Article Text

Abstract
Large and giant aneurysms pose significant challenges to the endovascular techniques of coil embolization or parent vessel reconstruction. Many large aneurysms are wide-necked with bulbous domes and frequently require stent-assisted coiling or flow diversion to reconstruct and preserve flow through the parent artery. Often the wire must be looped in the dome before catheterization of the exiting portion of the parent vessel is possible. In addition, it can be challenging to obtain stable distal purchase of the microcatheter that will allow the loop to be withdrawn from the aneurysm without the entire microcatheter unwinding, resulting in herniation into the aneurysm or proximal vessels. The stent anchor technique, a novel method of obtaining distal purchase that allows straightening of the catheter loop within a large aneurysm for the purposes of stenting for vessel reconstruction across large or giant aneurysms, is presented. This technique may facilitate the use of new stent technologies in the treatment of large aneurysms that have traditionally been exceedingly difficult to treat via an endovascular approach.
- Aneurysm
- angiography
- flow diverter
- stent
- technique
- artery
- spinal cord
- subarachnoid
- thrombectomy
- catheter
Statistics from Altmetric.com
Introduction
Large and giant aneurysms pose significant challenges to the endovascular techniques of coil embolization or parent vessel reconstruction. Many large aneurysms are wide-necked with bulbous domes and frequently require stent-assisted coiling or flow diversion to reconstruct and preserve flow through the parent artery. A balloon anchor technique has been described previously1 in which the microcatheter, after gaining distal access, is exchanged for a balloon catheter which is then inflated in the distal vessel, thereby anchoring it and allowing for the loop within the aneurysm to be withdrawn without the catheter tip prolapsing back into the aneurysm. We present the stent anchor technique, a novel method of obtaining distal purchase that allows straightening of the catheter loop within a large aneurysm for the purposes of stenting for vessel reconstruction across large or giant aneurysms.
Case report
A woman in her 50s with multiple unruptured intracranial aneurysms, including a 15×15×15 mm right middle cerebral artery trifurcation aneurysm, presented for stent-assisted coil embolization (figure 1). She was initiated on aspirin and clopidogrel 1 week prior to the procedure.
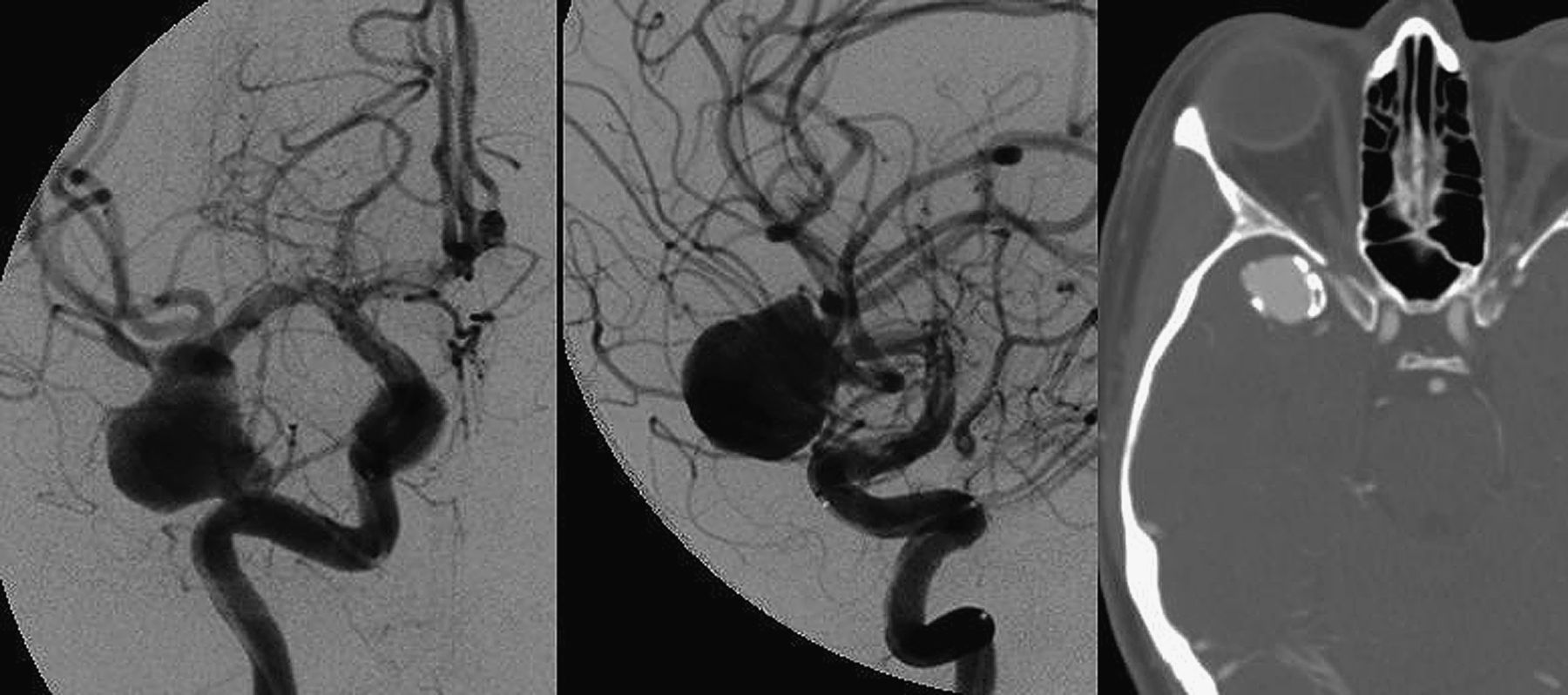
