Article Text

Statistics from Altmetric.com
Background
‘Time is brain’ is a slogan that has been used by stroke advocacy groups to raise public awareness that stroke is a medical emergency which requires timely treatment.1 Similarly, the acronym FAST (face, arm, speech, time) has been advertised as an easy way to remember the most common stroke symptoms and the need to act quickly.2
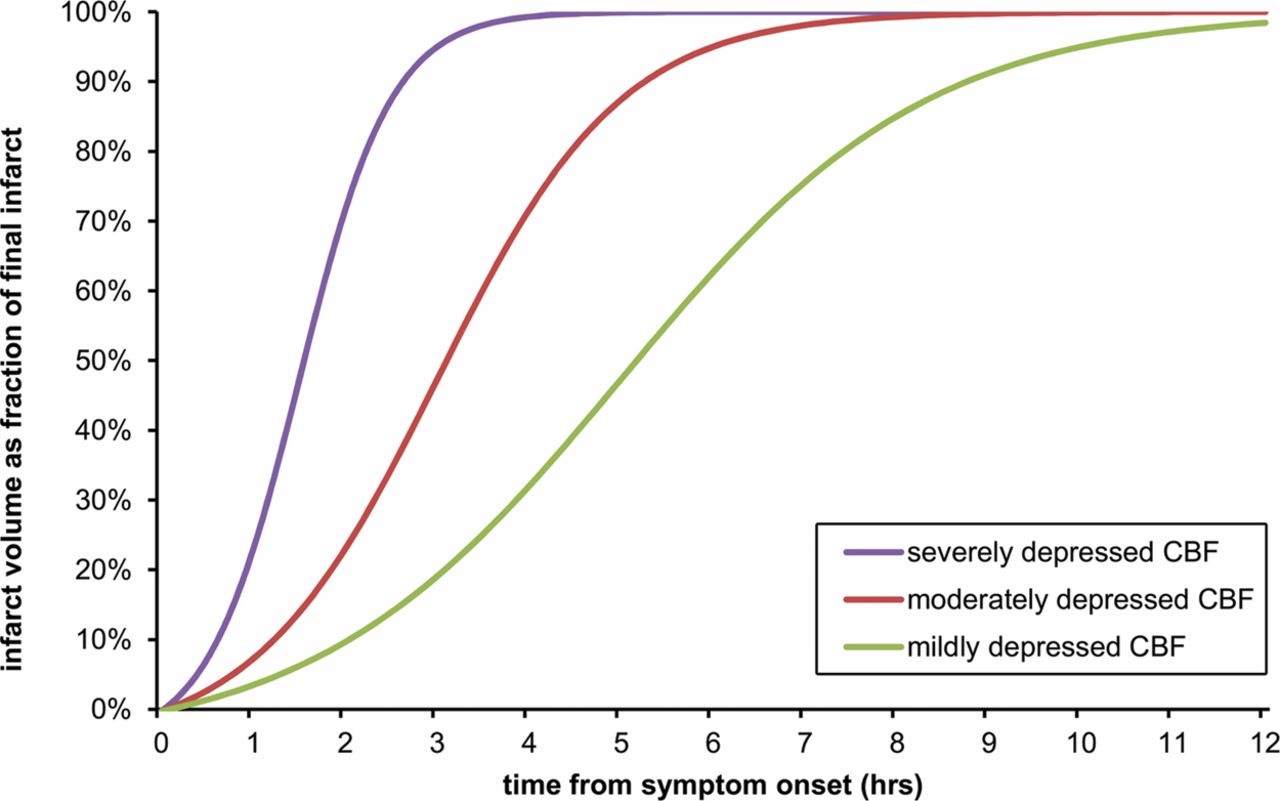
The time dependent nature of brain injury following an ischemic event has been characterized in animal experiments. Early studies have shown that brain tissue gradually undergoes irreversible damage following an acute ischemic stroke. These studies suggest that infarct growth can be described by a logarithmic or a sigmoidal function. The rate at which tissue transitions from reversible to irreversible injury is dependent on the depth of the ischemia; with mild reductions in cerebral blood flow, brain tissue remains viable for a relatively long duration, whereas cerebral injury becomes irreversible rapidly when cerebral blood flow is severely impaired (figure 1).3 ,4 Another factor that determines the rate at which tissue undergoes irreversible ischemic injury is the type of tissue that is involved. For example, gray matter, which has a higher metabolic demand, is more susceptible to ischemia than white matter.5 The average rate of neuronal loss in humans is estimated to be 1.9 million neurons per minute during the first 10 h after stroke onset.1 These data indicate that stroke treatments aimed at restoring blood flow are most effective when they are initiated early.

