Article Text

Abstract
Background: Bleeding and transfusion after percutaneous coronary intervention (PCI) are known predictors of mortality. Transradial arterial access reduces bleeding and transfusion related to femoral access complications, although its association with mortality is unknown.
Objective: To determine the association of arterial access site (radial or femoral) with transfusion and mortality in unselected PCIs.
Design, setting and patients: By data linkage of three prospectively collated provincial registries, 38 872 procedures in 32 822 patients in British Columbia were analysed. The association between access site, transfusion and outcomes was assessed by logistic regression, propensity score matching and probit regression.
Main outcome measures: 30-Day and 1-year mortality.
Results: 1134 (3.5%) patients had at least one blood transfusion. Transfused patients had a significantly increased 30-day and 1-year mortality, adjusted odds ratio (95% CI) 4.01 (3.08 to 5.22) and 3.58 (2.94 to 4.36), respectively. By probit regression the absolute increase in risk of death at 1 year associated with receiving a transfusion was 6.78%. The number needed to treat was 14.74 (prevention of 15 transfusions required to “avoid” one death). Radial access halved the transfusion rate. After adjustment for all variables, radial access was associated with a significant reduction in 30-day and 1-year mortality, odds ratio = 0.71 (95% CI 0.61 to 0.82) and 0.83 (0.71 to 0.98), respectively (all p<0.001).
Conclusions: In a registry of all comers to PCI, transradial access was associated with a halving of the transfusion rate and a reduction in 30-day and 1-year mortality.
Statistics from Altmetric.com
Both large randomised controlled studies and numerous elective and acute coronary syndrome registries have demonstrated that major bleeding and transfusion after percutaneous coronary intervention (PCI) are associated with increased in-hospital and 1-year mortality.1–9 Despite the mounting data, the interventional community remains slow to focus on strategies to minimise bleeding. The extent of the problem is not well recognised and a commonly held belief is that only patients with high morbidity are at risk.10 More than two-thirds of bleeds are attributable to complications at the femoral access site with retroperitoneal, gastrointestinal and intracerebral sources the minority.2 8 11 Indeed, a femoral haematoma requiring transfusion is an independent predictor of 1-year mortality.8 Potential strategies to reduce bleeding include improved puncture technique; more individually tailored and monitored anticoagulant and antiplatelet treatments and alternative arterial access. Transradial PCI has been shown to reduce dramatically transfusion related to the access site, although lower historical procedural success rates and a more technically demanding procedure, coupled with a natural resistance to change, have made use of this approach still a minority world wide.12–14 In this study we link three large prospectively collected multicentre provincial databases to investigate the association between the arterial access site used for coronary intervention and transfusion rates, 30-day and 1-year mortality.
METHODS
Data linkage
The Canadian province of British Columbia has a population of four million served by a single tiered medical system. Data entry into the British Columbia Cardiac Registry (BCCR) has been mandatory for all PCIs since April 1994. Prospectively collected data are acquired from four clinical centres through structured data sheets completed in the catheterisation laboratory after each procedure and entered into a central database maintained by a dedicated management team. Vital statistics data are automatically entered into the BCCR from the provincial Vital Statistics database.
The Central Transfusion Registry (CTR) was developed in 1998 by the Provincial Blood Coordinating Office and prospectively catalogues all blood products transfused.
All residents of British Columbia undergoing PCI between 1 January 1999 and 30 December 2005 were eligible. The study was approved by the ethics committee of the University of British Columbia. Patients were linked to the CTR database to identify those patients who received at least one packed red cell transfusion within 10 days of PCI, consistent with previous studies.2
The patient matching between CTR and the BCCR was done by personal health number only and a second pass was based on last name, first name, middle name and birth date fields. Of the 32 824 distinct patient PCI procedures, the transfusion status was identified in 32 822, which were used for analysis.