Anteroposterior (left panel) and lateral (center panel) views after right internal carotid artery injection, demonstrating the large 15 mm middle cerebral artery trifurcation aneurysm. Dense calcification is seen at the aneurysm neck on CT angiography (right panel).
Technique
Selective catheterization of the right internal carotid artery was performed using a 6 F 0.088 inch Neuron Max (Penumbra, Alameda, California, USA) after obtaining femoral artery access. Systemic heparinization was performed for a goal ACT of 250–300. A Prowler Select Plus microcatheter (Codman, Raynham, Massachusetts, USA) was advanced over a 0.014 inch Synchro-2 standard microwire (Stryker Corporation, Kalamazoo, Michigan, USA). The wire was advanced into the aneurysm and, using a loop technique, directed out of the superior M2 branch to traverse the aneurysm and gain access into the distal middle cerebral artery vasculature (figure 2). At this point, with the loop in place, an Enterprise 4.5×28 mm stent (Codman) was advanced into position within the distal Prowler Select Plus microcatheter. Next, a PX-400 microcatheter (Penumbra) was advanced over a Synchro standard wire (Stryker Corporation) into the intracranial circulation and positioned within the aneurysm in a jailing technique. The Prowler Select Plus microcatheter was then withdrawn slowly in an attempt to reduce the loop in the aneurysm. However, rather than straightening the microcatheter, the microcatheter simply unwound. This maneuver was therefore halted and instead the Enterprise stent was partially deployed to provide a distal anchor secondary to the stent's purchase with the distal vessel lumen. This allowed successful reduction of the loop in the aneurysm while the stent remained in position against the distal vessel wall. Once no excess catheter remained looped in the aneurysm, the stent was recaptured, ideally positioned across the aneurysm neck and then redeployed across the neck of the aneurysm in standard fashion to reconstruct the parent artery (figure 3). When this was completed, coil embolization was undertaken successively with the jailed microcatheter. At the conclusion of the procedure, Raymond grade III embolization had been completed with a small amount of residual dome filling (figure 4). The contrast in this remaining portion demonstrated significant stasis and therefore it was felt this was likely to progress to thrombosis. The patient tolerated the procedure without complication and is awaiting follow-up angiography.