{kind=link}
Schematic representation of infarct volume evolution. A schematic representation of the evolution of infarct volume is shown for three hypothetical scenarios: the patient with a severe reduction in cerebral blood flow (CBF) (purple line) experiences rapid expansion of the infarct, which reaches its final volume early; moderate growth is seen in the patient with a moderate reduction in CBF (red line); and slow infarct growth is observed in the patient with a relatively mild reduction in CBF (green line).
Time to treatment and intravenous thrombolysis
The most convincing human data to support the notion that ‘time is brain’ stem from the clinical trials that tested the use of intravenous tissue plasminogen activator (tPA) for patients with stroke. The first positive trial of intravenous tPA restricted enrollment to patients in whom treatment could be initiated within 3 h, with 50% receiving treatment within 90 min.6 In contrast, three other trials (European Cooperative Acute Stroke Study (ECASS) I, II and Alteplase ThromboLysis for Acute Non-interventional Therapy in Ischemic Stroke (ATLANTIS)), which were similar in design but allowed treatment up to 6 h and 5 h, respectively, failed to show a benefit of intravenous tPA.7–9 A pooled analysis of all major intravenous tPA trials has demonstrated a gradual decline in the OR of benefit from tPA with longer times from symptom onset to treatment.10 The pooled data from these studies were also used to estimate the number of patients needed to treat (NTT) with tPA to benefit one patient and the number of patients needed to treat to harm (NNH) one patient.11 The approximate number of patients needed to treat to have one patient experience a net benefit (ie, NTT adjusted for NNH) was four for treatment started within 90 min, five for treatment between 90 and 180 min, 7.5 for treatment between 180 and 270 min, and infinity for treatment beyond 270 min.11
Based on the results of these pooled analyzes, a trial was designed to test the hypothesis that treatment with intravenous tPA within the 3–4.5 h time window is beneficial. This study, ECASS III, was published in 2008 and confirmed that tPA treatment in the 3-4.5 h time window is associated with an increased odds of an excellent outcome (OR 1.34; 95% CI 1.02 to 1.76).12
Taken together, the data from trials of intravenous tPA clearly demonstrate that time is of the essence in acute stroke therapy, and that delays in initiating intravenous tPA treatment increase the number of patients who are ‘treatment failures’.
Time to treatment and endovascular therapy
Despite significant improvements in the devices and techniques used for endovascular treatment of acute stroke, the clinical outcomes of patients treated with endovascular therapy remain marginal.13–15 Good functional outcome after endovascular treatment depends on multiple factors. Time is one factor that likely plays an important role in the outcome of these patients.16–18
Similar to the data for intravenous tPA,19 ,20 the endovascular literature has shown that shorter times (imaging to puncture, imaging to recanalization, symptom onset to puncture, and symptom onset to recanalization) correlate with increased chances of a good outcome.16–18 A post hoc analysis from the Interventional Management of Stroke (IMS)-I and II studies, including 54 patients with middle cerebral artery or distal internal carotid artery occlusions who underwent successful intra-arterial recanalization (Thrombolysis in Cerebral Infarction score 2–3), showed that time to angiographic recanalization was an independent predictor of good clinical outcome. Interestingly, the authors noted that after 7 h, the probability of good clinical outcome was similar in cases with and without angiographic reperfusion. The authors concluded that good clinical outcome following successful endovascular treatment is time dependent (a 30 min delay in achieving successful reperfusion decreased the probability of good functional outcome by 10%).16 Sun et al17 compared the imaging characteristics, treatment times and outcomes of patients treated with intra-arterial therapy who were transferred from outside hospitals (n=132) to patients who presented locally (n=58). Transferred patients had less favorable ASPECTS (Alberta Stroke Program Early CT Score), longer imaging to puncture times (205 vs 89 min) and worse clinical outcomes (modified Rankin Scale score 0–2 in 29% vs 51%). Shorter imaging to puncture times were independently associated with good outcomes in a logistic regression model.17 The SWIFT (Solitaire FR With the Intention For Thrombectomy) trial demonstrated that the Solitaire flow restoration device achieved substantially better angiographic, safety, and clinical outcomes than did the Merci retrieval system.15 A subanalysis of the data revealed that the times from symptom onset to puncture were shorter in the Solitaire arm compared with the Merci arm (293 min vs 319 min) as was the median time from initial placement of guide catheter to achievement of recanalization or end of procedure (36 min vs 52 min). These shorter times, in combination with the higher recanalization rates from Solitaire, may have led to the better outcomes of patients randomized to treatment with the stent retriever.15 It has also been suggested that high volume endovascular stroke centers have faster times to treatment which may lead to higher rates of good clinical outcomes in these centers.18 In a retrospective multicenter review of 442 patients who underwent intra-arterial treatment, median time from CT to puncture was 96 min and median total procedure time was 95 min. Eighty per cent of patients who had short CT to puncture times (less than 95 min) were treated at high volume endovascular stroke centers (centers that treat >50 intra-arterial stroke cases/year), and patients treated at high volume centers were more likely to have good clinical outcomes.18