Of the 32 822 patients in the cardiac registry tables, 5231 (16%) patients were also in the CTR database. Only packed red cell transfusions given within 10 days of the PCI procedure date were included, giving 1134 (3.5% of total) transfusion events. A total of 6341 units were transfused to these 1134 recipients during 1145 procedures. An “end date” field for each PCI was created to avoid double counting the same blood product for patients with multiple procedures within 10 days. If a patient had multiple procedures on the same date then only the last procedure of the day was used. The format of the CTR/Cardiac Registry was an encrypted Access database (Microsoft).
Patients receiving coronary artery bypass grafting (CABG) within 10 days of PCI were then further excluded from the dataset as transfusion events were assumed to be attributable to CABG. Of 39 386 PCI procedures (in 32 822 patients) within the study period, 311 procedures were excluded for proceeding to CABG. A further 80 procedures were excluded where the access site was either brachial (43 patients) or not entered (37 patients) and 123 procedures were excluded because the patient had another procedure later that day, leaving a total of 38 872 PCI procedures for analysis (fig 1).

Data collection
Data on each patient were collected in the following categories: demographics, medical history and cardiac risk factors, primary indication for PCI, procedure access site, transfusion status (yes/no) and 30-day and 1-year mortality. Information on congestive heart failure, adjunct pharmacotherapy and vascular closure devices was not sufficiently well collected for robust analysis.
Statistical analysis
Continuous variables are expressed as means, and categorical variables summarised as percentages. Means of clinical variables, demographics, transfusion outcome and 30-day and 1-year mortality outcomes were compared using two-sample t tests with equal variances. Missing values were imputed using switching regression.15 Of the 38 872 PCI procedure records, all variables were available for 22 080 procedures. Ninety per cent of the records with missing values had complete information on all but one or two variables. In 353 cases the imputation of body mass index generated a value <15 or >50. In each case, the imputed value was replaced by the cut-off value. Logistic regression was used to control for differences in all medical history and cardiac risk factors reliably recorded in the BCCR. A probit regression model was used to find the risk difference associated with transfusion after controlling for the same medical history and risk factors.
Standard errors were adjusted for correlation between observations resulting from multiple observations per person. In addition, a propensity score matching analysis was performed where stated. Survival curves were generated by the methods of Kaplan–Meier. All calculations were performed using Stata SE9. Imputation was done using ICE.16 All statistical tests were two-tailed, and a significance level of 0.05 was used throughout.
RESULTS
Table 1 describes the clinical variables split by association with access site. Differences between the radial and femoral cohorts achieved statistical significance for most clinical variables. An exception was the split of patients with stable angina and acute coronary syndrome, which showed equivalence. Table 2 presents the raw outcome data, transfusion status (yes/no), 30-day and 1-year mortality and association with access site and transfusion. Figure 1 illustrates the breakdown of procedures by access site, transfusion status (yes/no) and 30-day and 1-year mortality. Raw unadjusted 30-day and 1-year mortality rates differed in the radial and femoral cohorts in both the transfused and non-transfused groups (fig 1). Although 1-year mortality was higher in the non-transfused femoral versus radial cohorts (3.4% vs 2.5%), this was not statistically significant after adjustment for all the variables in table 1 (p = 0.1).
One of the four clinical centres accounted for just under 90% of the radial procedures. Each of the four centres had six experienced operators and performed about 2000 PCIs a year (300–350 for each operator). The centres cover different catchment areas within the geographically large Province of British Columbia. For case-mix comparison, the catheter laboratory directors reported their activities (table 3).
Association of transfusion with 30-day and 1-year mortality
Logistic regression
Of the 38 872 PCI procedures in 32 519 patients in British Columbia January 1999 to December 2005, 2.5% received transfusions and 97.5% did not receive transfusions. There were 12.6% and 22.9% deaths in the transfused group at 30 days and 1 year, compared with 1.3% and 3.2% deaths in the non-transfused group, respectively (table 2).
