Article Text

Abstract
Objective The goal of this work was to endothelialize silicone aneurysm tubes for use as in vitro models for evaluating endothelial cell interactions with neurovascular devices. The first objective was to establish consistent and confluent endothelial cell linings and to evaluate the silicone vessels over time. The second objective was to use these silicone vessels for flow diverter implantation and assessment.
Methods Silicone aneurysm tubes were coated with fibronectin and placed into individual bioreactor systems. Human umbilical vein endothelial cells were deposited within tubes to create silicone vessels, then cultivated on a peristaltic pump and harvested at 2, 5, 7, or 10 days to evaluate the endothelial cell lining. A subset of silicone aneurysm vessels was used for flow diverter implantation, and evaluated for cell coverage over device struts at 3 or 7 days after deployment.
Results Silicone vessels maintained confluent, PECAM-1 (platelet endothelial cell adhesion molecule 1) positive endothelial cell linings over time. These vessels facilitated and withstood flow diverter implantation, with robust cell linings disclosed after device deployment. Additionally, the endothelial cells responded to implanted devices through coverage of the flow diverter struts with increased cell coverage over the aneurysm seen at 7 days after deployment as compared with 3 days.
Conclusions Silicone aneurysm models can be endothelialized and successfully maintained in vitro over time. Furthermore, these silicone vessels can be used for flow diverter implantation and assessment.
- aneurysm
- device
- flow diverter
Data availability statement
Data are available upon reasonable request. Any detail related to the model or the results are available from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Flow diversion can be a successful approach for treating cerebral aneurysms.1–3 The flow diverter is deployed across the aneurysm to reduce intra-aneurysm flow, reconstruct the parent artery, and ultimately achieve aneurysm occlusion.4 Preclinical models are critical for evaluating flow diverters during development, and useful models can include complex aneurysm geometries and/or the cellular environment of an aneurysm.
Preclinical device assessments include benchtop, in vitro and in vivo models. Benchtop models often use clinical or anatomically relevant data to produce 3D silicone replicas as a mechanism for device testing, physician training, and other clinical research.5–8 These models can accurately capture complex geometries, but they typically lack cellular or biologic components. Recent work has documented the incorporation of cells in polydimethylsiloxane (PDMS) benchtop models, but these models were focused on hemodynamic and genetic studies and were not used for device testing.9 10 The most common in vivo preclinical model for flow diverter assessment is the rabbit elastase-induced aneurysm model, which allows evaluation in a complex physiologic environment that includes relevant geometries as well as cellular components.4 11 12 However, these models require advanced techniques and facilities, and can be costly for early-stage assessments.
In vitro aneurysm models have the potential to serve as precursors to animal models by combining the anatomically accurate and well-controlled geometries of benchtop models with simplified cellular components, in a cost-effective and scalable way. Our laboratory focuses on creating these in vitro models, which we refer to as “aneurysm blood vessel mimics”. Previous work has incorporated traditional tissue engineering approaches, using electrospun polymer scaffolds to create custom aneurysm geometries and incorporating human endothelial and smooth muscle cells.13 14 However, electrospinning has some limitations with complex geometries such as saccular necks with tight angles. Many laboratories also do not have in-house customizable electrospinning capabilities such as those previously published.14 Given the extensive use of silicone models in the neurovascular field and the ability to create complex clinical geometries, silicone aneurysm models could be effective in vitro models if they supported consistent formation of endothelial cell linings and, importantly, if those cell linings could withstand device deployment. Previous work has shown the ability to endothelialize PDMS models,9 10 but assessment beyond 24 hours and the ability to use these types of models for device testing has not been shown.
Therefore, the goal of the current work was to endothelialize silicone aneurysm models in vitro, to assess these silicone vessels over time, and to implant as well as evaluate flow diverters in these vessels. The first set of experiments focused specifically on establishing consistent and confluent human endothelial cell linings in silicone models and evaluating the resulting silicone vessels at varying time points. The second set of experiments focused on flow diverter implantation to determine whether the endothelial cell lining in silicone vessels can withstand device deployment and whether the model can subsequently be used to evaluate the endothelial cell response to flow diverters over time.
