Article Text

Statistics from Altmetric.com
We thank the Editors of JNIS for alerting us in advance to the concerns about SELECT2 raised by Jadhav1 and colleagues and appreciate the opportunity to explain the rationale for the study design and clarify the benefits of including perfusion imaging-based selection criteria. We are confident that SELECT2 will provide high-level, reliable data regarding the safety and efficacy of endovascular thrombectomy (EVT) for large core patients.
The choice of imaging modality for identifying large core in acute ischemic stroke remains an area of considerable debate. Magnetic resonance imaging (MRI) diffusion-weighted imaging (DWI), computed tomography (CT) or MR perfusion imaging and Alberta Stroke Program Early CT Score (ASPECTS) have all been proposed and studied. At present, there is no clear consensus on which imaging modality is best for identifying patients with large core. It is important to recognize that the early window randomized EVT trials used a broad range of imaging selection criteria. The imaging selection criteria for the initial five pivotal trials ranged from allowing patients to be enrolled regardless of the degree of early infarct signs,2 to studies that required a specific ASPECTS score range in addition to other imaging criteria,3–5 to EXTEND IA6 where the ASPECTS score was not considered, and CT perfusion (CTP) mismatch with a maximum estimated core size was required. All five trials were successful but with substantial variability in the treatment effect, leaving uncertainty as to the optimal imaging approach as well as whether there are patient subgroups who do not benefit. In fact, those utilizing perfusion mismatch criteria (EXTEND-IA, SWIFT PRIME) had higher rates of modified Rankin Scale (mRS) scores 0–2 and larger treatment effects, compared with other trials.2–6
Even if a treatment has a clear benefit in most patients, there can be important subgroups that do not benefit or are harmed. The overall study results with all subgroups included can be positive, but important subgroups who should not be treated may exist. Based on well-established pathophysiology of brain ischemia, we believe that the subgroup of large core patients who are most likely to benefit from EVT are those who continue to have penumbral tissue at the time of the procedure. The subgroup that is least likely to benefit are patients who have competed their infarct and no longer have any penumbral tissue. Multiple studies have suggested that about 15% of early window large vessel occlusion patients may have a completed infarct due to very poor collaterals7–9 and these patients are the most likely to present with a large core. The design of SELECT2 is unique – and in our opinion offers important advantages in that it will allow assessment of the heterogeneity of EVT treatment effects in patients with large core on CT by assessing their ischemic core volumes on perfusion imaging, which has increasingly become part of the diagnostic algorithm for stroke patients on arrival to the hospital.10 This design will allow for a randomized assessment of whether perfusion imaging in large core patients provides additional data that influence the safety and efficacy of thrombectomy.
Accuracy of CTP
Concern was raised that CTP does not provide a reliable estimate of the ischemic core, with the particular concern about misidentification of patients who may not actually have a large region of irreversible injury. The accuracy of CTP for estimating the size of the core can vary depending on a number of parameters including the time between stroke onset and imaging and the imaging parameters used to acquire the perfusion imaging and the software chosen to analyze the data. Use of a standardized CTP acquisition at the study sites and the use of a validated software platform (RAPID, iSchemaView) helps to reduce this variability within the SELECT2 study. An independent study from Kiel11 that compared CTP software programs for accuracy showed that the perfusion software included in SELECT2 was more accurate than other programs for estimating ischemic core, with a substantially lower incidence of core overestimation. In addition, multiple studies have shown good performance in core estimation, without significant overestimation, when using the same perfusion software used in SELECT2.4 7 12 13 For example, in SWIFT PRIME, core overestimation was rare and when it occurred the median volume was only 4 mL.14 Furthermore, in a pooled analysis of data from HERMES and EXTEND-IA TNK using the same software as the one used in SELECT2, the median difference between the CTP estimated ischemic core volume and the diffusion lesion volume at 24 hours was 4.4 (IQR 1.2–12.0) mL and “volumetric CTP core overestimation was uncommon”.15 Only one of the studies cited by Jadhav et al suggesting CTP is not accurate for estimating core used the perfusion software we are using in SELECT2 and that study found that only 16% had core overcall of 10 mL or more using follow-up CT (rather than MRI which is more sensitive for estimating infarct volume).16 The authors of this study concluded “CBF <30% may overestimate infarct core volume, especially in patients imaged in the very early time window and with fast complete reperfusion”. We agree that recent evidence has demonstrated that cerebral blood flow (CBF) <30% is not the optimal threshold for estimating core in patients imaged within 90 min of stroke onset17 18 and recently implemented a plan to address this in SELECT2 by using the <20% threshold in patients imaged within 2 hours from last known well (LKW). Additionally, perfusion imaging may be more accurate than an ASPECT score threshold to differentiate patients with salvageable tissue from those with a completed infarct because it estimates not only the core but also the penumbra (mismatch). Multiple studies have demonstrated that patients without a mismatch do not have a favorable clinical response to reperfusion.7 9 13 19 20 Based on these differing positions in the field regarding the benefit of CTP for patient selection, there exists scientific equipoise, and thus the need for a randomized trial such as SELECT2 to help address this question.
