Article Text

Abstract
Background The flow diverting stent is a new and expansive tool in the endovascular therapy of complex intracranial aneurysms. We present our experience using SILK flow diverter (SFD) in patients with complex intracranial aneurysms, and a cost analysis.
Methods Between September 2010 and May 2012, 19 consecutive patients with 29 complex intracranial aneurysms were treated with SFD without the adjunctive use of coils. We retrospectively evaluated the technical aspects, thromboembolic events, adjunctive therapies, and short term results in patients with complex intracranial aneurysms treated with SFD. A cost analysis of patients who were treated with SFD was performed and compared with similar sized aneurysms coiled with stent assisted coiling.
Results The primary technical success rate was 100%. An adjunctive device was required in two of our patients. The technique related complication rate and the 30 day mortality and morbidity rates were 5% (1/20) and 10% (2/20), respectively. We had a total of 263 patient months of clinical and 166 patient months of imaging follow-up. Follow-up imaging revealed two asymptomatic occlusions of the parent artery. Complete occlusion of the aneurysm with fully patent parent artery was observed in 59% of patients where follow-up images were available. The cost analysis showed that the mean cost of treatment with SFD was significantly cheaper compared with the presumed cost of stent assisted coiling (p<0.001).
Conclusions The SFD provides a very feasible, efficient, relatively safe, and cost effective method to treat complex intracranial aneurysms without the use of adjunct coiling.
- Aneurysm
- Flow Diverter
Statistics from Altmetric.com
Introduction
Since the International Subarachnoid Aneurysm Trial (ISAT),1 endovascular coiling of intracranial aneurysms has become the preferred method of treatment in the majority of intracranial aneurysms. Coiling of large, fusiform, and wide neck aneurysms remains technically challenging. These aneurysms have a recurrence rate of approximately 20–30% after endovascular treatment,2 resulting in retreatment in 10–12% of patients.3 ,4 Adjuvant stenting was proposed in the mid 1990s, initially for fusiform aneurysms5 and more recently to support the neck region of intracranial saccular aneurysms and to prevent recurrence.6
The principle of reduced blood flow in the sac of an aneurysm after stent placement in the parent artery causing stagnation and thrombosis has been exploited in other anatomies. This approach has now been extended to the intracranial vasculature using a new range of implants designed to be sufficiently flexible for intracranial navigation. These new devices, termed flow diverters, recently became available for clinical use. The first flow diverter used in clinical practice was the SILK stent (Balt Extrusion, Montmorency, France) in early 2007. Other flow diverters are PIPELINE (Covidien, Massachusetts, USA) and SURPASS (Surpass medical, Miramar, Florida, USA). These are self-expanding flexible stents constructed of woven strands with low porosity to divert blood flow away from the aneurysm into the distal parent artery to exclude the aneurysm sac. Since the introduction of flow diverters, several thousand have been implanted across the world. Compared with the number of devices used, there have been relatively few publications on these devices with many unanswered questions.
The economic impact of flow diversion stents is another important issue, considering the substantial cost and number of stents used per patient. We present a series of consecutive cases of SILK flow diverters (SFD) implanted in our center with a short term follow-up and a cost analysis of treatment of intracranial aneurysms using SFD.
Material and method
A retrospective review of our prospectively kept database in the Department of Neuroradiology for patients treated with SFD for an intracranial aneurysm, between September 2010 and May 2012, yielded 19 patients. The study was approved by our institutional ethics committee.
Patient selection
The treatment of patients with unruptured intracranial aneurysms was discussed in our neurovascular conference with four neuroradiologists and two neurosurgeons. We restricted our treatment to aneurysms that were either untreatable or were extremely difficult to treat by conventional endovascular or neurosurgical treatments.
Antiplatelet regimen
All patients were started on dual antiplatelet medications of aspirin (81 mg) and clopidogrel (75 mg) daily for 5 days before endovascular treatment. In cases where this could not happen, a loading dose of 325 mg of aspirin and 300 mg of clopidogrel was given on the first day followed by aspirin (81 mg) and clopidogrel (75 mg) daily until the day of endovascular treatment. Dual antiplatelet medications were continued for 3 months after treatment, followed by single antiplatelet medication for the rest of the patient's life. Platelet response to antiplatelet agents was not analyzed as the device used for this was not available in Canada until recently.