Materials and methods
Silicone aneurysm preparation
Silicone aneurysm tubes were obtained from Stryker Neurovascular. Tubes were 43 mm in length with an inner diameter of 4.0 mm, and incorporated an aneurysm with a 2.4 mm neck and 3.1 mm height (figure 1A). Silicone tubes had barbed fittings placed, and were submerged in sterile 70% ethanol then flushed with 1 x Tris-buffered saline. A 20 µg/mL fibronectin solution (MilliporeSigma, F1141) was injected into each silicone aneurysm tube and incubated statically for 1 hour at 37°C and 5% CO2. Coated tubes were then transferred into individual sterile bioreactors (figure 1B).

Silicone aneurysm tubes and bioreactor system configuration. Silicone aneurysm tubes were 43 mm in length, with 4.0 mm internal diameter, and incorporated aneurysms with a 2.4 mm neck and 3.1 mm height (A). Silicone aneurysm tubes were coated with fibronectin then placed in individual bioreactor chambers prior to cell deposition (B). Individual bioreactor systems were connected to media reservoirs, placed on peristaltic pumps, and run at 37°C and 5% CO2, before and after cell deposition (C).
Bioreactor preparation
Details of bioreactor systems have been published previously with electrospun blood vessel mimic work.15 Briefly, each bioreactor system contained a vessel chamber connected with gas permeable tubing to a media reservoir. The vessel chambers were filled with M199, supplemented with penicillin/streptomycin, fungizone, HEPES buffer, and L-glutamine. The reservoir chambers were filled with endothelial cell media (Lonza, CC-3156). Fibronectin-coated silicone tubes were aseptically mounted into vessel chambers, then each system was connected to a Masterflex L/S Cole-Parmer 8-roller peristaltic pump (figure 1C). Flow was initiated at the lowest setting to perfuse the system with endothelial cell media prior to cell deposition.
Cell culture, cell deposition, and vessel cultivation
Human umbilical vein endothelial cells (HUVECs, Lonza, C2519A) were cultured at 37°C and 5% CO2 with endothelial cell media (Lonza, CC-3156). HUVECs were passed a maximum of six times using 1:2 and 1:3 split ratios until a sufficient cell population was obtained. HUVECs were harvested from culture flasks and resuspended in endothelial cell media. For each vessel, approximately 4–6 million HUVECs were resuspended in 1 mL of media, then deposited into coated silicone tubes by injecting cells through the proximal stopcock using a syringe. Following cell injection, a small amount of additional media was used to push the cell solution into the silicone tube. Each bioreactor chamber was then returned to the incubator, rotated 90° every 2 min for three rotations, then rested statically. No cells or media were circulated during this time. One hour after cell deposition, steady flow was initiated from the media reservoir (containing fresh endothelial cell media) using the peristaltic pump at a low flow rate of 15 rpm and gradually increased to 90 rpm (4.7 mL/min) over 24 hours. Systems were then maintained for 2, 5, 7, or 10 days for assessment of silicone vessels over time, and media reservoirs were changed with fresh media every 2 days. A subset of vessels was used 2–4 days after cell deposition for device deployment.
Device deployment
Bioreactor systems designated for device implantation were removed from the pump and incubator 2–4 days after cell deposition and brought into the biological safety cabinet. In each silicone aneurysm vessel, a 4.5×15 mm self-expanding CoCr and Pt braided prototype flow diverter (supplied by Stryker Neurovascular) was deployed aseptically across the aneurysm. Devices were visually placed without the need for fluoroscopy or guided imaging systems. Treated vessels were returned to the pump and incubator and maintained for 3 or 7 days. Additional silicone vessels remained untreated as controls.
