Article Text

Abstract
Introduction Retrospective analysis of patients suffering iatrogenic dissection during neurointervention is reported. The circumstances surrounding the occurrence, early detection, clinical course and management options are discussed.
Methods and results 18 iatrogenic dissections over 11 years were retrospectively analyzed. Data were gathered from patient records, run sheets, morbidity records and imaging studies. All procedures were done by operators trained to operate according to institution standards. Total cases were 6981, with 3925 angiograms and 3056 interventions. Incidence was 0.26%, with 0.25% during diagnostic and 0.26% during intervention. 1031 pediatric cases had no dissections. Beyond 35 years, dissection rate increased to 0.35%. There was no difference between men and women. Carotid dissection was more common than vertebral. Most were minimal intimal tear (67%) and others flow limiting (33%). All cases were managed with heparin in the acute stage and later with aspirin and Plavix or Coumadin, except in two cases. Cases having >70% luminal narrowing with poor intracranial cross circulation were stented. None presented with neurologic deficits acutely or on follow-up. 94% of patients were followed for a variable period, with variable imaging modalities, being a retrospective study. Angiogram, MRI brain with MR angiography (MRA), Doppler ultrasonogram and CT angiograms were used for follow-up. There was good outcome in 94% of the followed-up cases.
Conclusion Iatrogenic dissection is a random event with a benign clinical course. Early detection and aggressive management result in excellent outcome. Angiography is the best modality to follow-up. Non-invasive imaging like MRI with MRA and duplex ultrasonography are good tools to follow dissections.
Statistics from Altmetric.com
Neurointerventional procedures are invasive, involving placement of guidewires and catheters into the blood vessels of the head, neck and brain, with an inherent risk of arterial dissection. Dissection of the cranial vessels poses a risk of ischemic injury to the brain. Arterial dissections can cause ischemic symptoms by limiting flow secondary to severe stenosis, occlusion or by acting as a source of thromboembolism. We report a retrospective analysis and review of patients suffering iatrogenic arterial dissections during cerebral angiography and cerebrovascular interventions. We evaluated the specific circumstances surrounding the occurrence of dissection, early detection, subsequent clinical course, follow-up and management options.
Methods
Cases were retrospectively collected from a high volume tertiary care center over a period of 11 years from January 2000 to December 2010. The cases were identified through a computerized review of the angiography records, using the search term ‘dissection’, and through a search of the morbidity and mortality conference records, which record all complications. We excluded all traumatic and spontaneous dissections. We collected data from the patient records, procedure run sheets, morbidity meeting records, follow-up records and imaging studies.
Patient demographics were recorded. The run sheets during the angiographic procedure during which the dissection occurred were reviewed, the size and type of catheter and the guidewire used during the event, the number of runs done before the procedure, the rate and volume of material injected prior to the dissection and if three-dimensional imaging was done before the dissection.
Angiograms of the patients were reviewed, with particular attention given to the artery dissected, the length of the dissected segment and the degree of stenosis (per cent diameter) or occlusion caused by the dissection, and the follow-up angiogram results were analyzed.
The clinical condition of the patient following the events was obtained from the follow-up records.
In all cases the procedures were done according to institution standards by the operator trained in or training in the institution. The angiographic catheterizations were performed using a standard ‘over the wire’ catheter technique, and contrast material was then test injected before the run. In all cases power injector was used for injection. The power injection rates used were 6 ml/s for the internal carotid artery, 8 ml/s for the common carotid artery and 3–6 ml/s for three-dimensional imaging over 7 s. Most patients had follow-up clinically, angiographically, by cross sectional imaging with CT angiography or MR imaging of the brain and by Doppler ultrasonography. Because this was a retrospective study, the clinical and imaging follow-up periods were variable, ranging from 1 day to 5 years.