Technique
The SFD were deployed using a standard technique. All patients were treated with single SFD except two patients where a second SFD was used to stabilize the distal portion of the first SFD which moved in the aneurysm. Coils were not used in any of these patients. In one patient a LEO stent (Balt Extrusion) was used as a scaffold for the SFD. In five cases a 4 mm×10 mm Hyperglide non-detachable balloon (Covidian) was used for further opening or wall apposition.
A prophylactic 10 mg of dexamethasone intraoperatively followed by a tapering dose of dexamethasone for the next 6 days was given to all of our patients.
Follow-up
Patients were discharged from hospital on the day after endovascular treatment, except in the event of complications. They were followed in the neurovascular clinic 6 weeks after treatment. Imaging follow-up was done with CT angiogram (CTA) or MR angiogram (MRA) at 3 months, 6 months, and 1 year post treatment. If the aneurysm was completely occluded on CTA or MRA, the next imaging follow-up was with catheter angiogram to establish complete occlusion. After complete occlusion, patients were followed-up every 2 years to study the long term outcome (figure 1).

A 64-year-old patient (patient No 1) presented with gradual loss of vision in the right eye. Anteroposterior (A) and lateral (B) views of the right internal carotid angiogram showed a wide neck aneurysm arising from the communicating segment of the right internal carotid artery. This aneurysm was partially thrombosed with small calcification in the wall of the aneurysm on CT angiogram. Follow-up at 3 months after treatment (C, D), using a single 4.5×40 mm SILK flow diverter, showed no residual aneurysm and remodeling of the parent artery (arrows). The patient's vision improved after treatment.
Cost analysis
For cost analysis, the cost of device used only after placement of guiding catheter was assessed. On review of endovascular coiling of unruptured aneurysms in our institution, the minimum number of coils needed to occlude an aneurysm was not less than the largest diameter of the aneurysm itself. Based on this experience, the minimum number of coils per aneurysm was estimated to be the maximum diameter of the aneurysm. The cost of balloons or stents used was added. In patients with multiple aneurysms, cost analysis was performed only for the largest aneurysm. This estimated cost was then compared with the actual cost incurred in each patient for treatment with SFD. The cost of possible parent vessel occlusion was not estimated. Other costs were thought not to be significantly different between the two types of treatments in our hospital.
Although most of the aneurysms in our series could not have been treated with other endovascular techniques, this crude assumption was done to estimate the minimum possible cost of presumed endovascular treatment. This was probably a significant underestimation of the cost for the presumed stent assisted coiling.
Statistical analysis
To compare the actual cost with SFD and the estimated cost of presumed stent assisted coiling, a normality test showed that the data significantly deviated from normality. For this reason, a non- parametric test, the Wilcoxon signed ranks test, was used to compare the cost of the two methods of treatment. A p value less than 0.05 was considered significant.
Results
Between September 2010 and March 2012, a total of 19 patients (four men, 15 women; aged 20–83 years, median age 62 years) with 29 intracranial aneurysms were treated using SFD (see online supplementary table S1). Approximately 90% of our patients had large or giant aneurysms (median diameter 13 mm) and all had wide neck (median neck diameter 8 mm) aneurysms. We had a total of 263 patient months (mean 10.5 months; median 13 months) of clinical and 166 patient months (mean 9 months; median 7.5 months) of imaging follow-up. The technique related complication rate and the 30 day mortality and morbidity rates were 5% (1/20) and 10% (2/20), respectively.