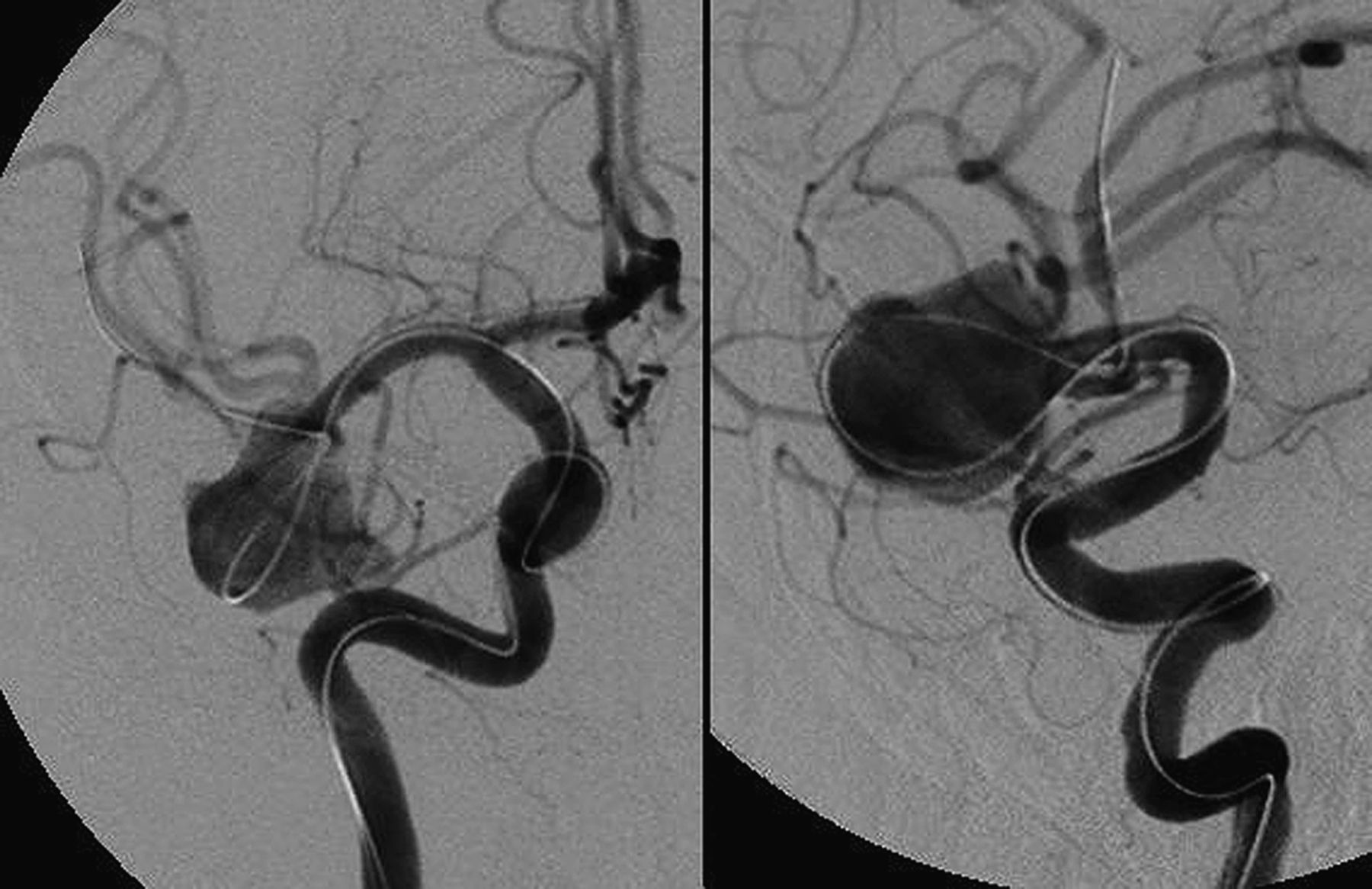
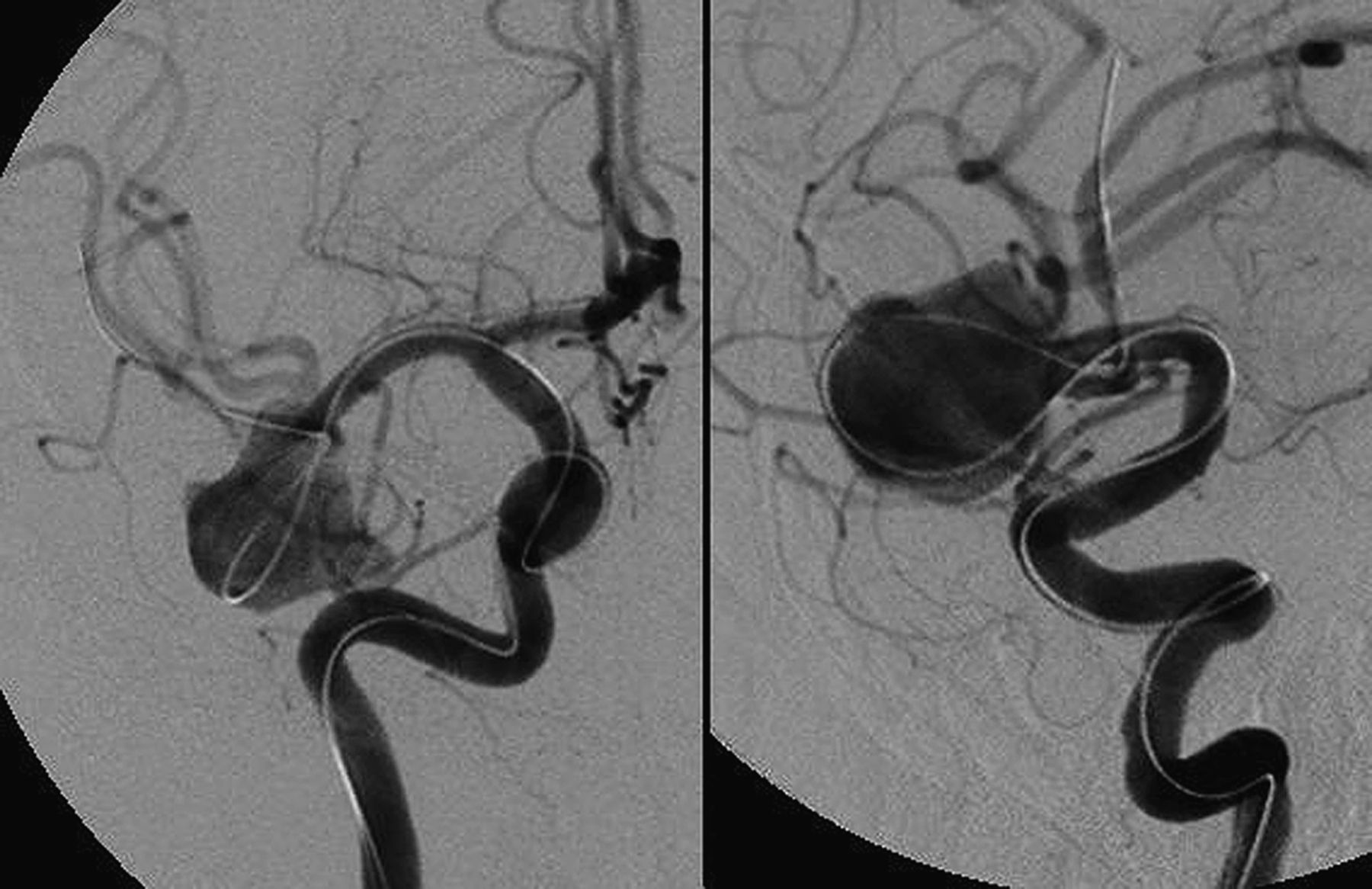
Anteroposterior (left panel) and lateral (right panel) views after M2 catheterization. The microwire and microcatheter were directed into the desired M2 branch by using a looping technique within the dome of the aneurysm.