Results
In total we had 6981 cases, of which 3925 were angiograms and 3056 were interventional cases. The overall incidence of arterial dissection was 18 (0.26%). The incidence during diagnostic procedures was 10 (0.25%) and during intervention was eight (0.26%). At our center, pediatric interventions are more common. We have not had any dissections among 1031 angiograms and intervention procedures in pediatric cases (less than 18 years of age). The incidence from 35 years of age was much higher at 0.35% and stayed at this rate for the rest of life (figure 1). Most dissections occurred between 35 and 70 years of age and this is the age group during which most interventions were done. The incidence between men and women were the same as overall incidence, without any significant difference between the two groups. In most cases, 5 Fr catheters were used, and we did not find any one type of catheter or guidewire causing more damage than others. Most cases had more than one run into the artery that was dissected. The number of runs varied from 1 to 6. Four of the cases had three-dimensional runs before the dissection. In our series, we had 10 carotid artery dissections compared with eight vertebral artery dissections. The dissection in most cases was minimal intimal tear (67%). In only 33% of cases it was flow limiting. We stented cases with more than 70% luminal narrowing and poor intracranial cross circulation. All cases were managed with heparin in the acute stage and later with aspirin and Plavix, with the exception of two cases that had acute intracranial bleeding prior to the procedure. There were two cases that had vessel occlusion of more than 70% with good intracranial cross circulation and did not receive stenting. One of the cases had a good outcome with vessel recanalization without flow restriction at 3 months. None of the cases presented with any neurologic symptoms acutely or on follow-up.

Age distribution of dissection.
The follow-up period ranged from 1 day to 5 years and the imaging modalities were variable, as this was a retrospective study. We used angiogram, MRI brain with MR angiography, Doppler ultrasonography and CT angiograms for follow-up imaging. We followed all but one patient (94%). We had excellent outcome in terms of caliber of the vessel and absence of neurologic deficit in 94% of all followed-up patients (table 1).
Summary of iatrogenic dissection cases, their management, follow-up and outcome
Discussion
Little has been reported in the literature regarding iatrogenic dissection complicating the neurointervention procedures. Most publications were in the early phase of development when the technique, protocol and hardware were improving. Now with the procedures being done more frequently than ever, with standard protocols and improved hardware, we analyzed whether or not we are any better in preventing the occurrence of iatrogenic arterial dissection and also the management of this condition.
Patterns of dissection and presentation vary. Dissection can be a minimal intimal tear, most commonly a non-flow limiting condition; separation of the intimal flap to variable length either longitudinally or circumferentially, forming a false lumen that may or may not communicate with the parent lumen distally and commonly causes flow limitation to a variable extent. Pseudoaneurysms are formed if the dissection is between the media and adventitia. It has no flow limitation but acts as a source of emboli. Rarely, slow arterial filling and distal emboli can be the presenting appearances of arterial dissection.1
On reviewing the literature of dissection as a complication of interventional procedures, we had valid information to compare. Olivecrona2 reported a 0.1% incidence and Huckman and colleagues3 reported 0.6%. Neither of these reports provided details regarding the outcome of these vascular injuries. Vitek4 reported seven cases of injury to the internal carotid artery that were caused by subintimal injection of contrast material among 2000 angiograms (0.35%). Harry and colleagues5 reported an incidence of 0.4%. None of these studies reported separately for diagnostic and interventional procedures. The overall incidence in our series is 0.25%. With diagnostic procedures the incidence was 0.25% and during intervention it was 0.26% (table 2). In our series, most cases had a diagnostic angiogram before the intervention. During the diagnostic procedure there is higher manipulation moving back and forth to image various vessels. During the interventional procedures, although we stick to one vessel, there are more manipulations during the procedure.
