Article Text

Abstract
Background Endovascular treatment of intracranial wide-necked and bifurcation aneurysms (WNBA) is technically challenging. The Nautilus Intrasaccular System is designed to provide a mechanical barrier at the aneurysm neck to support coil embolization. We report the results of a single-center series of patients treated for intracranial aneurysms with the Nautilus.
Methods Clinical and radiological data were retrospectively collected for all patients treated with the Nautilus for an unruptured or ruptured intracranial aneurysm at our center between March 2021 and March 2022. Clinical outcomes (modified Rankin Scale (mRS) scores), Raymond–Roy angiographic occlusion, recanalization, and complications were measured immediately post-procedure and at 3–6-month follow-up.
Results A total of 41 patients of mean age 56.7 years (range 37–83 years) were treated with the Nautilus, with 41 saccular aneurysms (18 (43.9%) unruptured and 23 (56.1%) ruptured). The majority of aneurysms (39/41 (95.1%)) were located in the anterior circulation. We experienced no technical complications. One patient had an asymptomatic post-procedural minor stroke related to the procedure. Immediate Class I occlusion was achieved in 30 (73.1%) patients. The rate of all-cause mortality was 7.3% (3/41). One patient was lost to follow-up. At follow-up, 94.5% (35/37) of patients achieved Class I occlusion and 94.5% (35/37) had an mRS score of 0. There were no procedural-related deaths or permanent morbidities at discharge or follow-up.
Conclusion This study demonstrates good safety and effectiveness using the Nautilus Intrasaccular System to treat both ruptured and unruptured intracranial aneurysms. Larger studies are needed to confirm these findings.
- Aneurysm
- Angiography
- Artery
- Brain
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Endovascular treatment of complex wide-neck and bifurcation aneurysms (WNBA) with flow diverter stents and intrasaccular implants is challenging. Advances in intrasaccular neck-bridging devices assist in coil embolization of WNBAs.
WHAT THIS STUDY ADDS
The Nautilus Intrasaccular System is a novel endovascular device designed for intrasaccular neck-bridging to assist in coil embolization of wide-neck aneurysms with good safety and effectiveness.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Most WNBAs are suitable for treatment with the Nautilus device with the benefit of avoiding antiplatelet therapy, reducing the risk of hemorrhagic complications related to periprocedural rupture of the aneurysm or vessel wall damage.
Introduction
Endovascular treatment of complex wide-neck and bifurcation aneurysms (WNBA) is challenging with the currently available techniques. Fluid dynamic disruption of the aneurysm via flow diverter stents and intrasaccular implants represents the state of the art in endovascular management of intracranial aneurysms.1 2 However, flow diverters have limitations related to the potential covering of bifurcation branches, the need for antiplatelet regimens, and compromised retreatment options,3 4 while some intrasaccular devices are limited by stiffness, shape, and available dimensions.2 5
Neck-bridging devices are designed to facilitate coil stability and reduce the risk of coil protrusion/herniation by providing a mechanical barrier that holds the coil mass in place.6–8 The Nautilus Intrasaccular System (EndoStream Medical, Israel) is a novel CE-marked endovascular device designed for intrasaccular neck-bridging to assist in coil embolization of wide-neck aneurysms. The Nautilus is a nitinol-based detachable implant consisting of flexible layers. Successful clinical use of the Nautilus has recently shown good technical results in aneurysms in various locations.9–11
We report the results of a single-center series of intracranial aneurysms treated with the Nautilus, with clinical and angiographic follow-up results at 3–6 months.
Methods
Patient selection
This was a single-center series of patients with intracranial aneurysms treated with the Nautilus. Multidisciplinary teams decided on the optimal treatment approach before each intervention. Factors included the clinical condition of the patient, morphological characteristics of the target aneurysm, regional vascular anatomy, width of the neck, and condition of the procedure (ie, in the setting of acute subarachnoid hemorrhage or elective treatment). The criterion for a wide-necked aneurysm was a neck diameter ≥4 mm with a cut-off dome-to-neck ratio of <2. Further complexity was added if the target aneurysm was present at the level of an arterial bifurcation or with radiological evidence of vessel incorporation at the neck. Assuming that Nautilus-assisted coil embolization was considered feasible, the proposed technique and procedural details were discussed with the patient and family. Alternative approaches included balloon remodeling, stent-assisted coiling, and flow diversion.
