department of Radiology, Haaglanden MC, the Hague); Ido R. van den Wijngaard (Department of Radiology, Haaglanden MC, the Hague); Adriaan C.G.M. van Es (Radiology, Rijnstate Hospital, Arnhem); Joost Bot (Department of Radiology, Amsterdam UMC, Vrije Universiteit van Amsterdam, Amsterdam); Pieter-Jan van Doormaal (Radiology, Erasmus MC University Medical Center); Anton Meijer (Radiology, Radboud University Medical Center, Nijmegen); Elyas Ghariq (Department of Radiology, Haaglanden MC, the Hague); Marc P. van Proosdij (Department of Radiology, Noordwest Ziekenhuisgroep, Alkmaar); G. Menno Krietemeijer (Radiology, Catharina Hospital, Eindhoven); Dick Gerrits (Radiology, Medical Spectrum Twente, Enschede); Wouter Dinkelaar (Radiology, Erasmus MC University Medical Center); Auke P.A. Appelman (Radiology, University Medical Center Groningen); Bas Hammer (Radiology, HAGA Hospital, the Hague); Sjoert Pegge (Radiology, Radboud University Medical Center, Nijmegen); Anouk van der Hoorn (Radiology, Radboud University Medical Center, Nijmegen); Saman Vinke (Neurosurgery, Radboud University Medical Center, Nijmegen); Wouter J. Schonewille (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Naziha el Ghannouti (Department of Neurology, Erasmus MC University Medical Center); Martin Sterrenberg (Department of Neurology, Erasmus MC University Medical Center); Wilma Pellikaan (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Rita Sprengers (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Marjan Elfrink (Department of Neurology, University Medical Center Groningen); Michelle Simons (Department of Neurology, Rijnstate Hospital, Arnhem); Marjolein Vossers (Radiology, Rijnstate Hospital, Arnhem); Joke de Meris (Neurology, Haaglanden MC, the Hague); Tamara Vermeulen (Neurology, Haaglanden MC, the Hague); Annet Geerlings (Department of Neurology, RadbouAnnet Geerlingsd University Medical Center, Nijmegen); Gina van Vemde (Department of Neurology, Isala Klinieken, Zwolle); Tiny Simons (Department of Neurology, Atrium Medical Center, Heerlen); Gert Messchendorp (Department of Neurology, University Medical Center Groningen); Nynke Nicolaij (Department of Neurology, University Medical Center Groningen); Hester Bongenaar (Department of Neurology, Catharina Hospital, Eindhoven); Karin Bodde (Department of Neurology, Reinier de Graaf Gasthuis, Delft); Sandra Kleijn (Department of Neurology, Medical Spectrum Twente, Enschede); Jasmijn Lodico (Department of Neurology, Medical Spectrum Twente, Enschede); Hanneke Droste (Department of Neurology, Medical Spectrum Twente, Enschede); Maureen Wollaert (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Sabrina Verheesen (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); D. Jeurrissen (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Erna Bos (Department of Neurology, Leiden University Medical Center); Yvonne Drabbe (Department of Neurology, HAGA Hospital, the Hague); Michelle Sandiman (Department of Neurology, HAGA Hospital, the Hague); Nicoline Aaldering (Department of Neurology, Rijnstate Hospital, Arnhem); Berber Zweedijk (Department of Neurology, University Medical Center Utrecht); Jocova Vervoort (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Eva Ponjee (Department of Neurology, Isala Klinieken, Zwolle); Sharon Romviel (Department of Neurology, RadbouAnnet Geerlingsd University Medical Center, Nijmegen); Karin Kanselaar1 (Department of Neurology, RadbouAnnet Geerlingsd University Medical Center, Nijmegen); Denn Barning (Radiology, Leiden University Medical Center); Vicky Chalos (Department of Neurology, Public Health, Erasmus MC University Medical Center); Ralph R. Geuskens (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Tim van Straaten (Department of Neurology, RadbouAnnet Geerlingsd University Medical Center, Nijmegen); Saliha Ergezen (Department of Neurology, Erasmus MC University Medical Center); Roger R.M. Harmsma (Department of Neurology, Erasmus MC University Medical Center); Daan Muijres (Department of Neurology, Erasmus MC University Medical Center); Olvert A. Berkhemer (Department of Neurology, Erasmus MC University Medical Center; Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam and Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Anna M.M. Boers (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam and Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); J. Huguet (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); P.F.C. Groot (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Marieke A. Mens (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Katinka R. van Kranendonk (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Kilian M. Treurniet (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Manon L. Tolhuisen (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam and Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Heitor Alves (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Annick J. Weterings (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Eleonora L.F. Kirkels (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Eva J.H.F. Voogd (Department of Neurology, Rijnstate Hospital, Arnhem); Lieve M. Schupp (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Sabine Collette (Department of Neurology, Radiology, University Medical Center Groningen); Adrien E.D. Groot (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Natalie E. LeCouffe (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Praneeta R. Konduri (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Haryadi Prasetya (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Nerea Arrarte-Terreros (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Lucas A. Ramos (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam).
Contributors LD and IRvdW: conception and design of the study. LD and FAVP: drafting of the manuscript. LD: data and statistical analysis. EV and HFL: supervision of statistical analysis. IGHJ, MJHLM and R-JBG: acquisition of clinical data. CBLMM, YBWEMR, DWJD, WHvZ and RJvO: members of the trial executive committee and critical review and revision. BJE, RL, MJHLW, JB, GJLàN and ACGMvE: critical review and revision for valuable intellectual content. All authors provided final approval of the version to be published.
Funding The MR CLEAN Registry was partly funded by TWIN Foundation, Erasmus MC University Medical Center, Maastricht University Medical Center and Academic Medical Center Amsterdam. No funding was obtained for this specific substudy. Robin Lemmens is a senior clinical investigator of FWO Flanders.
Competing interests Erasmus MC received funds from Stryker and Bracco Imaging by DWJD. MUMC received funds from Stryker and Codman for consultations by WHvZ. WHvZ and RJvO are principal investigators for the MR CLEAN-LATE trial. R-JBG and FAVP are coordinating researchers for MR CLEAN-LATE. CBLMM received funds from TWIN Foundation (related to this project, paid to institution) and from CVON/Dutch Heart Foundation, Stryker, European Commission, Health Evaluation Netherlands (unrelated; all paid to institution). YBWEMR, CBLMM and IGHJ are shareholders of Nico.lab, a company that focuses on the use of artificial intelligence for medical imaging analysis. RL reports institutional fees from Ischamaview for consultancy. The other authors had no conflicting interests.
Provenance and peer review Not commissioned; externally peer reviewed.