Benefit of EVT in favorable ASPECTS, large CTP core – not so “indisputable”
Concern was raised that patients with favorable ASPECTS and a large CTP core have already been proven to benefit from EVT with “indisputable and unequivocal evidence”. We do not agree. Let us review the data here.
The early window clinical trials typically did not enroll sufficient patients with large core on perfusion imaging. Indeed, the vast majority of the patients in the HERMES meta-analysis had very small cores as shown in figure 1, and very few with an ischemic core >50 mL.13 Thus, the retrospective analyses that have been performed on this limited database are underpowered to evaluate this subgroup and cannot be interpreted as providing a high level of evidence.
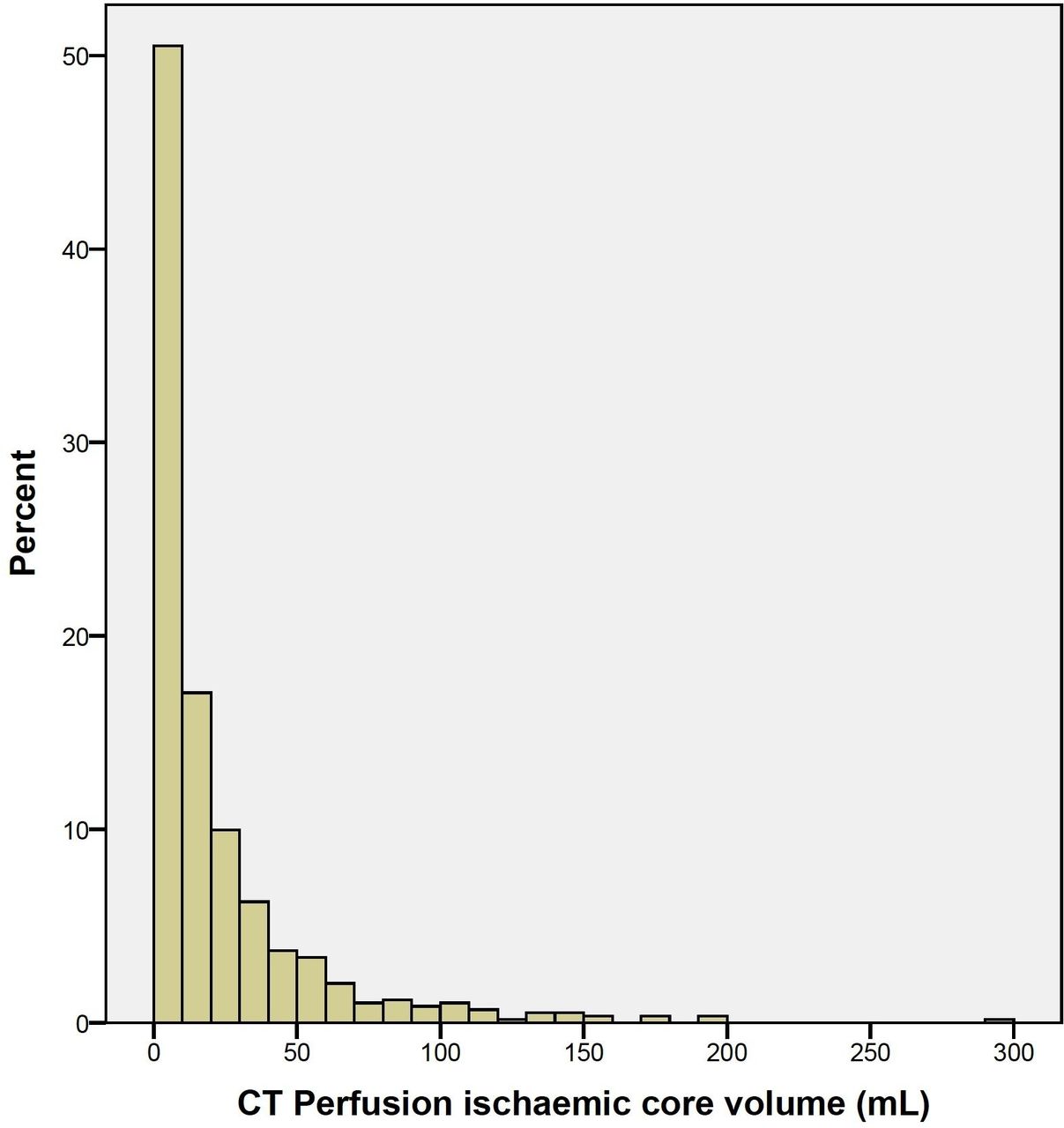
Distribution of ischemic core volume using relative cerebral blood flow (rCBF) of <30% threshold in patients included in the HERMES meta-analysis who received computed tomography (CT) perfusion, showing limited number of patients with core volume with >50 mL, and a vast majority of the patients have ischemic core volume <50 mL. Reprinted with permission from Elsevier. All rights reserved.
In HERMES, of 50/591 (8.4%) patients who had ischemic core of 70 mL or higher on CTP, there were imbalances in baseline ASPECTS (thrombectomy 8 (6–9) vs medical management 5 (4–7), P=0.001) and ischemic core volumes (85 (74–108) mL vs 110 mL (86–137) mL, P=0.12) in favor of EVT, potentially confounding analyses in this subpopulation.13 Furthermore, at least half