Article Text

Abstract
Background and purpose With mechanical thrombectomy (MT), 0–4.5hr patients ineligible for IV tPA likely benefit from recanalization therapy, and >4.5 hr patients may also benefit. However, limited centers provide MT. To transfer all high NIHSS patients for MT would be inefficient and costly, as NIHSS has been demonstrated to be of somewhat limited value as a surrogate for large vessel occlusion (LVO). We identify an NIHSS subset analysis that initial evaluators can use to help identify LVO patients, for whom MT may be beneficial.
Methods Acute strokes presenting to VUMC from 2012 to 2013 (779) were evaluated for presentation NIHSS. All patients had vascular imaging and 125 demonstrated LVO. Modified receiver operating characteristic (ROC) curves were generated for each combination of three NIHSS items. Subsets were ranked by a modified area under the curve (AUC). False negative rates could not exceed 80%, enabling comparison of each combination's specificity for LVO while ensuring >20% sensitivity.
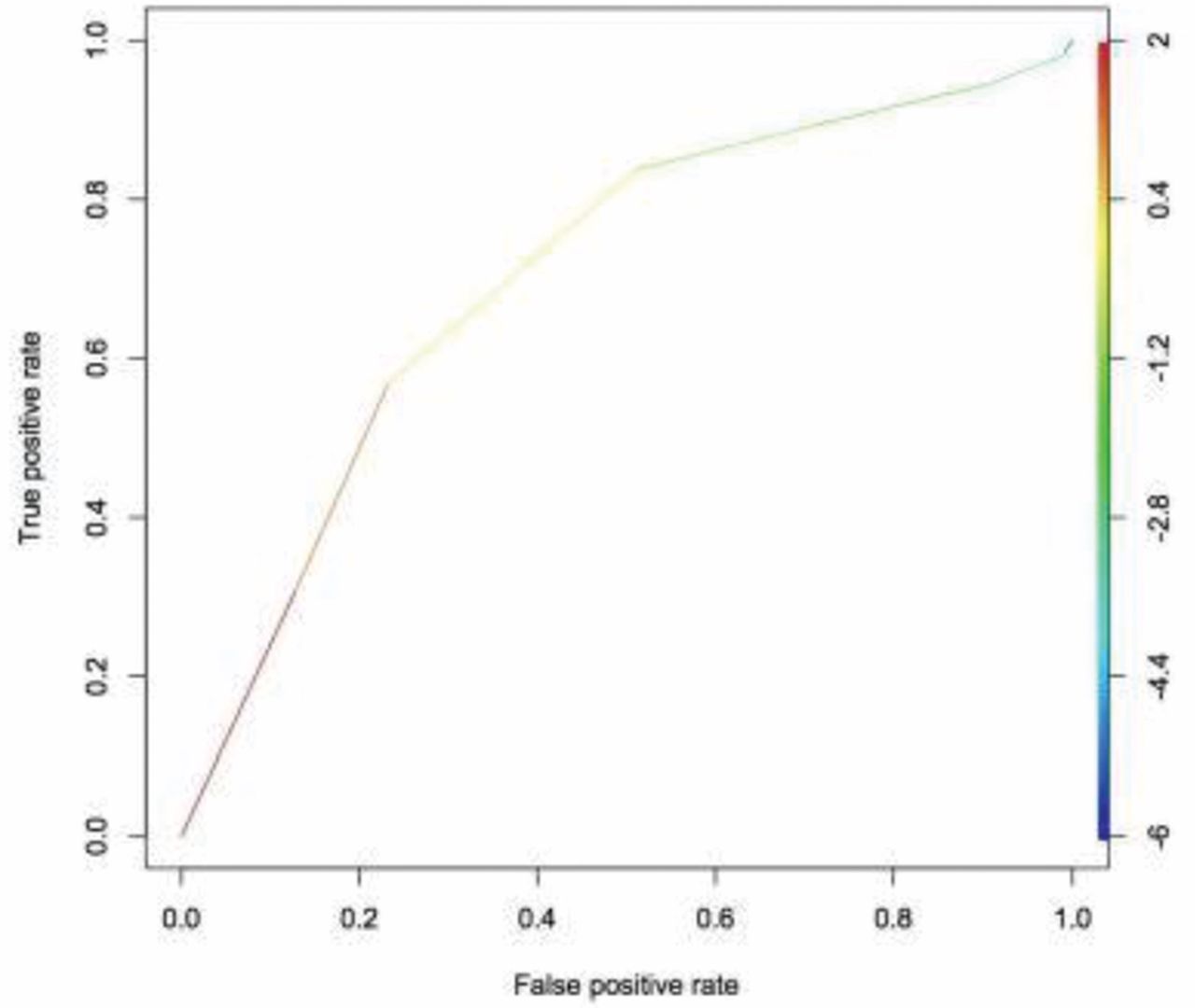
Results The 3 NIHSS subset with the largest modified AUC was “Facial Palsy”, “Language”, and “Extinction”. Given that “Language” could bias selection towards left hemisphere stroke, we identified the best AUC subset after excluding “Language”: “Level of Consciousness - Questions”, “Facial Palsy”, and “Extinction”. Using 4 out of 7 possible points as cutoff, these criteria have 89.3% specificity and 28.8% sensitivity for LVO. Figure 1 shows the modified ROC curve.
Conclusion We present a three-item score, derived from the NIHSS that is 89% specific for LVO. Hospitals without MT capabilities can use this easy to implement score to identify patients, with a likelihood of being correct for 9/10 referrals, who may benefit from transfer to a MT providing center. However, in order to maximise specificity, we have chosen to settle for only 29% sensitive, with 2/3 of LVO not being detected. While non-ideal, it is hoped that this scale may provide a reasonable balance of resource utilization and potential patient benefit.

{kind=link}
Modified ROC curve for predicting LVO
Disclosures S. Zuckerman: None. A. Sivaganesan: None. C. Zhang: None. M. Dewan: None. P. Morone: None. J. Mocco: None.