Percentage incidence of dissection was constant in various groups and was comparable with overall incidence
The overall incidence and natural history of spontaneous and traumatic dissections are difficult to detect. As only patients with obvious symptoms present clinically, it is difficult to compare the incidence of iatrogenic dissections with spontaneous and traumatic dissections. The natural history of the iatrogenic dissection is benign with appropriate management. None of our patients developed focal neurologic deficits. Neurologic deficits following dissection most commonly occur within the first few days but can occur in rare situations up to 1 month after the onset of the event.6 In our series, although we had more women than men, the incidence in men (0.24%) and women (0.27%) was similar and comparable with the overall incidence (0.24%) (table 2).
Iatrogenic dissection in children is extremely rare. We did not have a single case of dissection in patients <18 years of age and we could not find any reports in the literature of iatrogenic dissection in pediatric patients. We feel this could be due to the non-tortuous course of the vessels in pediatric patients requiring less manipulation, and all manipulations were always done by the most senior person in our team. The incidence increased significantly beyond 35 years of age to 0.35% and remained at this rate for the rest of life. As most interventions are done between 35 and 70 years of age, most patients have a risk of 0.35% for dissection of vessels (figure 1).
Our analysis of predisposing causes yielded valid results. The guidewire used during the procedure was relatively constant and we have used only a few types of improvised catheters. We had dissections with all catheter types. We did not find any particular catheter to be more traumatic than another. Most cases had multiple runs into the dissected vessels before arterial dissection was identified. The number of runs ranged from 1 to 6. Four cases had three-dimensional imaging runs before the procedure. All injections before dissections were done using power injector. We do not know if injection with the power injector caused or perpetuated the event. One of the vessels had fibromuscular dysplasia changes; another had associated multiple mycotic aneurysms in the brain. Others were related to catheter exchange, balloon test occlusion, balloon angioplasty, more tortuous course of the vessel and guidewire manipulation to gain access to the target vessel. Of the seven dissections associated with intervention, four cases had catheter exchange prior to dissection. The most common correlate was manipulation inside the vessel. Although the causes were varied, pre-existing diseased vessel, more difficult course and higher manipulation resulted in dissections.
We found more carotid dissections than vertebral dissections. Other series have reported more vertebral dissections. Harry and colleagues5 reported a higher incidence in vertebral dissection and claimed this is possible due to the following factors that make the vertebral artery more prone to injury: (1) it is usually smaller than the internal carotid artery, such that the guidewire and catheter are more constrained and generate relatively more tension against the arterial wall; (2) it is constrained in a canal made up of the transverse foramina of the vertebral bodies, which limits its ability to conform to the shape of the catheter and the guidewire; and (3) it often has a tortuous origin, especially in elderly patients. We attribute lower dissection rates in vertebral arteries in our study to our strategy of doing a road map of the subclavian artery, and not manipulating in the vertebral artery if it had a narrowing at the origin. We do either vertebral injection with the catheter closer to the origin or a subclavian injection. Even on gaining entry into the vertebral artery, our strategy is not to go too high to the region of the vertebral canal where the artery is relatively immobile and there is a greater chance of trauma.
Interventionalist should have a high index of suspicion of finding out dissections during the procedure, especially those with minimal intimal tear for effective management and prevention of neurologic complications. Atherosclerotic disease and fibromuscular dysplasia can mimic a dissection during angiography. In such a situation, comparison with previous runs of the angiogram or previous angiogram and follow-up angiogram weeks later can help in the differentiation.7 In spite of test injections, in all cases the dissection was detected after the run had been completed. The following factors could initiate the initmal tear during catheter advancement: (1) the forward jump of the catheter as pressure is built up on the catheter; (2) intimal scratch of the catheter tip with cardiac pulsation; (3) jet of injecting contrast; and (4) guidewire traumatizing the intima. In spite of checking the flow, during the test phase injection the tear is usually not very obvious. The partial tear is converted to a complete tear with contrast injection.