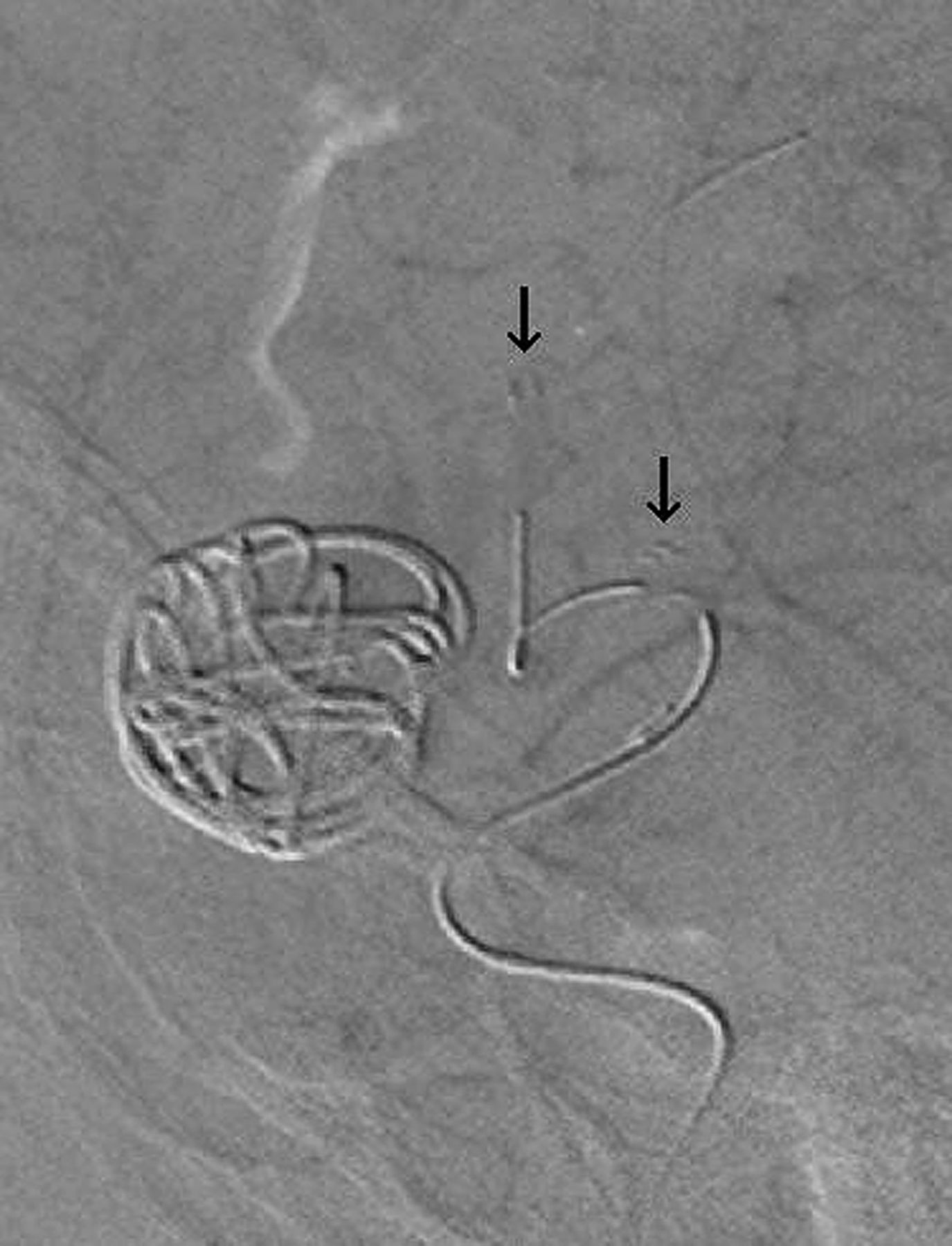
Lateral view demonstrating the position of the stent within the left M1-superior M2 division. The stent tines are marked with arrows.