Immediate postprocedural mortality
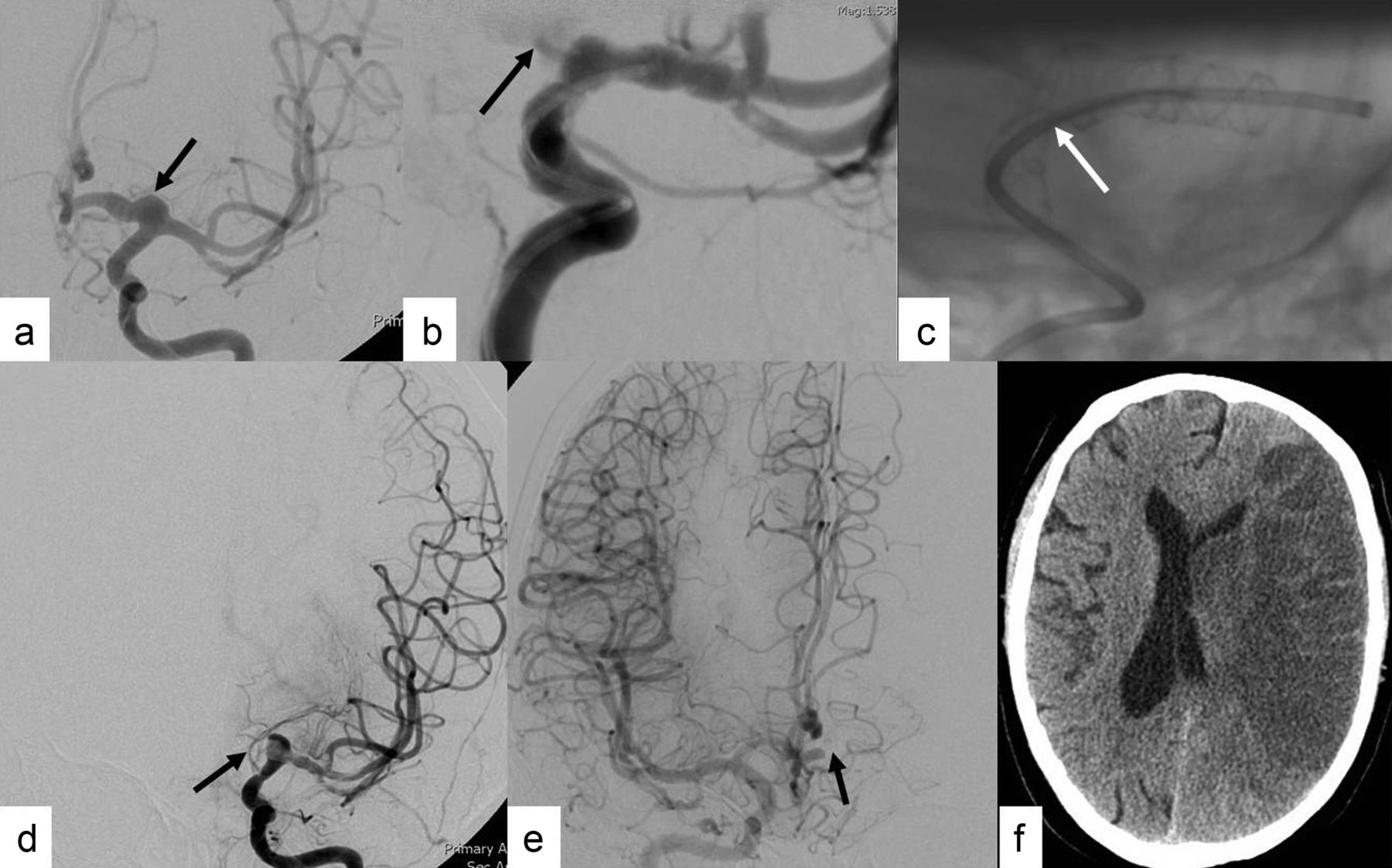
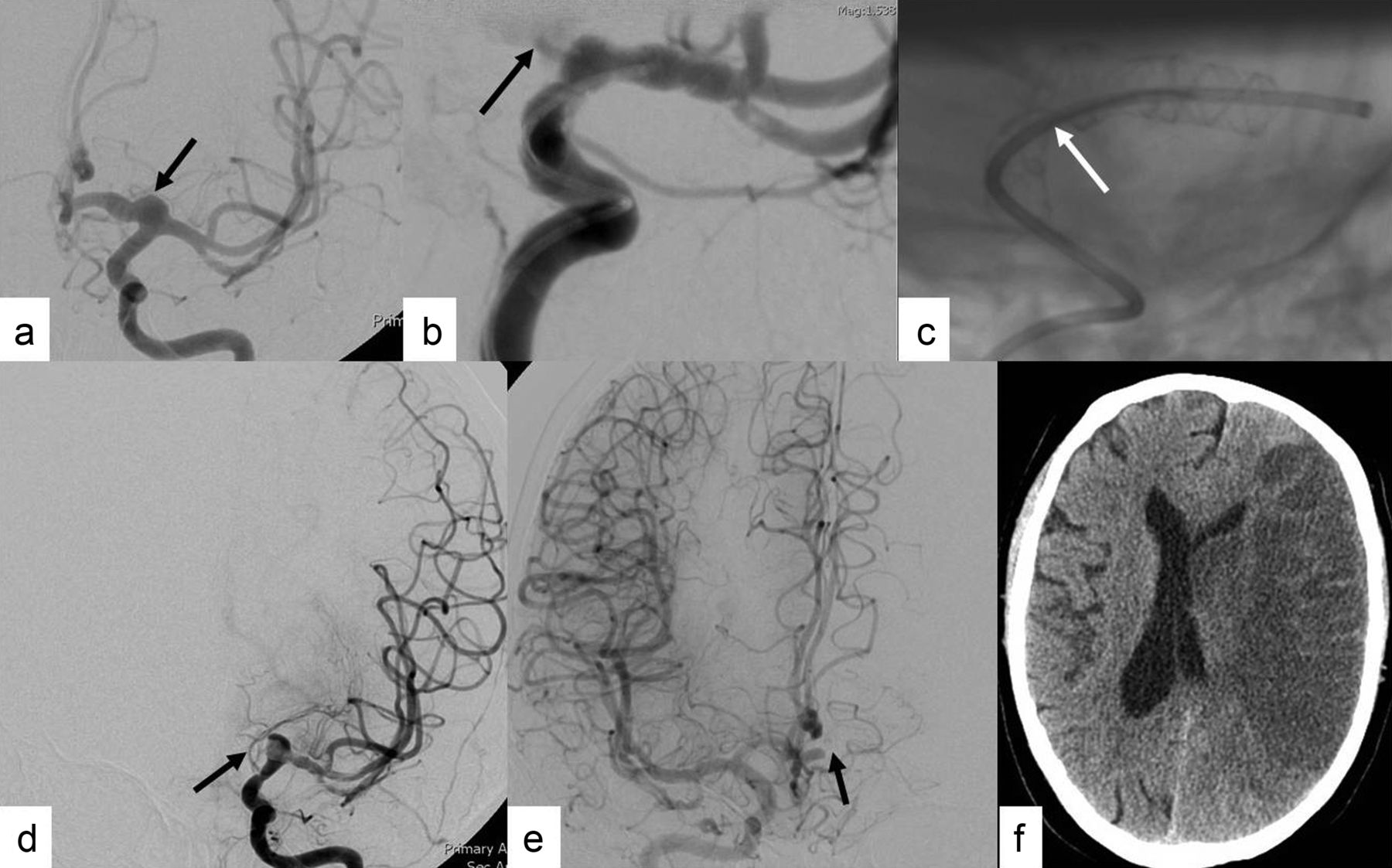
In patient No 13 the SFD did not appose the wall of the artery completely in its proximal aspect and balloon angioplasty was contemplated. On the control angiogram, thrombus formation was noted inside the stent, which did not respond to full dose intra-arterial Abciximab. The SFD could not be re-accessed and the SFD got pushed inside the A1 aneurysm, resulting in complete occlusion of the aneurysm and the A1 segment of the left anterior cerebral artery. This resulted in recanalization of the left internal carotid artery and the middle cerebral artery (MCA) in less than 1.5 h from the time of occlusion. Postoperative CT head showed a complete left MCA territory infarct. The patient had complete right-sided hemiplegia and aphasia but remained hemodynamically stable. He died of ventilator related complications in the intensive care unit 1 week after treatment. In retrospect, before pulling out the microcatheter, access across the SFD should have been maintained by placing an exchange length microguidewire through the SFD (figure 2).