of the 25 patients who received medical management demonstrated an ASPECTS of 4–5, suggesting a significant concordance between CT and CTP imaging in the early window, which suggests that a large CTP core in ASPECTS 6–10 patients is uncommon. In addition, among the small population of HERMES patients who did not have a perfusion mismatch, “these patients had no functional improvement from endovascular treatment (cOR 0.87 (95% CI 0.20 to 3.81), P=0·85)”.13 These wide confidence intervals suggest that EVT outcomes could be 4–5 times better or worse than medical management.
SELECT2 was designed based in part on the data from the first SELECT study. Institutional review board approval was obtained from all participating centers in SELECT and all patients or their legally authorized representatives provided informed written consent prior to participation. In SELECT, of 285 patients receiving EVT, 197 presented with ASPECTS 6–10 on non-contrast CT within 6 hours of last known well. Some 173 (88%) of these patients demonstrated an ischemic core of <50 mL on CTP imaging, whereas 24 (12%) had an ischemic core of ≥50 mL. The distribution of the mRS scores at 90 days in these patients is provided in figure 2.

Distribution of functional outcomes as measured by modified Rankin Scale (mRS) scores obtained at 90-day follow-up in SELECT trial patients who presented within 6 hours of last known well with computed tomography (CT) ASPECTS of 6–10, stratified by ischemic core volume (relative cerebral blood flow (rCBF) <30%) on CT perfusion.