Harvesting and fixation
Silicone aneurysm vessels without devices were harvested from bioreactor systems at 2, 5, 7, and 10 days after cell deposition for vessel assessment over time. Silicone aneurysm vessels with implanted flow diverters were harvested at 3 and 7 days after deployment, along with a set of untreated controls. Vessels were fixed in 4% paraformaldehyde. After fixation, each silicone vessel (with or without an implanted flow diverter) was cut longitudinally such that the aneurysm was fully contained in one longitudinal half. Fixed longitudinal sections were stored at 4°C in 1 x Tris-buffered saline until staining and imaging.
Silicone aneurysm vessel staining and imaging
Fixed longitudinal sections that contained the aneurysm dome, with or without devices, were stained with the nuclear stain bisbenzimide (BBI, Abcam, ab145597) then imaged under fluorescent microscopy to visualize and quantify cell presence. Longitudinal sections that solely contained parent vessel sections, with or without devices, were stained with hematoxylin and eosin (H&E) by submerging in hematoxylin, deionized water, then eosin to visualize the morphology of the endothelial cell lining. These samples were imaged under white light microscopy.
Image analysis and BBI quantification
For vessels without devices, 10× BBI images were used to visualize and quantify endothelial cell deposition along the length of each vessel. Images were analyzed using a custom ImageJ macro to count nuclei, and cell density was calculated for each image. An average cell density was then calculated for each vessel. For interpretation purposes, literature has shown that endothelial cell density in human vasculature is in the range of 112 000 to 132 000 cells/cm2.16 17 For vessels with devices, 10× BBI images were also used. Cell adherence on device struts was evaluated by manually counting BBI-stained cell nuclei in seven representative sections of each flow diverter and averaged to provide cell counts per flow diverter strut.
PECAM-1 staining
An additional set of straight silicone vessels was created and cultivated to visualize endothelial cell expression in the model through immunostaining. These vessels were harvested at 2, 5, and 7 days after cell deposition. The vessels were fixed in 100% ice-cold methanol and washed three times in cold phosphate-buffered saline (PBS), then cut longitudinally. The samples were blocked using a solution containing 10% donkey serum, 22.52 mg/mL glycine, and 0.1% Tween 20 in PBS for 30 min. After blocking, samples were exposed to the CD31 primary monoclonal antibody (1:200, Abcam, ab24590), which was diluted in a solution containing 10% donkey serum and 0.1% Tween 20 in PBS, for 1 hour. The primary antibody was then removed, samples were washed three times in PBS, and a 1:200 dilution of donkey anti-mouse secondary antibody (Abcam, ab150105), diluted in a solution containing 10% donkey serum and 0.1% Tween 20 in PBS, was added for 1 hour in the dark. After washing three times in PBS, samples were counterstained with BBI and imaged under fluorescence microscopy.
Data analysis
For vessels without devices, cell density was quantified for each image, and an average cell density was calculated for each vessel. These average densities were then used to obtain an overall average for each time point, with data represented as mean±SE. For vessels with devices, the number of cells on each strut region was quantified and used to calculate an average for each time point, represented as mean±SE.
