Article Text

Statistics from Altmetric.com
We know without doubt that ‘time is brain’. How do we know this? It is a combination of data, logic, biological plausibility, and experience.
Now that endovascular treatment is the standard of care,1–5 we have an obligation to focus on process improvement to maximize patient benefit. As we go down the pathway of improving these processes, it is important to understand the idea of bottlenecks.
What are bottlenecks? In any complex process, not all parts of it are flow-limiting, especially when one considers parallel processing. For instance, imagine a situation where, in a particular hospital A, all endovascular stroke cases are done under general anesthesia (GA). Also imagine that, after working hours, anesthesia is usually available within 1 h of being called. The neurointerventionist is working hard with hospital administration to ensure that the nurse and technologist can be in the laboratory within 20 min instead of the current 30 min; even if successful, this would essentially be a waste of time as the bottleneck is anesthesia availability time. In the same scenario, now imagine that they took a decision to try to perform most cases without anesthesia; in this case, the availability of the team becomes the new bottleneck. This is what is meant by shifting bottlenecks.
Human behavior is such that, if one component of the overall workflow is extremely slow, there is a tendency to not worry about a few minutes here and there since the one particular bottleneck is overwhelming. As an example, in the days of intra-arterial tissue plasminogen activator (tPA), the endovascular procedure was so slow (often taking more than 1.5 h) that no one worried about speeding up the process of shifting the patient onto the angiography table.
The way in which bottlenecks in acute stroke workflow have shifted over a period of time is interesting. These changes have been a consequence of technology, data, competitive spirit, personal efforts, and endeavors of stroke teams in various hospitals. In the days of PROACT2,6 the technology available for opening the vessel was one of the biggest bottlenecks. Also, based on the teaching at that time (and the lack of widely available CT angiography (CTA)), many interventionists performed a complete angiogram before tackling the occluded vessel. The availability of the MERCI device resolved that bottleneck. The MERCI device had its limitations, however, as demonstrated in the SWIFT7 and TREVO28 studies. Ultimately, procedural bottlenecks are disappearing but other bottlenecks are beginning to stand out.
While all this progress was happening, the world of imaging was also undergoing major advancements. There were an ever-increasing number of proponents of MRI with the diffusion-perfusion mismatch paradigm. ‘Patient selection’ became the buzzword, and the impact of MRI on overall workflow was therefore not properly studied. Experts and centers created the so-called 6 min protocols9 (which would typically include diffusion, perfusion, MR angiography (MRA) and a blood detection sequence), but in reality would take much longer (finding out about MR compatibility, MR availability and access, managing intravenous lines and pumps, patient cooperation, kidney function, etc). This bottleneck was slowly overcome due to a combination of factors,10 including improvement in CT quality, increased use of CT perfusion, and dramatic improvement of and access to CTA (CTA currently far outperforms MRA in most situations, but more so in emergency situations). The number of centers across the world using MR-based decision-making is relatively few. It is possible that there may be further improvement in workflow with the advent of physiologic imaging in the angiography suite itself and/or with the implementation of hybrid CT–neuroangiography suites.11 ,12
Contemporaneously, the GA versus no-GA battle was being played out. Many centers traditionally did all acute stroke cases under GA. This was due to multiple factors. Many centers believed that the procedural complexity and length warranted GA and that, by minimizing movement during intracranial microcatheterization, GA was presumably safer. The shift away from GA happened due to a combination of factors, including several publications showing the lack of added benefits and potential for harm with GA,13 the development of newer devices that were quicker and better, and an overall shift in the field of neurointervention wherein there was a sudden growth in the number of centers and interventionists after a positive ISAT trial.
While all these changes were happening, other bottlenecks appeared and disappeared—for example, waiting for a response to tPA before deciding; creating order sets to expedite the process of door to imaging14; creating and implementing STAT stroke protocols. As workflow became faster, two new bottlenecks appeared: (1) CT perfusion: we found that collateral imaging was providing the same information for treatment decisions in most cases, despite taking less time,15 so we used collateral imaging within the ESCAPE trial3; and (2) the time to set up the angiography suite once the patient was ready: we found that this process was complex.3 ,16 The way that most catheterization laboratories are organized entails collecting many different packets from different parts of the laboratory and then opening all these packets prior to beginning the procedure. Also, we found that different items are required at different times; very often, a product that was not needed until later was presented first to the neurointerventionists—for example, the neurointerventionist is being handed the clot retrieval device while he/she is looking for a puncture needle. We successfully solved this problem by the creation of BRISK (Brisk Recanalization Ischemic Stroke Kit). For now this is a home grown solution allowing the catheterization laboratory to be constantly ready to receive a stroke patient by ensuring that a stroke table is always available where most of the needed products are laid out in a particular fashion to allow increased efficiency.