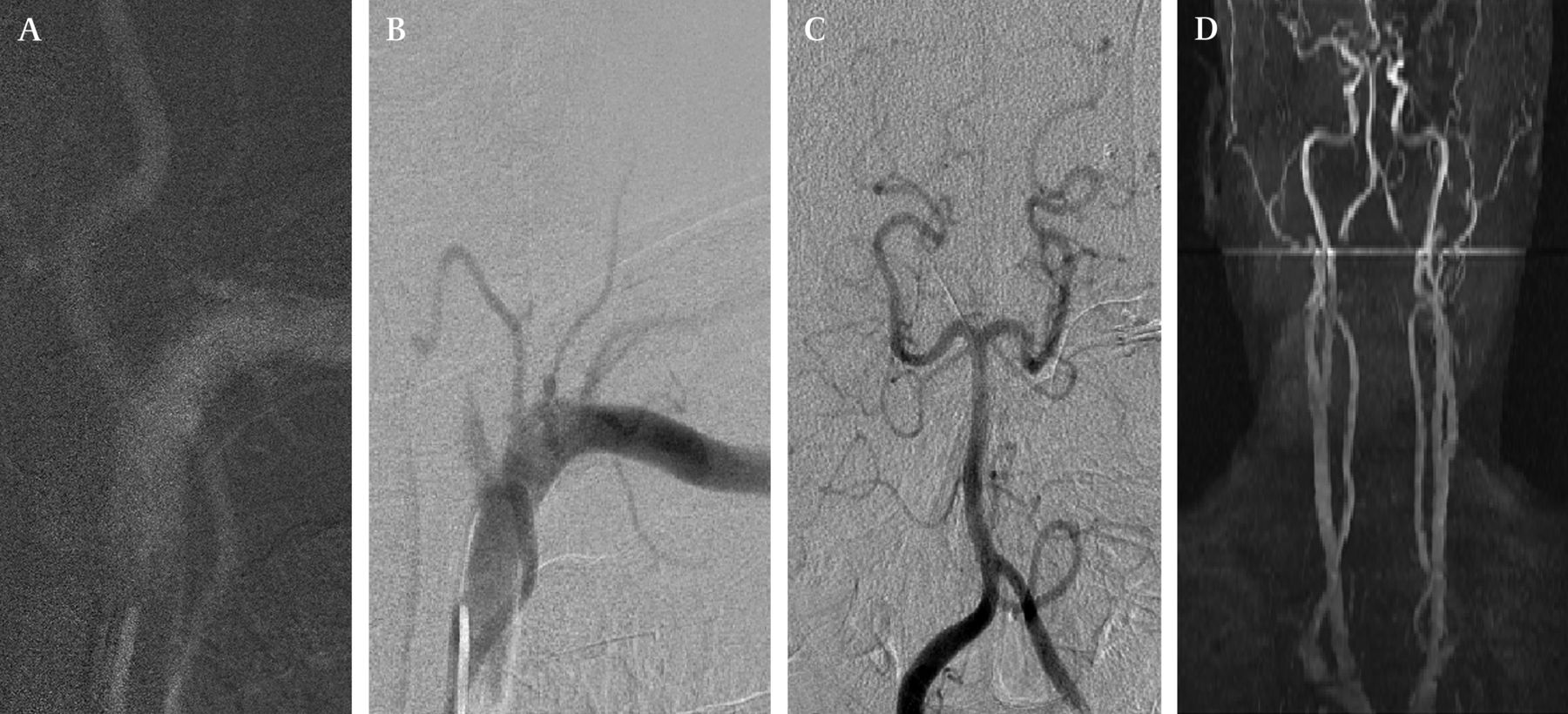
The dissection can be minimal intimal tear that does not limit flow but has a higher chance of throwing emboli. It can be a large tear extending to a variable length and producing flow limitation. In all flow limiting cases, we checked the cross circulation in the brain. If in doubt we aggressively stented. Out of the 18 cases we stented three cases. We stented cases with more than 70% luminal narrowing and poor intracranial cross circulation. Two cases with more than 90% stenosis due to vertebral artery dissection were not stented as they had good flow through the other vertebral artery (figure 2). One of the stented cases had significant narrowing with good intracranial cross circulation, with an arteriovenous malformation in the same territory. We stented that case in order to preserve the vessel for future intervention (figure 3). All but two cases in our series had heparin infusion immediately and were followed by aspirin and Plavix or Coumadin for a minimum of 3 months. Of the two cases not treated medically, one had acute subarachnoid hemorrhage and other had intracerebral hemorrhage. We are of the opinion that most dissections are minimal intimal tear that can be safely and effectively treated medically. If it is flow limiting with poor intracranial cross circulation, stenting should be considered. We used heparin in the acute stage followed by antiplatelets for a period of 3–6 months.