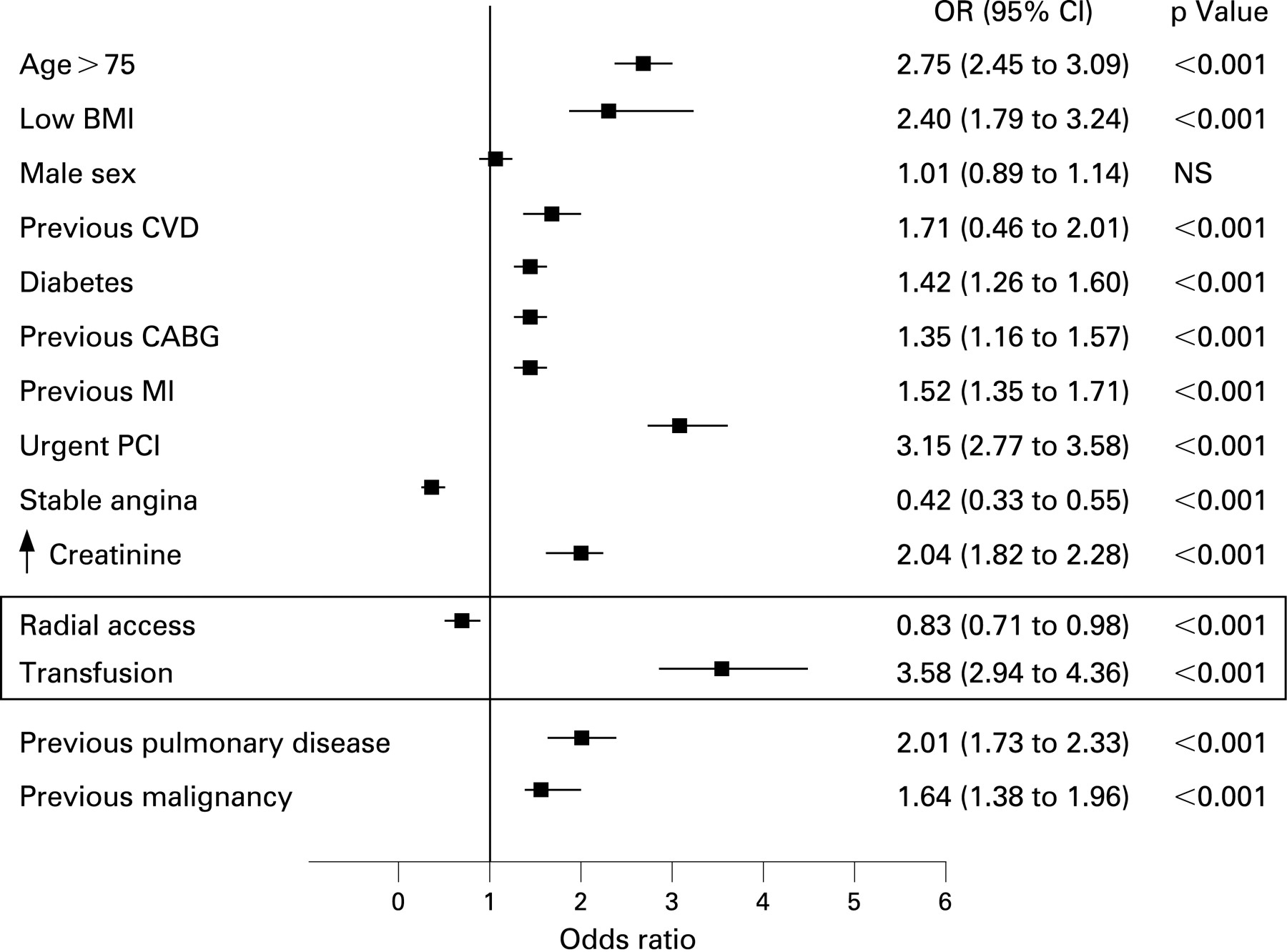
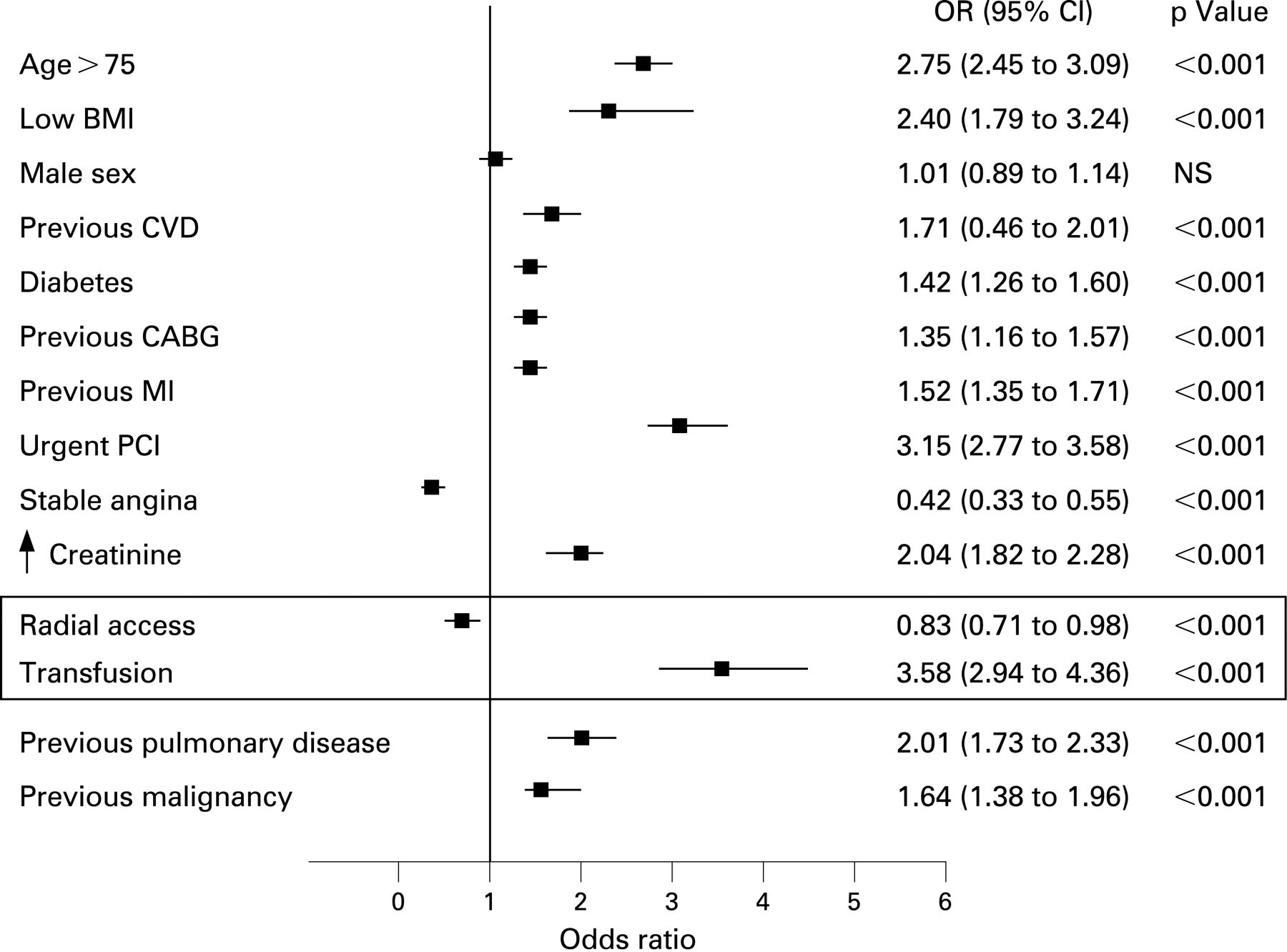
Unadjusted odds ratios of association of receiving a transfusion with 30-day and 1-year mortality were 11.35 (95% CI 9.20 to 14.01) and 8.94 (95% CI 7.61 to 10.5), all p<0.001. Adjusted odds ratios (for all variables in table 1) of association of receiving a transfusion with 30-day and 1-year mortality were 4.01 (95% CI 3.08 to 5.22) and 3.58 (95% CI 2.94 to 4.36), all p<0.001 (fig 2).