Despite a favorable ASPECTS score, patients who presented within 6 hours with an ischemic core of 50 mL or larger demonstrated significantly less functional independence (26% vs 58%, P=0.003) and greater mortality (48% vs 9%, P<0.001), symptomatic intracerebral hemorrhage (ICH) (17% vs 5%, P=0.038), and neurological worsening (26% vs 8%, P=0.009) when compared with patients who presented with a favorable ASPECTS and smaller ischemic core. Additionally, the functional independence rate of 26% in the favorable ASPECTS/large core on CTP group in SELECT is similar to the functional independence rate of 26.5% in the control group from HERMES, further supporting equipoise in this patient subgroup.
In addition, there are many examples of studies that randomized a subgroup of uncertain benefit even if that subgroup had been included in a prior randomized study that showed benefit in the total population. For example, the PRISMS study evaluated the efficacy and safety of intravenous thrombolysis in a subgroup of patients who were included in the original NINDS tissue plasminogen activator (tPA) studies.21 Subsequent endarterectomy studies have also identified subgroups that did not benefit, even though they were included in prior positive studies.22
What is the evidence for benefit in patients with CTP core volumes of 50–70 mL in the late time window?
Data from DEFUSE 3 were used to argue that we already have definitive evidence that core volumes of 50–70 mL benefit from late window EVT.23 However, only half of the subgroup they cite with core “larger than DAWN” (n=18) had ischemic core of >50 mL. This analysis reported cOR 20.9 (95% CI 1.3 to 337.8) while adjusting only for age and National Institutes of Health Stroke Scale (NIHSS). This evidence is far from precise or sufficient. Additionally, these data are limited to the 6–16 hour window. The DAWN trial inclusion criteria did not allow patients with core volume >50 mL, thus there is no evidence on these patients beyond 16 hours. The limited evidence for EVT efficacy in early window patients with core volumes >50 mL is described above.
However, we acknowledge that core lesions between 50 and 70 mL are not considered by all to be “large core” and therefore we have prespecified a sensitivity analysis in the statistical analysis plan that assess EVT efficacy and safety with and without this subgroup.
Data regarding patients with low ASPECTS and favorable CTP core volumes
Another group of interest are those with poor ASPECTS but moderate core volumes and significant penumbra. These patients have been shown to have substantial treatment effects in high-quality randomized studies, and some of these patients had ASPECT scores <6.6 12 For example, patients enrolled in DEFUSE 3 with an ASPECTS of 5 had a median core size of 30 mL and large penumbral volumes. In the SELECT EVT group, the median CTP core volume for patients with ASPECTS of 5 was 25 (IQR 14–43) mL. For those with ASPECTS of 4 the median CTP core was 59 (IQR 36–80) mL.24
This subgroup of patients with poor ASPECTS/favorable CTP (that are included in the ongoing ASPECTS-only randomized controlled trials) had higher rates of functional independence and a much better safety profile in SELECT as compared with the good ASPECTS/unfavorable CTP (see figure 3).24

{kind=link}
{kind=link}
{kind=link}
Proportion of functional independence and safety outcomes stratifying by computed tomography (CT) and CT perfusion (CTP) profiles in patients receiving thrombectomy in the SELECT trial. Patients with favorable profiles on both imaging modalities demonstrated the highest functional independence and lowest rates of safety outcomes. Patients with unfavorable CT but favorable CTP demonstrated moderately reduced functional independence with similar safety outcomes to patients with a favorable profile on both imaging modalities. Patients with favorable CT but unfavorable CTP had lower functional independence and high rates of symptomatic intracranial hemorrhage (ICH), neurological worsening, and mortality. Reprinted with permission from John Wiley & Sons, Inc. All rights reserved.
Additionally, a pooled analysis from SELECT and TREVO registry also demonstrated marked variability in outcomes in patients with ASPECTS of 3–5 with differing baseline ischemic core volumes.25 As core volume increased, functional independence decreased, while symptomatic ICH and mortality substantially increased. These findings highlight the heterogeneity of outcomes in patients with large core on CT ASPECTS based on the core volume assessed by perfusion imaging. This point influenced the design of SELECT2: the availability of both CT-based ASPECTS and CTP-based ischemic core volumes will allow for an assessment of EVT treatment effect heterogeneity which is not possible in the studies that only assess ASPECTS. It is plausible, as has already been shown (SELECT+TREVO results), that thrombectomy outcomes in patients with large core based on ASPECTS vary based on their CTP core volumes.