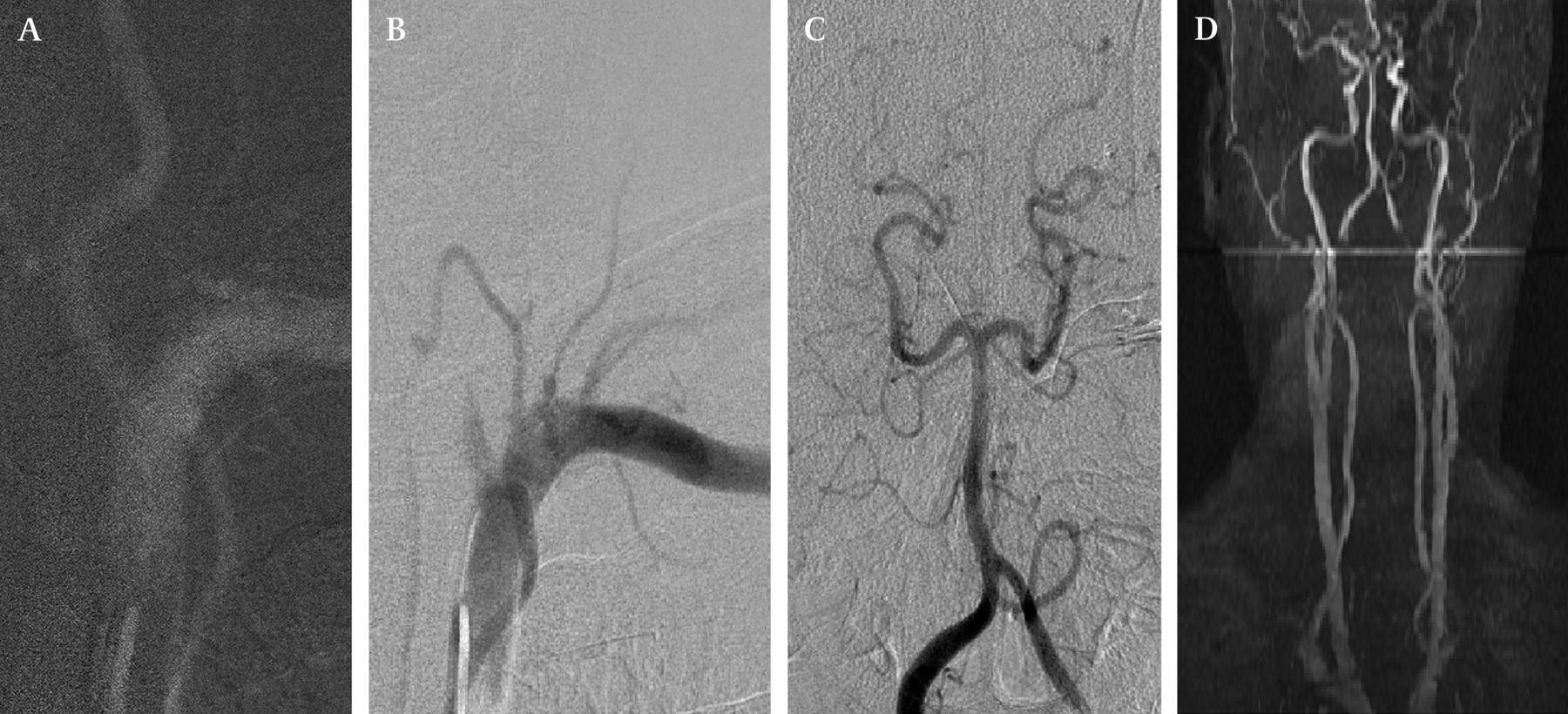
(A) Left vertebral artery was patent during a road map. (B) Dissection of the vessel found after a run. (C) Good distal circulation from the dominant right vertebral artery. (D) Three month follow-up MR angiography after conservative management showing complete recanalization.