Device description
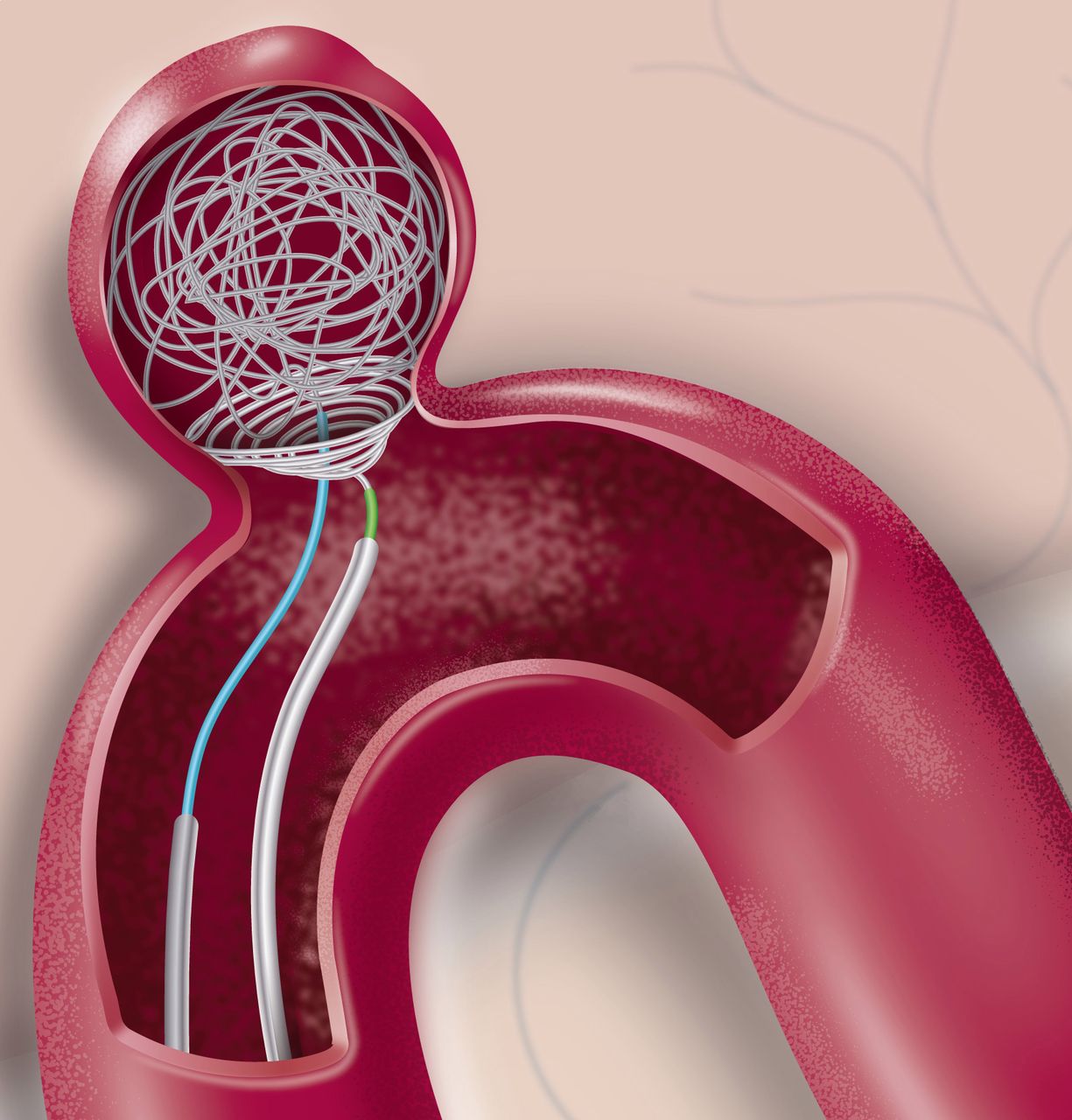
The Nautilus Intrasaccular System is an endovascular device containing a self-expanding metallic structure consisting of a spiral element and a distal ring made from a radio-opaque single nitinol wire covered with a platinum alloy coil. The nitinol component allows the Nautilus to undergo a unique and reversible phase transformation between a soft embolization coil to a firm discus-like shape. The device is available in sizes ranging from 4 to 7 mm in diameter. Volumetric measurements and three-dimensional considerations of aneurysm geometry are unnecessary because the Nautilus is a mechanical barrier that aims to reconstruct the neck from within the aneurysm. Therefore, aneurysm necks wider than 6.5 mm in diameter may constrain the successfully implanted Nautilus. The implant is fully compatible with currently available 0.0165 inch microcatheter technology. During insertion into the aneurysm, the Nautilus is flexible and easily bendable. Its structure changes into a dense discus shape after being fully deployed at body temperature. The device is fully retrievable and may be repositioned by retraction into the microcatheter during or after deployment. It provides a solid supporting framework that enables coil embolization. When fully deployed, the Nautilus features a 1 mm central hole that allows navigation of a dedicated microcatheter meant for coil insertion. The Nautilus is wire-mounted and can be mechanically detached from the delivery wire at any point (see figure 1 and online supplemental figure 1).