Results
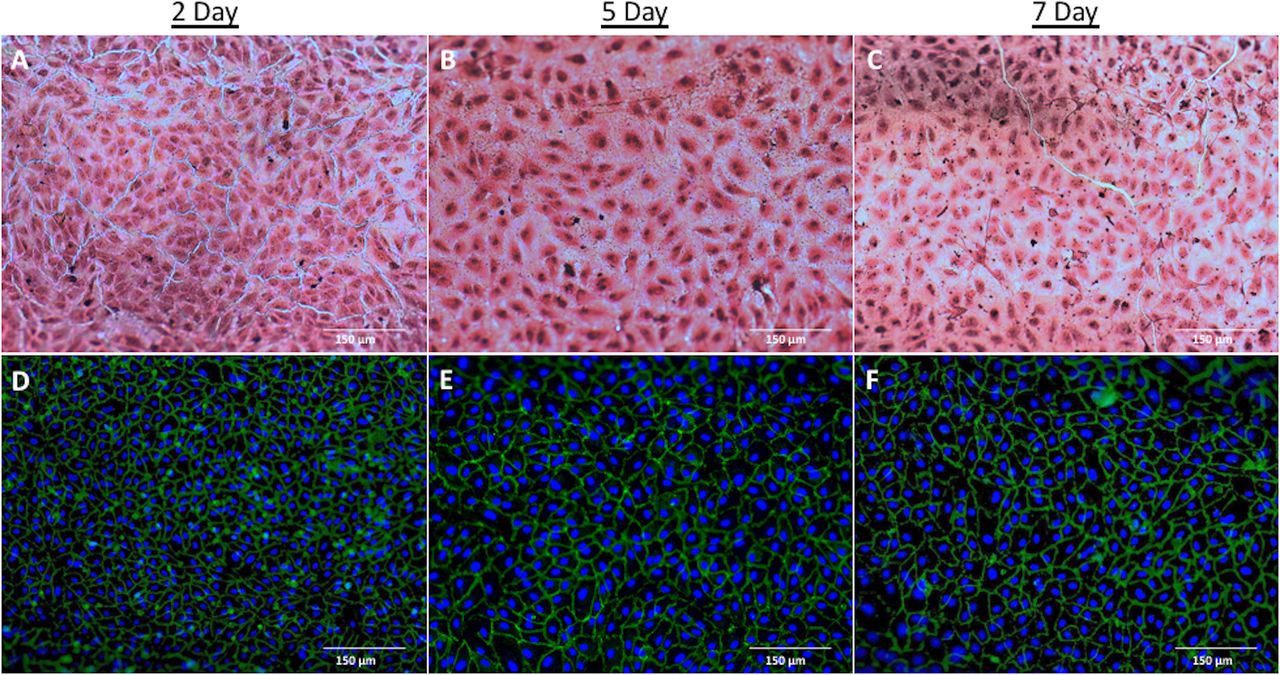
Silicone tubes successfully supported endothelial cell deposition and maintenance of the endothelial cell lining over time. H&E images along the vessel walls qualitatively revealed a consistent and confluent cell lining with the cobblestone morphology expected of endothelial cells (figure 2A–C). Platelet endothelial cell adhesion molecule-1 (PECAM-1) staining confirmed that endothelial cells maintained their phenotypic expression in silicone vessels over time (figure 2D–F).
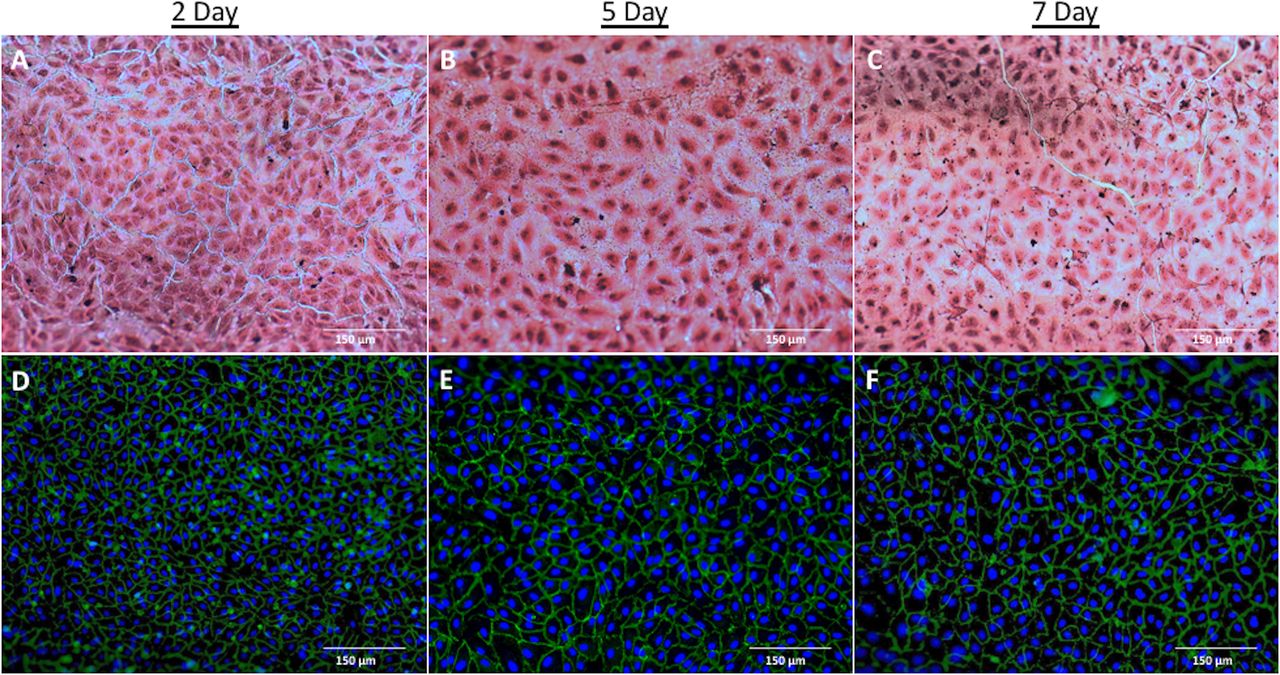
Establishment and maintenance of endothelial cell linings in silicone vessels. H&E images taken under white light microscopy illustrated consistent and confluent cell linings over time (A–C). Fluorescent microscopy was used to confirm endothelial cell phenotype through PECAM-1 (platelet endothelial cell adhesion molecule 1) staining (green) with bisbenzimide nuclear counterstaining (blue) over time (D–F).
Silicone aneurysm vessels facilitated and withstood flow diverter implantation. Device deployment was performed efficiently and consistently, with flow diverters successfully centered within the aneurysm vessel each time. H&E images from the parent vessel sections revealed that cell linings remained intact following device deployment (figure 3A and D). BBI images from the longitudinal sections containing the aneurysm dome further confirmed that cells were present on the silicone vessel underneath, and cell coverage of device struts illustrated that cells were able to respond to the implanted devices (figure 3B–C and E–F).

Evaluation of flow diverters in silicone aneurysm vessels after 3 and 7 days. H&E images revealed an intact cell lining beneath implanted flow diverters, indicating the cell linings were robust enough to withstand device deployment (A, D). Bizbenzimide (BBI) images illustrated cell coverage on device struts, including over struts at the neck where the slope of the aneurysm began (B, E), as well as over struts in the center of the aneurysm (C, F). These images illustrate the ability to evaluate cell response to implanted flow diverters. The 3D model, at the left, shows where various images were obtained, with the parent vessel section for H&E images on the left, and the section containing the entire aneurysm dome for BBI images next to it.