The recently published IMS-III study failed to show improved functional outcomes in patients treated with intravenous tPA plus endovascular therapy compared with intravenous tPA alone; interestingly, the time to endovascular treatment was over 30 min longer than in IMS-I, and the authors suggest that this may be an important reason for the lack of clinical benefit.14 A secondary outcomes analysis of the IMS-III trial showed a trend towards better outcomes in patients with intravenous tPA to groin puncture times under 90 min compared with patients with times exceeding 90 min but the difference was not significant. Another recent trial compared intravenous tPA with endovascular treatment within 4.5 h after symptom onset. This trial failed to show benefit of endovascular therapy which may, in part, be explained by a 60 min delay in time to treatment in the endovascular group compared with the intravenous tPA group (3.75 h vs 2.75 h; p<0.001).13
In other studies, the relationship between shorter times and improved outcome have been less clear.21 ,22 Nogueira et al21 evaluated the relationship between time to treatment and independent outcomes in the MERCI (Mechanical Embolus Removal in Cerebral Ischemia) and Multi-MERCI cohorts and found no association. Analyzes of the PROACT (Prolyse in Acute Cerebral Thromboembolism) II data also demonstrated that time to randomization and time to treatment were not strongly associated with outcome or treatment effect. The ability to detect this relation in this cohort, however, is limited as treatment was initiated around the same time (between 5 and 6 h) in most patients.22
Tissue clock versus time clock
Patients who are most likely to benefit from revascularization have a relatively small region of permanent ischemia (infarct cores) and a relatively large region of reversible ischemic injury (penumbra).23 ,24 Because of the inverse relationship between duration of cerebral ischemia and penumbral volume, time to treatment can be used as a surrogate for the presence of penumbral brain tissue. Time to treatment is, however, not a perfect surrogate as the rate at which penumbral tissue undergoes irreversible injury is dependent on multiple variables and therefore varies among patients. For example, patients with good collaterals and relatively modest reductions in cerebral blood flow continue to have penumbral tissue many hours after stroke onset whereas patients with poor collaterals and severe reductions in cerebral blood flow may lose all penumbral tissue within the first few hours.
Because time is an inaccurate estimate for the presence of penumbral tissue, patient selection may be improved by the use of imaging techniques that can visualize the ischemic penumbra directly. This has been referred to as the use of a tissue clock for patient selection. The use of a tissue clock could identify patients with good collaterals who are outside the established time window for intravenous tPA, but who may still benefit from reperfusion therapy based on the presence of penumbral tissue.25 Stroke patients with a significant volume of penumbral tissue are often referred to as patients with a ‘mismatch’ between the volumes of their ischemic core and hypoperfused tissue. Both MRI and CT perfusion criteria have been proposed to identify patients with a mismatch.26–33
The Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution (DEFUSE) study and the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET) have provided evidence that image based patient selection is promising.26 ,34 DEFUSE was a prospective cohort study of intravenous tPA in the 3–6 h time window, and EPITHET was a randomized controlled trial of intravenous tPA in the same time window. Patients enrolled in these studies showed improved clinical outcomes with reperfusion if a mismatch was present whereas patients without a mismatch did not appear to benefit from reperfusion.35 Similarly, DEFUSE 2 has demonstrated a differential response associated with endovascular reperfusion depending on the presence of a perfusion–diffusion mismatch on MRI.36
The negative results of IMS-III and SYNTHESIS Expansion could, in part, be explained by inclusion of a heterogeneous patient population which likely included a relatively large proportion of patients who lacked an adequate amount of penumbral tissue. Both studies allowed inclusion of patients primarily based on a treatment time window only. Additional inclusion criteria that require the presence of penumbral tissue on MR or CT imaging could have led to a more homogeneous population of patients who are more likely to benefit from revascularization. This concept was tested in MR RESCUE (Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy),37 a randomized controlled trial of endovascular therapy that prespecified imaging criteria to identify patients with an ischemic penumbra. This study failed to show benefit from endovascular therapy in both patients with and without mismatch.37 A combination of imaging selection criteria which allowed the inclusion of patients with relatively large ischemic cores and relatively low rates of revascularization with endovascular intervention may have contributed to these negative results.
Conclusion
Reperfusion therapy is only effective in the presence of a significant volume of penumbral tissue. Because the penumbra diminishes over time, reperfusion therapy for acute stroke is most effective when administered early. However, because infarct evolution varies among patients, time is an inaccurate surrogate for the presence of penumbral tissue. Reperfusion therapy is therefore most effective when it is initiated at the earliest possible time in patients with documented evidence of penumbral tissue.
References
Footnotes
-
Contributors Both authors contributed substantially to this work.
-
Competing interests None.
-
Provenance and peer review Commissioned; not externally peer reviewed.