Supplemental material

{kind=link}
Artist’s impression of Nautilus-assisted coil embolization of a cerebral saccular aneurysm. The device creates a solid and compliant mechanical barrier that facilitates the complete embolization of the target aneurysm. ©Anton Robov, used with permission, all rights reserved.
Endovascular procedure
Two operators used the device in this series, none of whom had previously used the Nautilus in a patient. The use of Nautilus was based on the treating physician’s discretion. All procedures were performed using a 6 F femoral approach under general anesthesia. Three-dimensional rotational angiography provided information on aneurysm anatomy, including the relationship between the parent artery and adjacent proximal vessels. The Nautilus size chosen for each case was based only on the neck diameter of the aneurysm. The selected device was oversized by at least 0.5 mm to increase compliance across the neck and fully reconstruct the latter. Under roadmap guidance, the aneurysmal sac was carefully catheterized via the 0.017 microcatheter. The tip of the microcatheter was intentionally positioned at the level of the equatorial plane of the aneurysm. The Nautilus was carefully inserted into the delivery microcatheter and attached to a flushing saline bag via a Y-connector fixed at its proximal end. The device was then successfully deployed at the midline of the aneurysm, carefully retracted, and adjusted to the neck. If an imprecise position of the device was observed, the implant was resheathed and redeployed in the desired position. Once the optimal implantation of the device was obtained, we proceeded with the navigation of a second microcatheter for coil delivery. Catheterization of the aneurysm sac was obtained through the central hole of the Nautilus. The radio-opacity of the device and its opening were easily distinguished. The tip of the coiling microcatheter was navigated and positioned near the bottom of the sac. Both standard framing and soft embolization coils could be used as the first coils inserted inside the aneurysm sac. Separation of the Nautilus device from the delivery wire can be achieved either after the first coil is inserted and a solid embolization structure has been obtained or on completion of the coiling process. Once the desired obliteration level was confirmed, the coiling microcatheter was slowly retracted out of the aneurysm past the opening of the neck-bridging implant. Separation of the Nautilus from the delivery wire was achieved via the detachment handle attached to the proximal end of the device. This technique was successfully carried out in all patients (figure 1).
Data management and analysis
We recorded patient demographics and aneurysm characteristics (localization, size, morphology, and ruptured or unruptured status). Baseline modified Rankin Scale (mRS) score, Glasgow Coma Scale score, and Fisher scale and Hunt and Hess scale scores for ruptured aneurysms were also recorded. Procedural data included the date, catheters used, Nautilus size selection, number of deployments and secondary navigation attempts, number of used coils, perioperative medications, and the incidence of technical and procedure-related complications.
Antiplatelet and anticoagulation regimen
Intraprocedural anticoagulation (heparin, 50 IU/kg) was initiated on insertion of the femoral sheath. No dual antiplatelet therapy was assigned to any of the reported patients including those who presented with acutely ruptured aneurysms. The primary rationale behind the absence of an antiplatelet prophylaxis regimen is that the Nautilus device operates within the aneurysm and does not harbor any intravascular components. In accordance with our local institutional protocol, we do not administer antiplatelet prophylaxis if there is no need. The flushing bags for all microcatheters contained 5000 IU/L of heparin.