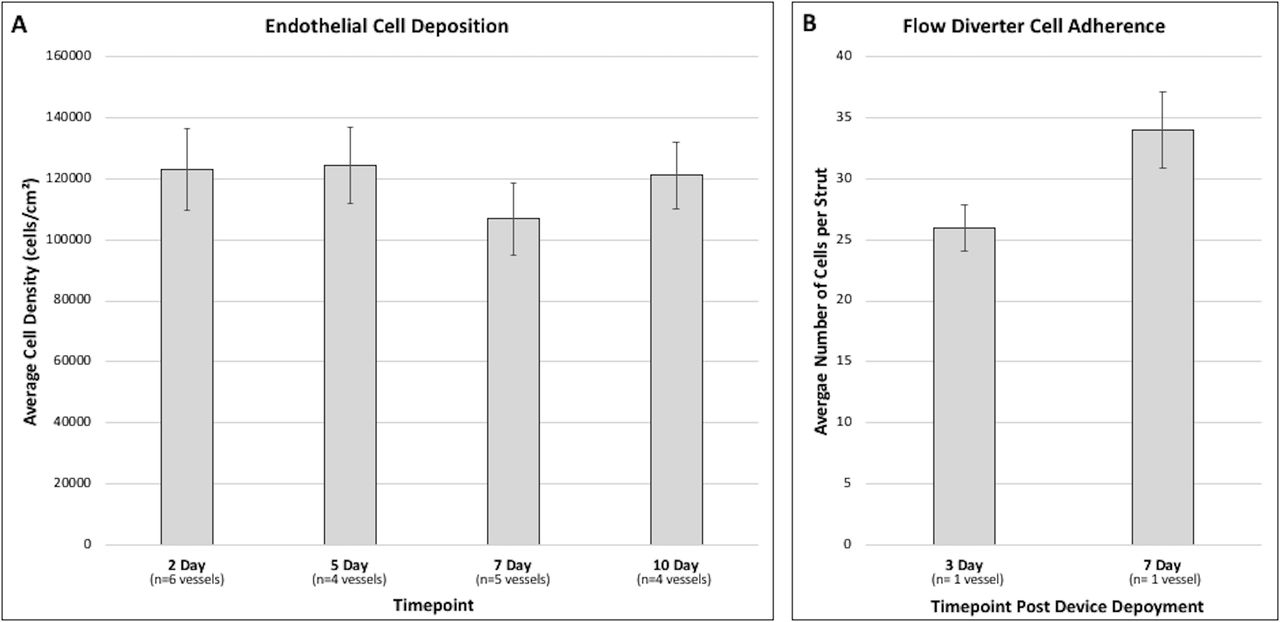
In addition to the qualitative images showing that endothelialized silicone aneurysm vessels can be successfully maintained over time and used for flow diverter implantation, quantitative cell counts were used to compare cell density on silicone vessels and to compare cell coverage on device struts. For vessel assessment over time, images were obtained and quantified from 19 different vessels at either 2, 5, 7, or 10 days. Results indicated that the average cell density ranged between 106 815 cells/cm2 and 124 209 cells/cm2 for each time point, suggesting an appropriate endothelial cell lining was established and maintained (figure 4A).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Quantification of endothelial cell density in silicone vessels over time, and cell adherence on flow diverter struts. The average cell density in silicone vessels was between 106 815 cells/cm2 and 124 209 cells/cm2 for each time point, demonstrating that an appropriate endothelial cell lining was established and maintained (A). In silicone vessels treated with flow diverters, quantification of cells per strut illustrated a higher amount of cell coverage on average after 7 days, as compared with 3 days after deployment (B), suggesting that endothelialized silicone vessels can be used to evaluate cell responses to implanted flow diverters.
For the flow diverter vessels, cell coverage on device struts over the aneurysm center was manually counted. The chosen strut region size was somewhat arbitrary, but it was consistent. Therefore, the average cell counts across consistently sized regions allowed a comparison between time points. Cell counts revealed an average of 34 cells/strut region at 7 days as compared with an average of 26 cells/strut region at 3 days after deployment (figure 4B).
Discussion