{kind=link}
{kind=link}
A 70-year-old patient (patient No 13) with an incidentally discovered 10 mm×12 mm left A1 segment dysplastic/dissecting aneurysm (arrow) (A) found initially on a CT head done for headaches. The patient and family were highly apprehensive about the aneurysm and insisted on treatment. (B) The aneurysm was treated with a single custom made tapered SILK flow diverter (SFD) (P4.5D 3 mm×25 mm) from the M1 segment of the left middle cerebral artery (MCA) to the left internal carotid artery (ICA). Marked reduction in contrast filling in the aneurysm was noted immediately after deployment (arrow). (C) The SFD did not open completely and had a constriction at the ICA bifurcation. There was in-stent thrombus formation on the check angiogram. (D) The left MCA was reanalyzed within 1.5 h of occlusion with no residual filling of the aneurysm or the A1 segment of the left anterior cerebral artery (ACA) (arrow). (E) There was filling of the left ACA territory through the anterior communicating artery from the right ICA injection with no residual filling of the aneurysm (arrow). (F) However, the patient infarcted the whole left MCA territory on the follow-up CT scan. The patient remained hemodynamically stable and eventually died 1 week after treatment from intensive care unit complications.
Immediate postprocedural morbidities
Patient No 3, with a basilar trunk large aneurysm, developed mild weakness (power 4/5) of her left leg 12 h after treatment. MRI showed a questionable tiny focus of restricted diffusion on the right side of the brainstem which was already significantly compressed from the aneurysm. The patient improved over a week and walked out of hospital at discharge.
Patient No 16, with a left paraophthalmic wide neck large aneurysm, complained of word finding difficulty 12 h after treatment. Multiple tiny diffusion hits were seen in the left cerebral hemisphere, possibly from treatment. The patient improved spontaneously over the next 24 h and was discharged home 48 h postprocedure.
Delayed mortality and morbidity
We had 3 month imaging and clinical follow-up in 18 of our 19 patients. Follow-up imaging revealed two asymptomatic occlusions of the parent artery, both in the anterior circulation.
Patient No 2 had severe headaches 2 months post treatment and CT and MRI showed complete occlusion of the aneurysm as well as the parent artery. She admitted that she did not refill her prescription and was without aspirin and Plavix for approximately 2 weeks. The patient was given a 2 week course of dexamethasone and was restarted on dual antiplatelet medication for another 6 months. Her headaches improved in 1 week and she remained neurologically asymptomatic. However, her aneurysm and the parent artery continued to be occluded on follow-up imaging.
Patient No 7, after 6 weeks of treatment, complained of severe headaches. MRA showed complete occlusion of the aneurysm and the parent artery. The patient did not have any neurological deficits and did not show any diffusion hits on MRI. She admitted missing several doses of her antiplatelet medications. The patient was started on a 2 week course of dexamethasone and dual antiplatelet medications following which her headaches improved completely but the aneurysm and parent artery continued to be occluded.
Patient No 12, with a left cavernous segment aneurysm, had severe headaches 1 week after SFD treatment, which started after a binge of alcohol. Repeat CTA showed that the proximal aneurysm was completely occluded and the distal aneurysm was partially occluded with a patent parent artery. His headaches improved after 2 weeks of dexamethasone.
Patient No 16, with a left MCA fusiform aneurysm, continued to have headaches on follow-up. She later complained of jaw claudication and was diagnosed as having temporal arteritis.
Two months after treatment, patient No 9 died suddenly at home. The family refused autopsy, but initial complains suggested that a cardiac event was the most likely cause of death in this 77-year-old patient with severe heart disease.
Angiographic outcomes
Complete occlusion of the aneurysm with a fully patent parent artery was observed in 59% of aneurysms. All other aneurysms showed either incomplete occlusion or near complete occlusion. None of the aneurysms remained unchanged in size.
Cost analysis
The mean cost of treatment with SFD was significantly lower (p<0.001) compared with the presumed cost of stent assisted coiling in these patients.
Discussion
Flow diverter technology is an important paradigm shift in the endovascular treatment of aneurysms which focused mainly on filling of aneurysm with coils for the past 20 years. Flow diverter, as the name suggests, diverts the blood flow away from the aneurysm sac into the distal artery. This reduces the shear stress on the aneurysm wall and promotes stasis and thrombosis in the aneurysm. This phenomenon is affected by the pore density of flow diverters.7 The optimal porosity to achieve flow reduction appears to be 70% (1%).8 In theory, a flow diverter also provides a scaffolding for the development of endothelial and neointimal tissue across the aneurysm neck.