By probit regression the absolute increase in risk of death at 1 year (adjusted risk ratio (ARR)) associated with receiving a transfusion is 6.78%. The number needed to treat (NNT) is 14.74 (prevention of 15 transfusions required to “avoid” one death). Transfusion is associated with a significant increase in risk of 30-day and 1-year mortality. Figure 3 shows the Kaplan–Meier survival curves for transfused and non-transfused patients.

{kind=link}
{kind=link}
{kind=link}
Propensity score matching
We drew a propensity score matched comparison group for patients who had a transfusion from patients who had not had a transfusion, but were, on average, identical in all measured characteristics within the dataset. We had 967 patients who had received a transfusion. We were able to draw a matched comparison group for 457 (47.3%) of them (in effect limiting the study population to 914 matched patients). The matched groups passed the tests for similarity of observed characteristics, p = 0.96.
Thirty-five (7.7%) of the 457 transfusion patients died within 30 days compared with nine (2.0%) of the comparable 457 non-transfusion patients. (ARR = 5.7%, NNT = 18; risk ratio = 3.9, 95% CI 1.89 to 8.0)
At 1 year 88 (19.3%) of the 457 transfusion patients had died compared with 26 (5.7%) of the comparable 457 non-transfusion patients. (ARR = 12.5%, NNT = 7.4; risk ratio = 3.38, 95% CI 2.22 to 5.14)
Transfusion is significantly associated with increased mortality at 30 days and 1 year, adjusting for all the risk factors for which we have data.
Impact of radial versus femoral access on transfusion rate
Of the 38 872 PCI procedures femoral access was used in 79.5% of procedures. Of these 2.8% were followed by transfusions within 10 days. Radial access was used in 20.5% procedures and 1.4% of those procedures were followed by transfusions within 10 days (fig 1, table 2).
The unadjusted odds ratio of association of receiving a transfusion with radial access compared with femoral access was 0.48 (95% CI 0.39 to 0.59), p<0.001.
The adjusted odds ratio (for all variables in table 1) of association of receiving a transfusion with radial access compared with femoral access was 0.59 (95% CI 0.48 to 0.73), p<0.001. Transfusion rate was halved in radial compared with femoral access.
Impact of radial versus femoral access on 30-day and 1-year mortality
There was 1.7% 30-day mortality after femoral procedures and 3.9% mortality at 1 year. The 30-day mortality after radial procedures was 1.0% and 2.8% at 1 year (table 2).
The unadjusted odds ratios of association of transradial access compared with femoral access with 30-day and 1-year mortality were 0.58 (95% CI 0.45 to 0.73) and 0.64 (95% CI 0.49 to 0.82) respectively, all p<0.001.
The adjusted odds ratios (for all variables in table 1) of transradial access compared with femoral access with 30-day and 1-year mortality were 0.71 (95% CI 0.61 to 0.82) and 0.83 (95% CI 0.71 to 0.98) respectively, all p<0.001. Radial access is associated with a significantly lower risk of 30-day and 1-year mortality. If only non-transfused procedures are analysed, the difference becomes non-significant, consistent with the hypothesis that the mortality difference might be driven by the outcomes for transfused patients. Figure 3 shows Kaplan–Meier survival curves for radial and femoral access. Figure 2 illustrates the adjusted odds ratios for the association of different variables with 1-year mortality.