Clinical evaluation
mRS scores were assessed at 24 hours, at discharge, and 3–6 months post-procedure. A good outcome was defined as mRS 0–2 and a poor outcome as mRS 3–6. The Raymond–Roy (RR) aneurysm occlusion scale was used to evaluate the aneurysm status at final angiography during embolization and the available radiological follow-up examination.12 Aneurysm recanalization was defined as the deterioration of RR classes I to II or III or an RR class II to III. Device- and procedure-related adverse events were radiologically assessed by the physician at the end of each intervention.
Statistical analysis
Continuous parameters were summarized by a number of evaluable observations, mean, ranges, median, minimum, and maximum. Categorical data were described by frequency counts and percentages with 95% exact binomial confidence intervals added where applicable.
Results
Patient and aneurysm characteristics
A total of 41 patients were treated with the Nautilus between March 2021 and March 2022. Patient baseline and aneurysm characteristics are presented in table 1. The mean age was 56.7 years (range 37–83) and 53.6% (22/41) were female. The majority of aneurysms were small (65.9% (27/41)), 29.3% (12/41) were large, and 4.9% (2/41) were giant. Twenty-three patients (56.1%) presented with a radiologically confirmed de novo ruptured intracranial aneurysm. All elective patients were neurologically intact and had a pretreatment mRS score of 0. The majority of aneurysms (95.1%, n=39) were located in the anterior circulation, including the internal carotid artery (ICA) (9.75%, n=4), posterior communicating artery/ICA bifurcation (21.8%, n=9), anterior communicating artery (26.8%, n=11), and middle cerebral artery (MCA) (36.6%, n=15). Two aneurysms (4.9%) were located in the posterior circulation in the basilar artery. The mean aneurysm diameter was 8.3 mm (range 2.76–21 mm) with a mean neck diameter of 5.2 mm (range 3.6–8.1 mm).
Baseline patient and aneurysm characteristics
Technical and procedural results
A total of 41 devices were successfully implanted in 41 aneurysms (table 2 and online supplemental figure 2). A pre-shaped 90° tip microcatheter for device delivery was used in 24.3% (10/41) of cases. Nautilus delivery inside the aneurysmal sac was performed using the Headway 17 Advanced (MicroVention) microcatheter in 90.3% (37/41) of cases, and the Excelsior SL 10 (Stryker Neurovascular) in the remaining 9.75% (4/41). Complete implant deployment across the aneurysm neck was observed in all cases. Thirty-four devices (82.9%) were deployed at the first attempt, while seven (17.1%) devices were ultimately recaptured and redeployed. In 7.3% (3/41) of cases we observed insufficient and uncompliant neck reconstruction/coverage at the time of initial deployment. In these cases, the lack of neck-bridging was due to under-sizing of the implant caused by measurement errors and the learning curve. The devices were replaced with those of adequate size, at least 1 mm larger than the previously selected devices.
Procedural data and technical results
Navigation of the second microcatheter intended for coil delivery was successfully performed in all cases. The intended central point of the Nautilus was easily catheterized in 92.6% (38/41) of aneurysms. In the remaining three cases, we navigated the second microcatheter through the struts of the already deployed neck-bridging device. To facilitate navigation through the central opening of the neck-bridging implant, we straightened the previous microwire curve. Uneventful withdrawal of the coiling microcatheters was observed in all cases. There were no adverse interactions between the coiling catheters and the implanted Nautilus. Visualization of the neck-bridging device was achieved in all instances, further facilitating the procedure. We documented no migrations, movements, or protrusions of the Nautilus during the coiling process. The tornado-like shape of the Nautilus and the nitinol composition further allowed conformity and support at the aneurysm/neck interface during coiling. Mechanical detachment of all 41 deployed devices was successfully conducted. Complete separation of the device from the wire via the detachment handle was achieved in 38/41 cases (92.6%). Detachment by manual retraction of the mounting wire from the hypotube of the device was used in 7.3% (3/41) of cases. In 80.4% (33/41) of cases the implant was mechanically detached from the mounted wire once the first framing coil was successfully delivered. The total number of inserted coils was 260, with an average of 6.3 coils per case.