The argument regarding not enrolling patients where treatment benefits have been “proven” in prior studies could equally apply to patients with an ASPECTS of 4 or 5 with small–moderate CTP core volumes and a large mismatch who are eligible for enrollment in studies that the commentary authors are involved with.
Inter-rater agreement for ASPECTS
As demonstrated recently by Van Horn et al from the TENSION trial investigators, even after ASPECTS training, one in three readings from study neuroradiologists resulted in misclassification on non-contrast CT based on TENSION eligibility criteria (0–2 vs 3–5 vs 6–8) in 20 illustrative cases.26 The potential consequences of inaccurate ASPECTs readings during the trial may threaten the validity and reproducibility of the study results.
We have accounted for the potential reliability concerns with ASPECTS in SELECT2 since the trial assesses large core on both CT and perfusion and evaluates the heterogeneity of thrombectomy effects in the different subgroups to allow a comprehensive assessment of the large core population.
Risk of early stopping for efficacy or futility
A concern raised was that SELECT2 might be stopped early because the patients with a large CTP core had a substantial benefit, while the large ASPECTS core patients may not show a statistical difference due to lack of power. This hypothetical concern is extremely unlikely to occur. The entire trial will be stopped early only if there is overwhelming efficacy in the entire population. A dominating effect in one subgroup is highly unlikely in SELECT2 given the substantial overlap between large CTP core and large ASPECTS core patients when both modalities are acquired.27 SELECT2 has a prespecified sensitivity analysis that assesses EVT efficacy and safety both with and without the large CTP core/ASPECTS 6–10 subgroup. Additionally, all patients’ data and subgroups of interest are reviewed regularly by our data and safety board (DSMB) of world-renowned experts in the field.
Similar issues of concern can be raised regarding studies that enroll patients entirely based on ASPECT scores. For example, if the ASPECTS-based studies are negative, we will not know if this is because the penumbral subgroup had benefit and the non-penumbral group did not, since there is no assessment of penumbra. If the studies are marginally positive, it is possible that they could reflect a substantial treatment effect in the penumbral patients and no treatment effect, or even some harm, in the non-penumbral patients. In addition, because inter-rater agreement on ASPECTS is only moderate, it is highly likely that some patients with site-read ASPECTS of <6 will be determined to have a higher ASPECTS on the core laboratory read by expert neuroradiologists.
Ultimately, the SELECT2 trial and the ASPECTS-based selection trials will all be needed to help evaluate the question of EVT in large core patients.
Conclusions
In conclusion, the editorialists, who are involved in complementary large core trials, assume they already know the answer as to whether EVT is beneficial in early window patients with a large CTP core and favorable ASPECTS, but they are relying on limited, low-quality evidence. Since ASPECTS is insensitive to irreversible ischemic changes in the early hours after symptom onset, some patients with very poor collaterals develop large regions of irreversible injury prior to the degree of injury being reflected in a low ASPECT score. As supported by the data presented above, these patients may or may not benefit from EVT and SELECT2 is the only study designed to clarify this issue.
The importance of the SELECT2 trial in addressing a critical area of therapeutic uncertainty has been supported by 30 institutional review boards, hundreds of investigators, and the United States Food and Drug Administration who have carefully considered the SELECT2 protocol and approved participation in the study. We look forward to the data from SELECT2 and other ongoing large core trials as we are confident that all of these trials will contribute to moving the field forward.
Data availability statement
Data are available upon reasonable request from the corresponding author.
References
Footnotes
Twitter @amrsarrajMD, @marcriboj, @dr_mchen, @VitorMendesPer1, @DrPatchiz, @PascalJabbourMD, @AdamArthurMD
Collaborators SELECT2 Investigators and SELECT2 Steering Committee.