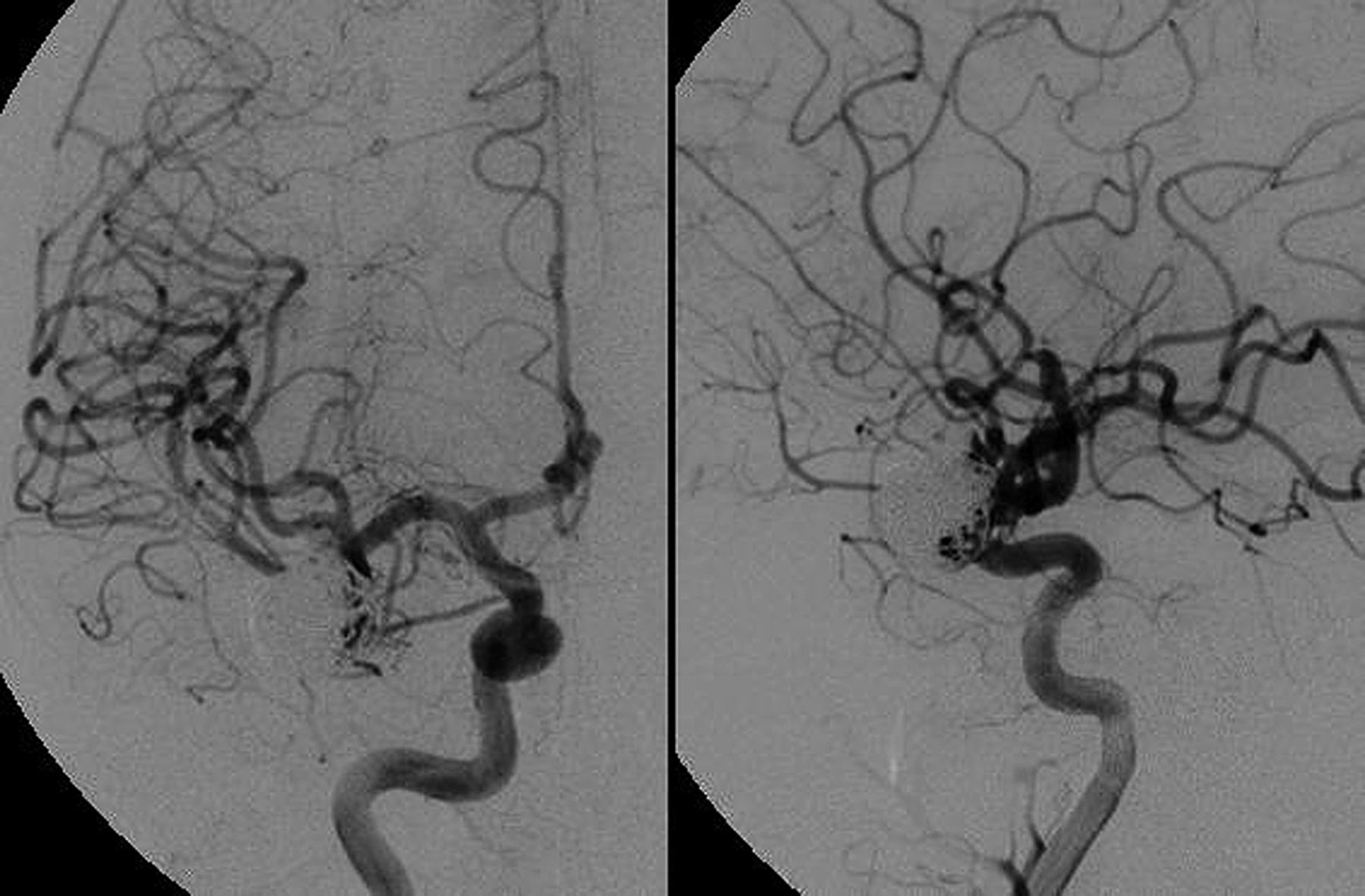
Final anteroposterior (left panel) and lateral (right panel) angiograms at the conclusion of stent-assisted coiling.