These studies demonstrate that traditional neurovascular models made of silicone can be endothelialized to create silicone vessels for flow diverter implantation and assessment. The first set of experiments illustrated that it was possible to successfully and consistently deposit a lining of human endothelial cells within silicone aneurysm tubes, and these confluent cell linings were maintained over time. This required optimization of the fibronectin concentration and coating protocol as well as the cell deposition procedure. The work presented here resulted in confluent endothelial cell monolayers with a cobblestone morphology and positive PECAM-1 staining.
The second set of experiments illustrated that it was possible to implant and evaluate flow diverters within endothelialized silicone aneurysm vessels. This required an initial assessment of whether the cell lining could withstand device deployment, followed by evaluation of the cell response at 3 and 7 days after deployment. Results illustrated that cell linings remained intact, and that cells responded to implanted devices through cell coverage of device struts. There was an increase in cell coverage at 7 days as compared with 3 days, suggesting that this model could be used to assess healing over time or to compare healing between different device configurations.
Although previous work has demonstrated the ability to electrospin custom aneurysm scaffolds to use in tissue-engineered aneurysm models, the present work using silicone has several key advantages. One significant advantage is that the creation of silicone tubes for benchtop models is fairly common in the neurovascular field, whereas electrospinning is more specialized and less common. Silicone models also allow greater complexity, with geometries that can be created to match specific clinical geometries.6 7 9 10 Electrospinning is limited in its ability to create certain complex geometries, especially saccular necks with tight angles.14 Silicone is non-degradable and stable for a longer time, as compared with degradable polymers often used in electrospinning. Additionally, silicone is transparent in comparison with opaque electrospun polymers, which allowed for very straightforward deployment through purely visual placement.