Complications
One patient experienced a minor asymptomatic post-procedural stroke. This patient had an unruptured MCA bifurcation aneurysm embolized using the Nautilus. No technical difficulties were experienced during the embolization. Final angiography documented no thromboembolic complications in the MCA territory. Twenty-four hours after the treatment, routine post-procedural brain imaging confirmed the presence of two 3 mm hypodense lesions parallel to the lateral ventricles in the centrum semiovale. The neurological status of the patient remained unchanged from baseline. Considering the deep border zone infarct seen on the post-procedural CT scan, we believe the event was related to a secondary microembolism caused by either blood flow disturbances of the two microcatheters or distal embolism during navigation of the guiding catheter. We observed no device-related vasospasm, iatrogenic aneurysms, or parent artery injuries. There were no device interactions, migrations, or prolapses. During embolization there was no angiographic evidence of blood flow disturbances at the aneurysm neck or the parent artery.
There were no other ischemic or hemorrhagic events in the survivor group after treatment within the first 30 days. The all-cause mortality rate was 7.3% (3/41), none of which were device- or procedure-related. Systemic inflammation and secondary organ dysfunction were the principal non-neurologic causes of death in this series. Clinical 3–6-month follow-up data were available for 97.3% (37/38) of survivors; at this time 94.5% (35/37) of patients had an mRS score of 0.
Device effectiveness
Complete aneurysm occlusion on post-embolization angiography was recorded in 73.1% (30/41) of patients. Final post-embolization DSA confirmed a neck remnant in 21.9% (9/41) of patients and aneurysmal remnants in 4.8% (2/41). Radiological follow-up at 3–6 months was available for 90.2% (37/41) of patients. Follow-up fluoroscopic analyses via DSA were performed in 28 patients, while MRI was available for nine patients. Complete occlusion was confirmed in 94.5% (35/37) of aneurysms, neck remnant in 0% (0/37), and residual aneurysm in 5.4% (2/37). Progressive obliteration of the aneurysm in terms of improved RR occlusion class was confirmed for 13.5% (5/37) of aneurysms (online supplemental figure 3). No aneurysms bled during the follow-up period. All implanted Nautilus devices remained in position. We found no device migrations or small-scale changes to the previously inserted embolization masses and coil baskets. Treatment-related and follow-up aneurysm occlusion rates are shown in table 3.
Treatment-related and follow-up angiographic outcomes and results
Discussion
This retrospective series summarizes an initial single-center experience of 41 patients with ruptured and unruptured intracranial aneurysms treated with the Nautilus. We achieved good occlusion rates at 3–6-month follow-up and experienced no technical complications with detachment or delivery of the device, with only one asymptomatic post-procedural complication. Our findings suggest good safety and effectiveness results with the Nautilus in both ruptured and unruptured WNBAs. These results compare favorably with previous reports on WNBAs with different techniques and approaches.13–16
Intrasaccular flow disruption is an offspring technique derived from the concept of endoluminal flow modulation, and has been applied specifically to WNBAs located at arterial bifurcations. Despite growing enthusiasm, few dedicated devices have been introduced into neurointerventional practice: WEB, LUNA/AED, and (more recently) the Contour device.17–19 The implants share common designs that aim to limit the inflow into the aneurysm sac once fully deployed, and promote neoendothelium growth at the aneurysm neck. The primary advantage of the Nautilus is that it is independent of dual antiplatelet therapy, which is often helpful, particularly in ruptured aneurysms.1 Although conceptually similar, the devices have unique features and properties and may overlap in terms of being suitable for treating complex WNBAs.20 Although the spherically-shaped WEB and LUNA devices are designed to fill the aneurysm volumetrically, the Contour has no volume but adapts to the neck plane in a conical or U-shaped fashion.21 Limitations with these approaches include the steep learning curve regarding control and precision of device placement, case selection, and implant sizing.22 Notwithstanding the growing popularity of this technique, the relevant published data should be interpreted with caution as they may not be generalizable to general practice.23
The WEB device has been studied in several larger prospective and small retrospective case series. A recently published systematic review of 15 articles on the use of the WEB in 963 aneurysms (mostly WNBAs) suggested promising results.24 The overall occlusion rate was 83.3% at final follow-up, with non-negligible complication and retreatment rates. Limited data are available for LUNA and Contour. The CERUS study reported adequate occlusion rates up to 84% at the final available follow-up.25 Recently, Biondi et al confirmed that the Contour device yields up to 89.3% adequate occlusion (defined as complete occlusion or presence of a neck remnant).26
Advances in neck-bridging devices have improved safety and effectiveness since the advent of the first neck-bridging device, the TriSpan.27 The Nautilus has similar results to currently available neck-bridging devices such as the PulseRider, pCONUS2, and pCANVAS. The ANSWER trial assessed 34 patients with a WNBA treated with PulseRider, demonstrating RR I or II occlusion in 87.9% of patients at 6 months, with mRS 0–2 in 94% of patients.28 A 2022 multicenter study29 that used the pCONUS2 device in 55 patients with mostly bifurcation aneurysms found a technical success rate of 98.2%, a complication rate of 8.9%, a permanent morbidity rate of 1.8%, mortality rate of 0%, and occlusion rate of 83.4%. A 2019 study30 using the pCANVAS device in 17 patients with unruptured aneurysms observed an RR class 3 in 68.8% of patients (11/16) and RR class 1 in 31.2% of patients (5/16) at follow-up. The results from the present study with the Nautilus device showed comparable rates of complications, occlusion, morbidity, and mortality to other available neck-bridging devices.