{kind=link}
{kind=link}
{kind=link}
(A) Dissection of the left internal carotid artery following intervention for a temporal arteriovenous malformation (AVM). (B) Immediate anticoagulation and stenting done with good flow restoration. (C) Six month follow-up angiogram showing healing of the dissection, good flow restoration with preservation of the vessel for further embolization of AVM.
Heparin has been the standard management of care in the initial phase of treatment. Good outcome has been reported.8 Hart et al recommend regimens using heparin for 7 days and Coumadin for 3 months, and recommend antiplatelets only when Coumadin is contraindicated.9 In the pre-endovascular era, surgical treatment for cases refractory to medical treatment such as endarterectomy, resection with grafting, extracranial–intracranial bypass and occlusion of the parent artery were used.10 Most have become obsolete as most cases can safely be dealt with by stenting of the vessel.
In patients presenting with neurological deficit, the role of intravenous tissue plasminogen activator (tPA) is controversial as many fear the dissection would progress with intravenous tPA. Derex et al are of the opinion not to rule out the benefit of tPA in stroke related to dissection and feel further evaluation of intravenous and intra-arterial tPA is needed in stroke related to cervicocerebral artery dissection to address the efficacy of thrombolysis in this setting.11 In patients presenting with a major vessel occlusion due to thrombosis or embolism, immediate mechanical thrombectomy with or without stenting of the dissected vessel is to be considered as an option. The use of acute endovascular stroke therapy for a large artery ischemic stroke secondary to arterial dissections involves modifications to the conventional procedural protocol.12 There should be careful manipulation of any microcatheters, wires and devices across the arterial dissection, as well as keeping the large bore guiding catheter proximal to the dissection and use of large suction force to retrive the clot. However, we have not encountered such a situation.
We followed-up 94% of patients. Excellent outcome in terms of caliber of the vessel and absence of neurologic deficit was found in 94% of the followed-up cases. For follow-up, cervical angiography is the study of choice13 and it is the most sensitive. MR imaging and MR angiography are useful non-invasive techniques for follow-up (figure 2). After the first few days, intramural hematoma become hyperintense in both T1 and T2 weighted images14 and it can be well visualized in fat suppression images to suppress the surrounding fat.15 It remains hyperintense for a period of a few months. Depending on the type of dissection, orientation of the vessel and plane of imaging the appearance can be a curvilinear, cresentric band or a small focus adjacent to the lumen.14 Duplex ultrasonography is a sensitive tool in selected cases with dissections at locations accessible to the tool. In cases with cervical carotid dissections, this is a useful tool. Steinek et al have reported an interval from the onset of symptoms to sonographic recanalization of the dissection of 2 days to 1 year, with most dissections recanalizing during the first 2 months.16
Conclusion
Iatrogenic dissection is a random event, not related to the catheter or guidewire used but to the manipulation during the procedure. A high index of suspicion of detecting them early and treating them aggressively has resulted in excellent outcomes in recanalization of the vessel and in prevention of thromboembolic complications. Although angiography is the best modality for follow-up of these patients, non-invasive imaging such as MRI with MR angiography and duplex ultrasonography are good tools to follow the dissections.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.