Discussion
Recent data suggest that endovascular occlusion rates for large or giant aneurysms are only approximately 60–70%.2 ,3 Frequently, these aneurysms have bulbous domes with wide necks, involve perforating arteries and have complex flow patterns that compete with the manipulation of the wire or catheter by the operator. Furthermore, the large size may encourage coil compaction leading to recanalization. These factors frequently lead to the case being aborted without treatment or, if treatment is initiated, encourage high recurrence rates after endovascular therapies. However, with a growing literature supporting the efficacy and safety of flow diversion stents such as the Pipeline Embolization Device (ev3, Irvine, California, USA),4–6 it is likely that more large aneurysms will be treated by endovascular means in the future. It is important that neurointerventionists have the necessary tools and techniques to successfully navigate and treat these difficult aneurysms.
It can occasionally be exceedingly difficult to navigate a microcatheter through large and giant aneurysms into the desired distal vessel without looping the catheter within the aneurysm dome. Flow jets directed from the parent vessel into the aneurysm may make distal arterial catheterization difficult; often the wire must be looped in the dome before catheterization of the exiting portion of the parent vessel is possible. Once the catheter is looped, it must be straightened so that a stent can be deployed across the neck of the aneurysm. Attempting to straighten the loop by withdrawing the catheter will frequently result in prolapse of the microcatheter tip out of the distal vessel and into the aneurysm dome due to lack of purchase within the distal vasculature. A means of anchoring the catheter in the distal vessel with a balloon, allowing for the catheter loop to be straightened (the balloon anchor technique), has been described previously.1 However, this technique requires that an additional device be used (balloon catheter) and, after anchoring and unraveling of the loop is performed, that the balloon catheter then be exchanged out for the stent. This requires maneuvers that serve as potential opportunities for losing access. Sometimes the microcatheter can be placed distal enough in the vasculature that the microcatheter can be straightened across the aneurysm neck without herniating into the aneurysm; however, this maneuver is effective only some of the time. A third technique which deploys coils into the aneurysm before obtaining distal access with the stent microcatheter (to help direct the microcatheter out of the desired branch without looping) may result in untoward consequences such as loss of important branches from the coil mass or inability to