Previous work by others that endothelialized PDMS and silicone models has focused on hemodynamics and genetic expression.9 10 18 Kaneko et al 9 replicated a basilar aneurysm clinical scan to study the biological effect of complex flow stress on endothelial cells. Similarly, Levitt et al 10 created an aneurysm from a patient’s angiogram to study the correlation between endothelial cell expression and wall shear stresses. Both studies illustrated the ability to endothelialize vascular PDMS models. However, time points were limited to 24 hours after cell deposition, and no devices were implanted. To our knowledge, no endothelialized silicone or PDMS-based model has previously deployed or assessed devices.
As compared with more standard benchtop models or in vivo models, we believe these in vitro models can serve a unique role in the progression of preclinical testing. Standard silicone benchtop models provide effective assessments for early device testing, physician training, and hemodynamic studies. However, they typically lack relevant cellular and biological components.5–8 The rabbit elastase-induced model is a well-established model for assessing neurovascular devices4 19–21 and is biologically comprehensive with relevant geometries,22–24 but the complex geometries may be difficult to control within and between animals. Additionally, advanced imaging, infrastructure, and animal facilities are required for in vivo device studies. In vitro silicone aneurysm models combine the easily controlled complex geometries of benchtop models with simplified cellular components in a cost-effective and scalable model that does not require advanced infrastructure or imaging equipment.
Although many advantages to an endothelialized silicone aneurysm model exist, the in vitro model and the work presented here have several notable limitations. First, this model is limited in its ability to replicate the complex physiological environment of a cerebral aneurysm. There are no circulating cells, the vascular cell lining is limited to endothelial cells, and the low flow environment does not accurately recapitulate the in vivo conditions. These components could be partially addressed through incorporation of more cell types and customized bioreactor flow circuits. For example, previous work has incorporated both endothelial cells and smooth muscle cells within in vitro aneurysm models,14 and physiologic flow environments have been incorporated in other in vitro models.10 Including more physiologic flow in this model would allow assessments of the interaction between wall shear stresses and device healing. However, for the current work, the focus was intentionally on creating a simple, scalable model, with flow adequate for nutrient supply, waste removal, and at least low levels of shear stress. Given the limitations, these simple models are probably best suited as precursors to more traditional and complex animal studies.
The current device work was limited to flow diverter evaluation at 3 and 7 days. Future work could evaluate longer times, as well as t=0 baseline comparisons, with more replicates for statistical comparisons. Different flow diverter coatings and configurations could be compared, or the model could also be used to assess other neurovascular devices. If intrasaccular devices were evaluated, it would be important to further characterize the cell lining and morphology within the aneurysm dome, as the current work focused on the vessel walls and neck region. Additionally, the geometry in this work was a relatively simple aneurysm, but future work could evaluate and incorporate more complex clinical geometries. These complex clinical geometries could be created using standard silicone manufacturing procedures or through 3D printing of other flexible polymers.9 10 25 26 More complex geometries may necessitate modified cell deposition methods, but it would expand the utility and application of the model.
Conclusion
The work presented here illustrates that silicone aneurysm models can be endothelialized and maintained in vitro over time, and these silicone vessels can be used for flow diverter implantation and evaluation of endothelial cell responses.
Data availability statement
Data are available upon reasonable request. Any detail related to the model or the results are available from the corresponding author.
Ethics statements
Acknowledgments
We would like to acknowledge Jason Provol for his assistance with the 3D model used to illustrate image location in Figure 3.
References
Footnotes
Contributors Concept planning and development of studies performed by AMC, GG, KOHC. Conduct of the study, aquisition and analysis of data performed by AMC, AT, SF. Writing of the article performed by AMC, KOHC. Critical review of the article performed by GG, AT, SF.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.