With more experience, the indications for flow diverter are expanding. We used flow diverters for complex aneurysms which were impossible or extremely difficult to treat using other endovascular or microsurgical approaches. We also included patients with segmental vessel wall disease with multiple aneurysms in the single arterial segment. Aneurysms located proximal to, at, and beyond the circle of Willis were included in our series.
Our experience supports the results of various other studies in the literature that SFD can be used safely in the treatment of complex intracranial aneurysm at different locations, including beyond the circle of Willis. We had procedural mortality and morbidity rates of 5% and 10%, respectively. One patient died of device related complications. Other studies have reported mortality rates ranging from 0% to 6%.9–11 The morbidity described in the literature ranges from 5% to 17.8%.10 ,12 ,13 The patient with left leg weakness was possibly secondary to swelling of the basilar trunk aneurysm mass causing compression of the brainstem or secondary to compression of the brainstem perforator. A similar phenomenon has been described in up to 25% of cases of basilar artery aneurysms.14 Flow diverters should be used with caution in basilar artery aneurysms. Compared with conventional endovascular treatment, morbidity and mortality appear to be higher with SFD. The aneurysms treated in our series with SFD were either untreatable or were extremely difficult to treat by conventional endovascular or neurosurgical treatment. Caution should be experienced in using SFD for aneurysms amenable to conventional treatment and should only be done in a trial.
One patient had a sudden death 2 months after treatment, probably from a cardiac related cause. Hemorrhagic complications from flow diverter treatment are described in the literature, in the range of 2% for the Pipeline and 0.8% for the SILK.15 Although the mechanism is not well understood, delayed rupture is frequently observed in symptomatic aneurysms (11/13 in Kulcsar's series), large and giant aneurysms (13/13 in Kulcsar's series), and aneurysms with a high aspect ratio.16
We observed delayed occlusion of the parent artery in two patients (10%). The incidence of parent artery occlusion has been reported to be as high as 14–28%.10 ,12 This prompts an important discussion of response/resistance of platelets to antiplatelet medications. We currently do not have any means of testing platelet response/resistance. The importance of this is being increasingly emphasized in the use of flow diverters. However, the method and results of these tests are yet to be standardized. Increased use of platelet inhibition assays will allow us to identify non-responders to these medications, and use of alternative antiplatelet agents may ultimately minimize thromboembolic complications.
At the 3 month imaging, we had complete occlusion of the aneurysms in 59% (11 patients) of successfully treated patients. The 3 month occlusion rate has been reported to range from 56% to 69%.12 ,17 Lylyk et al17 described complete angiographic occlusion in 56%, 93%, and 95% of cases at 3, 6, and 12 months, respectively. Szikora et al18 had complete occlusion in all but one aneurysm at 6 months. Both of these series used a Pipeline embolic device, in contrast with our series where we used SFD. Complete occlusion has been described in up to 68% of cases within 6 months in patients treated with SFD.9 In our study, we did not use any coils with the SFD. Whether use of coils in addition to the SFD scaffold across the neck would produce a higher rate of occlusion is unclear and needs to be studied in future studies.
The cost incurred by these devices is substantial, and multiple devices may be needed per patient. We believe we are the first study to discuss the cost effectiveness of flow diverters. Treatment with SFD was significantly cheaper (p<0.001) compared with presumed stent assisted coiling in our institution. The cost of treatment varies from center to center and operator to operator. If our study is any indication, wider application of SFD in the treatment of intracranial aneurysms may become cost effective. The EVIDENCE trial will compare the Pipeline device with endovascular coiling (with or without balloon or stent assistance) in large wide neck aneurysms in a prospective, multicenter, randomized study. This French trial will possibly be the first with both clinical and economic endpoints to measure the incremental cost effectiveness ratio of the Pipeline versus endovascular coiling.
Conclusion
The SFD provides a feasible, efficient, safe, and cost effective method of treating complex intracranial aneurysms without the use of adjunct coiling.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
▸ Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/neurintsurg-2012-010590).
-
The paper was presented at the Radiological Society of North America meeting 2012, Chicago, USA.
-
Contributors All authors contributed in various stages of manuscript preparation.
-
Competing interests None.
-
Ethics approval The study was approved by the CDHA ethics committee.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.