catheterize the distal vessels because of obstructing coil loops. The use of dual catheters (such as an inflated balloon in the aneurysm dome) is technically challenging, uses additional devices and is unlikely to generate the desired outcome. The technique described above, the stent anchor technique (figure 5), uses a partially deployed stent as the means of anchoring the construct so that, when the loop is withdrawn from the aneurysm dome, the distal access is maintained. The stent may then be recaptured, repositioned if needed and then deployed in the desired location. No additional devices or exchanges are necessary for this technique. Given the increasing utility of such stents in the treatment of aneurysms (particularly in large aneurysms), the stent anchor technique is a valuable tool in the armamentarium of the neurointerventionist. We have successfully used the stent anchor technique in one additional case (an 18 mm cavernous aneurysm where obtaining distal access was very difficult) without untoward occurrence. It appears, in our limited experience, that the use of the stent anchor technique is safe and effective for large or giant aneurysms with particularly challenging anatomy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
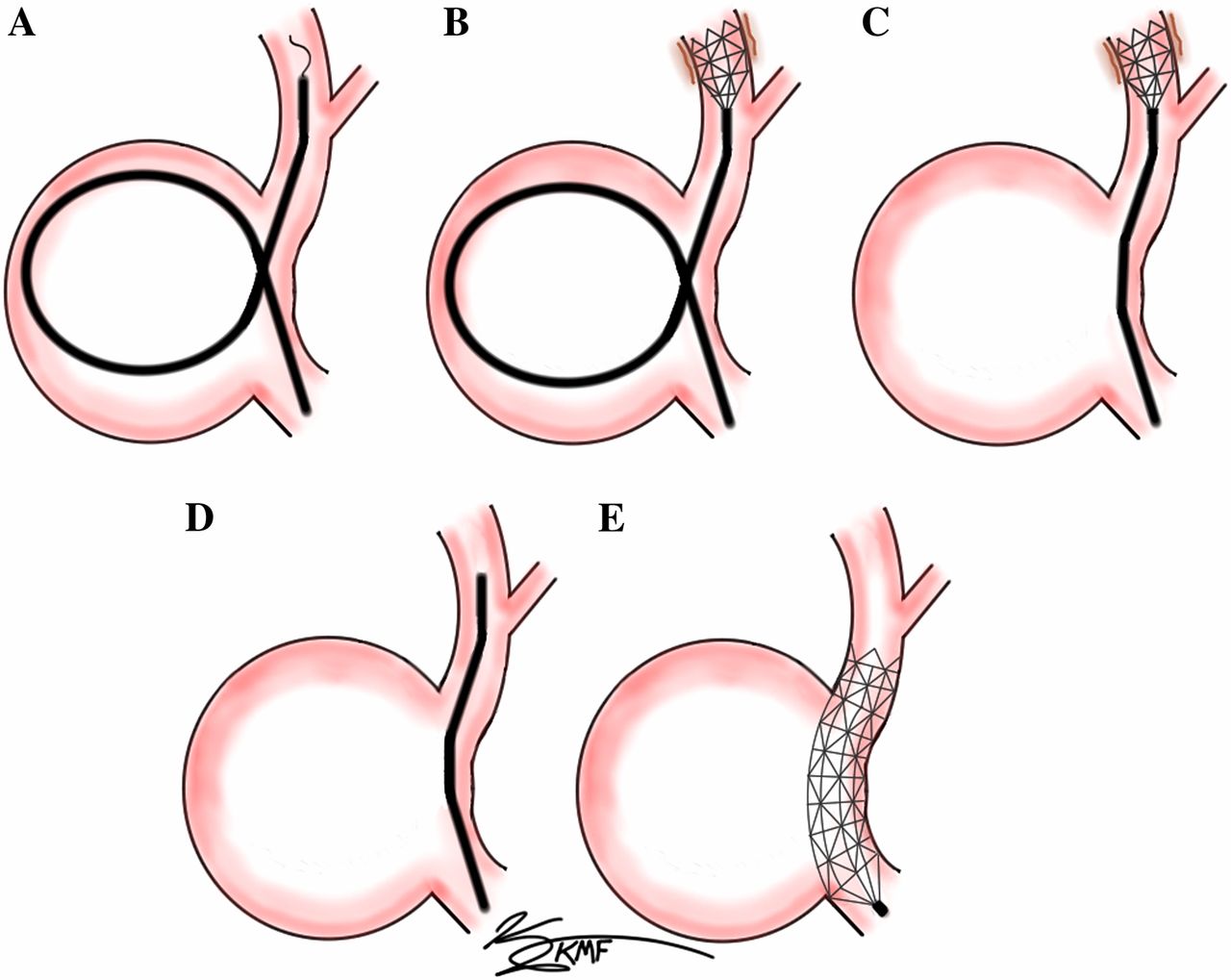
Diagram depicting the stent anchor technique for navigating a large aneurysm. (A) Looping of the microcatheter and wire through a large aneurysm is frequently necessary to successfully navigate the construct into the distal vessel. (B) The microwire is exchanged for a stent and the stent is partially deployed distal to the aneurysm neck, obtaining purchase with the vessel wall. (C) The looping catheter is straightened by pulling back on the catheter and stent. The distal position is maintained because of the purchase of the stent with the vessel wall. (D) Once the loop is straightened, the microcatheter is advanced over the stent and the stent is recaptured. (E) The microcatheter is positioned in an optimal location and the stent is then deployed across the neck of the aneurysm.
Conclusions
Although large and giant aneurysms remain technically difficult to treat via endovascular means, the stent anchor technique provides a method of maintaining distal access when looping of the microcatheter in the dome is necessary. This technique involves partial deployment of a stent distal to the aneurysm to obtain purchase against the vessel wall, such that the catheter can be withdrawn and the excess loop can be straightened. The stent may then be deployed across the neck of the aneurysm. This technique is likely to have increasing utility as the number of large aneurysms being treated with stents increases in the future.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.