DISCUSSION
The principal findings of this study are a reduction in 30-day and 1-year mortality associated with a halving of transfusion rate using transradial instead of femoral access in all comers to PCI. We confirm transfusion status as an important independent predictor of 1-year mortality1-8 10 17 and support the suggestion that safety and bleeding concerns should move to the forefront of the PCI agenda.18
A lower rate of transfusion after transradial access has been shown previously in small studies12 13 because the radial artery is smaller and more readily compressible. Although we do not have data on bleeding and use transfusion as a surrogate, we propose that this difference probably reflects reduced access site complications. Furthermore, a femoral haematoma requiring transfusion after PCI independently predicts 1-year mortality.8
We now present the first data to support the hypothesis that radial access, with a proven lower incidence of access site related bleeding and transfusion, may be associated with a reduction in mortality, independent of other major outcome predictors. The high mortality rates in transfused patients are highly consistent with the results of Kinnaird et al, who reported 22.7% mortality in patients with major bleeding and transfusion after PCI.2 We must be mindful that these data are retrospective and non-randomised and therefore serve generate a hypothesis rather than proving the concept. By adjusting for all variables for which there were reliable data we have controlled for any differences in risk between the femoral and radial cohorts which might otherwise account for the observations. Nonetheless, unknown confounders of risk difference between the radial and femoral cohorts may persist. Consistent with this we observed a trend towards reduced mortality favouring radial access in the non-transfused patients, although statistical significance was only achieved when transfused patients were included.
Our data do not allow us to show whether reduced bleeding alone (without transfusion) may be the cause of some of this difference. Consistent with the published data showing that two-thirds of major bleeding requiring transfusion after PCI is directly attributable to femoral access site complications,2 5 11 radial access in our study halved the transfusion rate. Transfusion related to chronic disease state or non-access site related bleeding, including spontaneous retroperitoneal, intracerebral or gastrointestinal bleeding, will not be influenced by choice of access site but continues to challenge us to develop safer antithrombin and antiplatelet protocols.
By limiting our data capture to transfusion after index PCI, we have aimed to exclude, at least in part, “top-up” transfusions for comorbid anaemia which might be preferred where possible before PCI. Other authors have suggested that access site related transfusion approaches zero in transradial cases,12 hence we can postulate that the 1.4% transfusion rate in our radial cohort reflects on the whole the baseline incidence of these other indications for transfusion. We were unable to assess the impact of femoral access closure devices owing to insufficient data capture, although current meta-analyses suggest no reduction or even increased bleeding complications with their use.19–21
Similarly, data within our registry were insufficient to analyse adjunct pharmacology, in particular glycoprotein IIb/IIIa inhibitors which exacerbate access site bleeding.22 However, we were able to control for urgency of procedure: emergency or elective, stable angina/acute coronary syndrome and diabetes, which incorporate the clinical indications for elective glycoprotein IIb/IIIa use, and it would be reasonable to assume that procedural bail-out indications such as side-branch loss or no-reflow were independent of arterial access.
In addition glycoprotein IIb/IIIa use across the four centres was reported as comparable. Bivalirudin use, proved to reduce bleeding end points, was only significant (20%) in one femoral centre. By our number needed to treat analysis of the impact of transfusion on mortality, we propose that prevention of 15 transfusion events is required to “avoid one death”. It might be speculated, therefore, that at the incidence of transfusion in our study for each approach, 2.8% femoral, 1.4% radial (which are modest in comparison with other studies citing incidences of 5–16%2 4 6), we might prevent three transfusions per 200 PCIs. This yields an approximate speculative figure of one life potentially “saved” per 1000 PCIs by adopting radial access. This is too small to be detected in the practice of a single operator or institution but can be reviewed in the context of national or global figures—for example, 2.2 million PCIs world wide in 2004.18 Similarly, the next logical step of a randomised prospective comparison of radial versus femoral would require huge numbers for adequate power to detect a difference of one per thousand with a mortality rate of 3%, although studies with 30-day end points are recruiting patients.