Contributors AS designed and drafted the manuscript and provided administrative support. GWA designed and drafted the manuscript and provided critical revisions. BC, MR, MSH, MC, MGA, MGL, VMP, SB, CWS, RFB, NPO, JFA, TW, JB, MM, JS, JPT, NS, OK, DG, SW, DC, NWM, TJK, JMO, LE, GT, AA, PJ, BY, SEK, ASA, MP, JCG, and AEH provided critical revisions to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AS reports serving as the Principal Investigator (PI) for SELECT, SELECT2, a site PI for DEFUSE 3, and a speaker bureau and advisory board member in Stryker. MR reports serving as a site PI and steering committee member for SELECT2, and holds consulting agreement for Medtronic, Stryker, Cerenovus, Anaconda Biomed, Apta Targets, Sanofi, and reports serving as a speakers bureau member for: Philips, UCB Pharma, Ischemia View, and reports ownership in Anaconda Biomed, and Methinks. MSH reports receiving fees for consulting for Cerenovus, and reports serving as a member on DSMB for Rapid Medical, and DSMB for Cerenovus, and a steering committee member and a site PI for SELECT2. MGL reports serving as a steering committee member for SELECT2, and PI for DEFUSE 3. BY reports serving as a co-PI for SELECT2 and DIRECTS SAFE. JFA reports having received honoraria as speaker/consultant for the following companies: BI, Pfizer, Daiichi, Bayer, Amgen, and Medtronic; and reports serving as a site PI on SELECT2. The institutions where JFA works have received research funding from Spanish Ministry of Economy, European Comission, and Castilla y León Departments of Health and Education. JMO receives consulting fees from Aptoll, Abbvie, Medtronic, and reports receiving speaker fees from Pfizer, Bristol Myers Squibb. LE reports serving as a site PI on SELECT2 and a sonsultant for Cerenovus, Medtronic, VizAI, Microvention, and Scientia. AA reports serving as a speaker bureau member and consultant for NovaSignal, Longeviti, and Siemens. NW Manning reports serving as a site PI on SELECT2, and a consultant for Balt, Stryker, Microvention and Medtronic. CWS reports serving as an Imaging Core Lab member for SELECT and SELECT2. SEK reports serving as a site PI on SELECT2, and reports receiving consultant fees from Medtronic, receiving grants non-relevant to this work from WL Gore, Medtronic, Bristol-Myers Squibb, and other fees from Bristol-Myers Squibb (consultant), Abbvie (consultant), UpToDate (royalties), and Elsevier (royalties). ASA reports serving as a consultant for Balt, Johnson and Johnson, Medtronic, Microvention, Penumbra, Scientia, Siemens, Stryker, and reports receiving research support from Balt, Medtronic, Microvention, Penumbra, and Siemens, and is a shareholder at Azimuth, Bendit, Cerebrotech, Endostream, Magneto, Marblehead, Mentice, Neurogami, Serenity, Synchron, Triad Medical, and Truvic. MP reports research partnership with Siemens, Apollo Medical Imaging, and Canon; and reports serving as an advisory boards member for Medtronic, Boehringer Ingelheim. AEH reports serving as a consultant/speaker for Medtronic, Microvention, Stryker, Penumbra, Cerenovus, Genentech, GE Healthcare, Scientia, Balt; a site PI on SELECT2 and COMPLETE study – Penumbra, LVO SYNCHRONISE; steering committee/publication committee member for SELECT, DAWN, SELECT2, EXPEDITE II, EMBOLISE, CLEAR; a Proctor for Pipeline, FRED, Wingspan, and Onyx; and is supported by grants from GE Healthcare, Valley Baptist. GWA reports serving as a steering committee member for SELECT2, PI for DEFUSE 3, and reports receiving consulting fees for iSV and Genentech and has equity interest in iSV. BC, MGA, MC, SB, RFB, NPO, TW, JB, MM, JS, JPT, NS, OK, DG, SW, DC, and TJK report serving as site PIs for SELECT2. VMP, GT, PJ, and JCG report no relevant disclosures and no conflicts of interest to this work.
Provenance and peer review Not commissioned; internally peer reviewed.