The Nautilus device and its design should not be directly compared with existing neck-bridging devices as it is entirely intrasaccular. Unlike the PulseRider, pCONUS 2, and the pCANVAS devices, the Nautilus does not have any intraluminal parts.
Regarding design similarities, the NEQSTENT (Cerus Endovascular) is a dedicated intrasaccular device that can be used as a coiling assisting device.31 32 This implant has 48 wires and is braided more compactly than its counterpart, the Contour. This design porosity mainly allows access through the mesh or between the implant and the aneurysmal wall by a coiling microcatheter. Although the published literature describing use of the NEQSTENT is limited to two retrospective studies, the technical aspects of the NEQSTENT likely mirror Nautilus-assisted coil embolization. In both techniques the devices are selected based primarily on the dimensional characteristics of the aneurysmal neck. Also, the inserted coil mass in both methods increases device compliance with the aneurysm/neck interface. Anchored across the aneurysmal orifice, both devices likely have higher occlusion rates than conventional techniques. However, the lower profile 0.017 inch delivery system is a significant advantage favoring the Nautilus embolization system over the 0.021 inch NEQSTENT.
We believe that the progressive occlusion of the aneurysms observed during follow-up is related to the ability of flexible layers of drawn-filled tubing of nitinol to hemodynamically seal the aneurysm neck. We hypothesize that the mechanical scaffold of the implant encourages aneurysm healing via endothelial cell migration and overgrowth. Additionally, the implant is compatible with the available 0.0165 inch microcatheter technology. The device is available in sizes ranging from 4 to 7 mm in diameter; therefore, most WNBAs are suitable for treatment with the device. We advocate slight oversizing of the implant by at least 0.5–1.5 mm over the aneurysm neck diameter, so the recommended upper limit of neck width is 5.5–6.5 mm. Volumetric measurements and three-dimensional considerations of aneurysm geometry are unnecessary because the Nautilus device is a mechanical barrier that aims to reconstruct the neck from within the aneurysm. However, based on our experience, selecting aneurysms with larger heights and widths only promoted the successful technical execution of Nautilus delivery and deployment across the neck. Having more room for manipulation with the device inside the aneurysm was favorable, especially during the initial experience with the implant. Finally, and contrary to the other series of endosaccular flow modulators, we did not use antiplatelet therapy. Theoretically, avoiding antiplatelet therapy may reduce the risk of hemorrhagic complications related to periprocedural rupture of the aneurysm or vessel wall damage.
Limitations
Our study has a few limitations, most notably that it is a single-center series with a retrospective analysis, with physician adjudication and without a comparator group. Technical and procedural results were limited by the level of expertise of the senior and junior authors. We may have underestimated the long-term durability of the technique because of the short follow-up period. Despite these limitations, we have described the results of a new technique that we are optimistic is a valuable addition to the arsenal of endovascular and embolization techniques.
Conclusion
This study demonstrated good safety and effectiveness using the Nautilus Intrasaccular System to treat ruptured and unruptured WNBAs. The low-profile compatibility of this approach and the fact that it can be safely applied without dual antiplatelet therapy further reduce the complexity of the technique.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
All procedures performed in the study involved human participants and were carried out in accordance with the ethical standards of the institutional and national research committees. Informed consent was obtained from all individual participants included in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AlexanderSirak1
Contributors All authors contributed to the design of the work and the acquisition, analysis, or interpretation of data, drafted the manuscript or made critical revisions, approved of the final version to be published, and agree to be accountable for all aspects of the work. Guarantor: SS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.