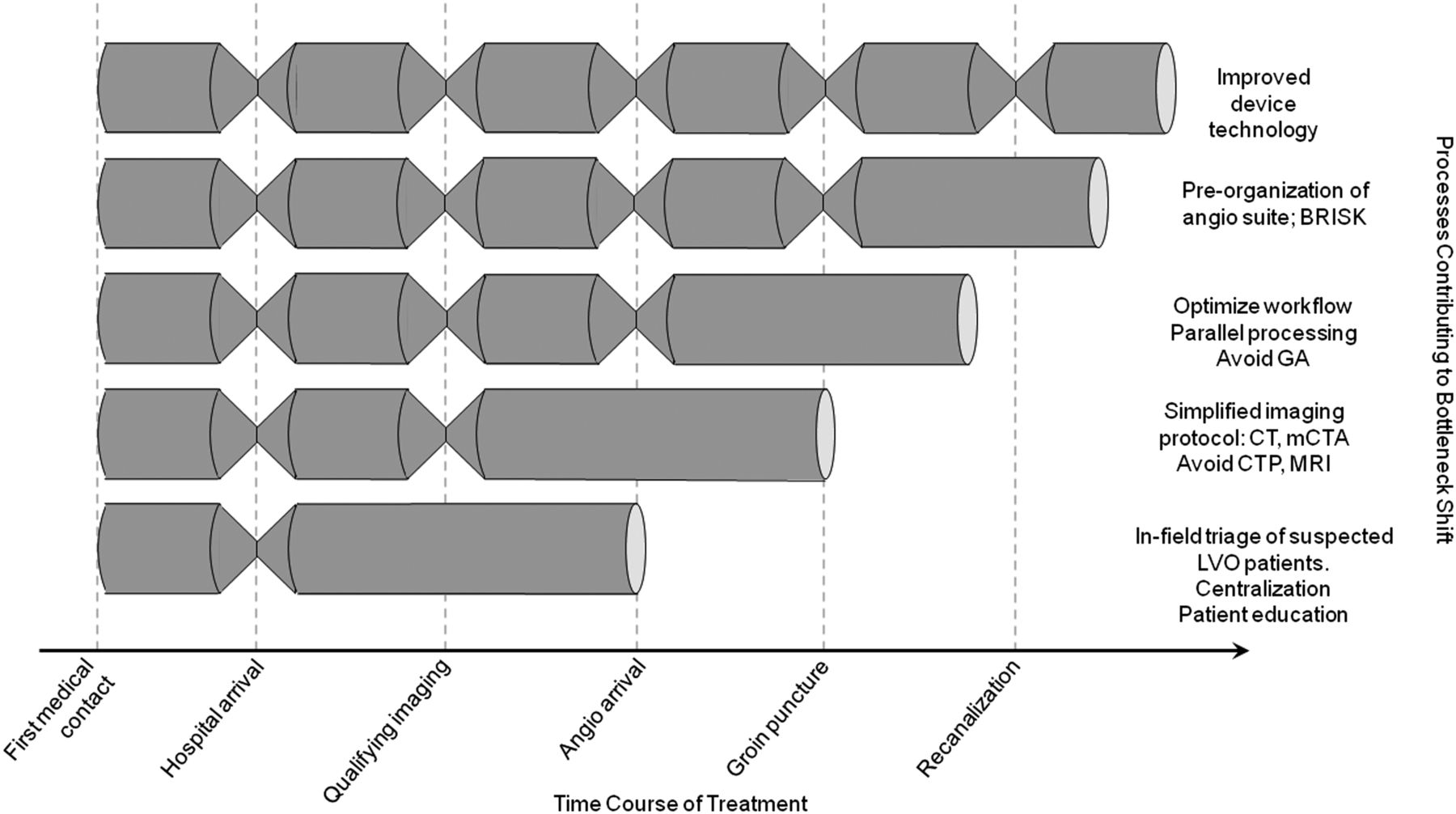
Over the last 10–15 years, using a combination of (1) better devices, (2) moving away from GA, (3) simple effective imaging (CT, multiphase CTA), (4) ever-ready catheterization laboratory, and (5) parallel processing and STAT stroke protocols, we have successfully overcome many of the shifting bottlenecks (figure 1).
{kind=link}
Shifting bottlenecks: the individual steps from first medical contact to final recanalization. Each pose potential rate-limiting steps in achieving fast reperfusion. Initial bottlenecks were faced in achieving fast recanalization and patient selection. With improvements at nearly every step, the remaining significant bottleneck is now in-field patient triage. BRISK, Brisk Recanalization Ischemic Stroke Kit; CTP, CT perfusion; GA, general anesthesia; LVO, large vessel occlusion.
So what is the biggest bottleneck now? It is getting the correct patient to the correct hospital quickly. We suspect that the solution to this lies as much in the realm of politics and economics as in the world of technology and teamwork. Irrespective of in which domain the solution lies, it is up to us as a collective to find the correct solutions to overcome the last of the bottlenecks.
References
Footnotes
Competing interests MG has received consulting fee from Medtronic for conduct and design of SWIFT PRIME trial. ESCAPE trial for partly funded by Medtronic through a grant to University of Calgary. MG has developed technologies related to improving systems of stroke diagnosis that has been subsequently licensed to GE Healthcare.
Provenance and peer review Not commissioned; internally peer reviewed.