Candidate mechanisms linking bleeding to adverse outcome include haemodynamic compromise, induction of hyperadrenergic or inflammatory state and enforced cessation of thrombotic agents. With respect to transfusion strategy, there is evidence from the critical care setting that a low threshold for transfusion may worsen outcome, implicating liberal transfusion (in addition to the bleeding itself) as part of the problem.23 24 In a study by Rao et al transfusion was independent of bleeding and haematocrit nadir in predicting 30-day mortality.9 This may in part be because of altered characteristics of older stored blood such as reduced oxygen delivery, nitric oxide depletion or stimulation of inflammation, immune modulation and vasoconstriction.25–28 Rao et al demonstrated in trial populations that blood transfusion was associated with worse survival when given to patients with nadir haematocrits >25%.9 Sabatine et al further demonstrated in trial populations with acute coronary syndrome that transfusions were associated with more recurrent ischaemia and worse survival across all haemoglobin levels.29 Intriguingly, also, red cell contamination is a negative predictor of outcome after autologous stem cell therapy for myocardial infarction.30
Given the growing evidence of the importance of reducing PCI-related bleeding and transfusion, radial access is one factor to be considered in the strategy alongside adjunct treatments, smaller catheters and more judicious transfusion thresholds.
Limitations
The data are retrospective and non-randomised and dependent on statistical methods to control for differences between the radial and femoral cohorts, which were statistically significant for most clinical variables. Although the radial cohort was older and had more emergency procedures, the femoral cohort may have contained more high-risk patients as they had more diabetes, comorbidities, prior procedures and infarcts, and renal disease. Although a strength of the study is the huge number of patients and procedures, even minor differences in demographics become highly statistically significant (table 1) and caution should be used in drawing comparisons. This made statistical analysis a challenge to control for known and unknown differences in the groups. If patients who had received a transfusion are excluded from the analysis, the adjusted mortality difference between radial and femoral becomes non-significant (p = 0.1). Possible confounding factors include ejection fraction, adjunct pharmacologies and also case mix and practice between the centres.
The majority of radial cases were performed in one of the contributing centres making it important to highlight and control, where possible, for differences in practice between centres. Although the catheter laboratory directors’ data demonstrate reasonable uniformity in case mixes across the radial and femoral centres, local unknown differences in practice or referral patterns—for example, numbers of trainee operators or referral after recent diagnostic puncture, remain potential confounders.
We were unable to study the impact of femoral vascular closure devices and pharmacotherapies as these were insufficiently entered in the database. Additionally, procedural variables, such as sheath sizes, time to sheath removal and peri-procedural activated clotting times, were not captured by this registry and they may have been associated with rates of access site complications.
The method of data collection did not allow us to determine reliably the exact reason for transfusion or provide any clinical details of bleeding. Similarly, our data did not capture nadir haematocrits before and after procedure to allow comment on transfusion thresholds within the study. Although the analyses show transfusion to be an independent predictor of death, the degree of contribution to mortality of transfusion is difficult to determine.
A further limitation of this method of anonymous data linkage using procedures as index events rather than patients, is that statistical adjustment was required to adjust for correlation between observations resulting from multiple observations per person.
CONCLUSIONS
In a registry of all comers to PCI, transradial access was associated with a halving of transfusion rate and a reduction in 30-day and 1-year mortality. Although retrospective and non-randomised, these data generate the hypothesis that radial access may be associated with improved outcome after PCI, probably through a reduction in bleeding and transfusion. These data require confirmation by other large registries and randomised prospective trials.
Acknowledgments
We acknowledge the contributions of Dr Richard Mildenberger, Dr Gerry Simkus, Dr Anthony Fung and Dr John Webb, catheter laboratory directors of the contributing centres. In addition, we thank Dr Dewy Evans, formerly of the BCCR, and Dr Gayle Shimokura of Providence Health Care, for data collection.
REFERENCES
Footnotes
-
Competing interests: None.
-
Funding: The project was funded by Victoria Heart Institute Foundation. Dr Chase’s fellowship was supported by an unrestricted educational grant from Boston Scientific Corporation.
-
WPW is principal custodian of the data and all authors are responsible for its integrity.
-
Ethics approval: Ethical approval was granted by the University of British Columbia.