Article Text

Abstract
Purpose Recanalization using intra-arterial fibrinolytic therapy in combination with mechanical clot disruption may be a more effective strategy for early reestablishment of cerebral blood flow in acute ischemic stroke. To validate our hypothesis, we evaluated a prototype balloon infusion wire (NeuroInterventions, Pittsburgh Pa) for delivering rtPA directly within the clot and compared its performance with the HyperGlide compliant balloon (eV3 Neurovascular, Irvine, CA) and microcatheter directed rtPA infusion in a rabbit common carotid artery (CCA) thromboembolic occlusion model.
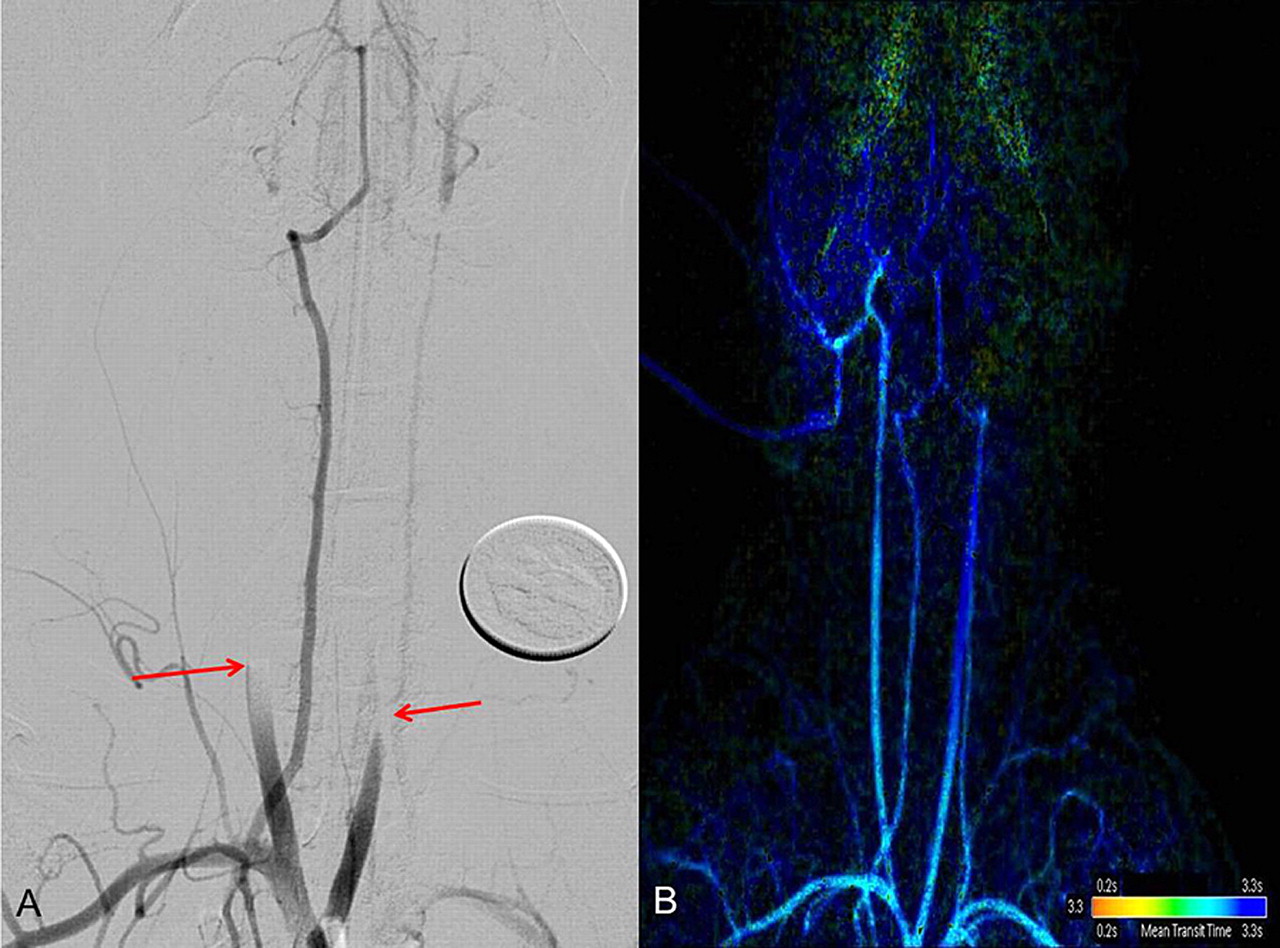
Materials and Methods New Zealand white rabbits (n=7) were selected for this work due to their similar response to rtPA as in humans. They were anesthetized and >50% luminal stenosis of the CCA was created bilaterally with 3-0 silk suture. Allogenic clot was injected through a 6F guide catheter and lodged consistently in the CCA proximal to the stenosis (arrows, A). The stenosis was released one hour post clot injection allowing sufficient time for clot-vessel lumen interaction. DSA was performed bilaterally to confirm the occlusion and assess the Thrombolysis in Cerebral Infarction (TICI) score. Each vessel was assigned to receive the device, balloon angioplasty, or microcatheter directed rtPA. The negative control group received no therapy. The primary endpoint was flow restoration. The secondary endpoint was time to recanalization and vascular safety, which was assessed by histological response on luminal scanning electron microscopy (SEM) and H&E staining. An assessment of the vascular safety from controlled operation of the infusion device and balloon occlusion in unembolized rabbit CCA was also made.
Results We successfully created consistent thromboembolic occlusions with TICI 0 flow at the predetermined location within the CCA. The balloon infusion wire achieved an earlier recanalization with a TICI 2B score (B, 2D perfusion post MTT) in 14 min requiring 2.8 mg rtPA. In comparison, microcatheter directed rtPA achieved TICI 2B score in 29 min requiring 4 mg rtPA. Balloon angioplasty, when used alone, achieved an inferior TICI 2A final recanalization score in 20 min post treatment and often failed to recanalize the CCA. Histomorphometry and luminal SEM evaluation revealed that the operation of the infusion device is comparable to balloon angioplasty with endothelial cell denudation and an exposure of the internal elastic lamina, an acceptable level of disruption for mechanical revascularization devices.
Conclusion Combined pharmaco-mechanical disruption achieves a high recanalization grade with a lower thombolytic dose more rapidly in comparison to either therapy (balloon angioplasty and thrombolysis) used alone.
{kind=link}
Statistics from Altmetric.com
Footnotes
Disclosures M Gounis: This work was supported by Neurointerventional Therapeutics. R Nogueira: Consultant for Neurointerventional Therapeutics. M Mehra: None. E Finol: Founder of Neurointerventional Therapeutics. Y Yang: Neurointerventional Therapeutics. S Jahrmarkt: Neurointerventional Therapeutics. M Migliuolo: Neurointerventional Therapeutics. A. Wakhloo: None.