Article Text

Abstract
Background Flow control during endovascular stroke treatment with stent-retrievers is crucial for successful revascularization. The standard technique recommended by stent-retriever manufacturers implies obstruction of the respective access catheter by the microcatheter, through which the stent-retriever is delivered. This, in turn, results in reduced aspiration during thrombectomy. In order to maximize aspiration, we fully retract the microcatheter out of the access catheter before thrombectomy—an approach we term the ‘bare wire thrombectomy’ (BWT) technique. We verified the improved throughput with systematic in vitro studies and assessed the clinical effectiveness and safety of this method.
Methods We compared aspiration flow of water through various access catheters (5–8 F) with a Rebar microcatheter (0.18 inch and 0.27 inch) and a Trevo stent-retriever using the standard technique and the BWT technique in vitro. We also retrospectively analyzed 302 retrieval maneuvers in 117 patients who received endovascular treatment with a stent-retriever between February 2010 and April 2015.
Results In the in vitro experiment, removal of the microcatheter in all tested settings resulted in significantly increased aspiration flow through the access catheter (p<0.001). This effect was particularly pronounced in access catheters with a diameter of ≤7 F. In the clinical study, the revascularization rate (Thrombolysis In Cerebral Infarction ≥2b) was 91%. There were no complications associated with the BWT technique in 302 retrieval maneuvers.
Conclusions The BWT technique results in improved aspiration flow rates compared with the standard deployment technique. Our clinical data show that the BWT technique is effective and safe.
- Stroke
- Catheter
- Balloon
- Intervention
- Stent
Statistics from Altmetric.com
Introduction
Recently it has been shown that endovascular treatment is the most effective treatment option for acute ischemic stroke caused by large vessel occlusion (LVO) in the anterior circulation. Five prospective studies have shown that (near) complete recanalization (Thrombolysis In Cerebral Infarction (TICI) ≥2b) of the occluded vessels and a favorable functional outcome (modified Rankin scale (mRS) ≤2) was achievable in up to 88% and 60% of cases, respectively.1–5 Good outcome was mainly attributed to the use of modern stent-retrievers. Even though the basic principle of thrombus removal with stent-retrievers is well established, optimization of retrieval techniques may improve the effectiveness and efficiency of endovascular stroke treatment.6 The standard technique recommended by most stent-retriever manufacturers is to first position a microcatheter and stent-retriever to bridge the thrombus; the stent-retriever is then deployed by retracting the microcatheter until its distal end overlaps the proximal markers of the stent-retriever (figure 1). Subsequently, the thrombus is retrieved by retracting the stent-retriever and the microcatheter into the access catheter, which is a long sheath or a balloon catheter with a diameter of ≥7 F or a distal access catheter with a diameter of 5 F or 6 F in most cases. Antegrade flow should be interrupted during this maneuver in order to prevent migration of thrombus fragments.7 The question whether proximal versus distal aspiration, or whether a balloon catheter versus a large sheath results in superior flow control is subject to various studies and discussed controversially.7–11 In the end, all mentioned techniques have an inherent issue in common when aspiration is to be applied—namely, the microcatheter occludes the access catheter and reduces aspiration flow in the respective access catheter. The degree of flow reduction is determined by the diameters of the catheters used. For example, a standard 0.018 inch (0.46 mm) microcatheter causes considerable occlusion of a 5 F (1.7 mm) distal access catheter, leading to a flow reduction of roughly 65% compared with the empty access catheter. The simplest approach to maximize aspiration flow through the access catheters is to remove the microcatheter before thrombus retrieval (the bare wire thrombectomy (BWT) technique). However, most, if not all, stent-retriever manufacturers discourage from retracting the microcatheter further than the proximal stent-retriever markers in their manuals. To the best of our knowledge, the issue of flow reduction due to the recommended deployment technique has not been addressed yet in the literature. In this paper we present physical considerations and results from an in vitro study in which we examined the impact of the recommended technique versus the BWT technique on aspiration flow. We also present our clinical experience with the BWT technique and report the effectiveness and safety of this method in our institution.

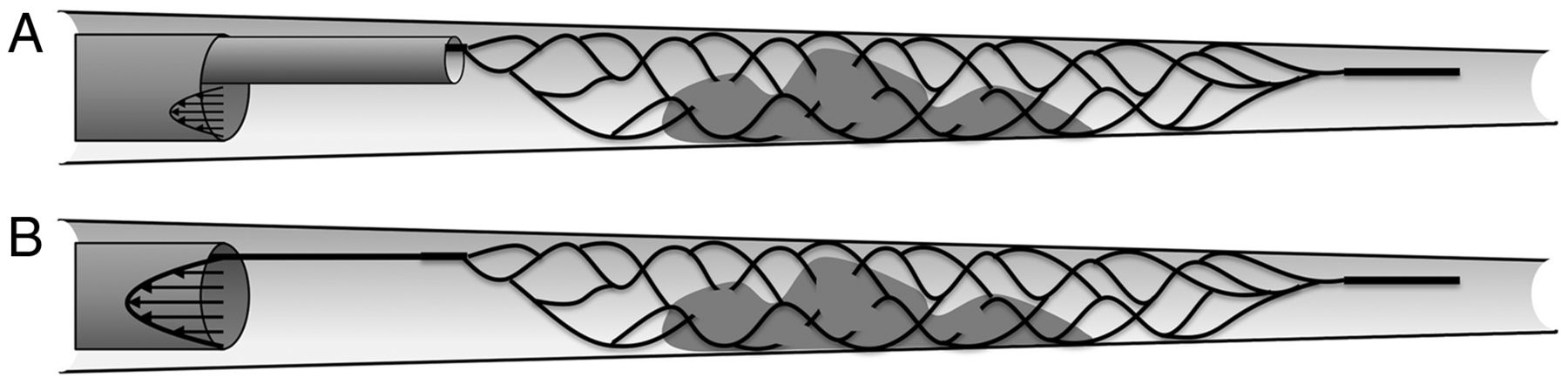
Illustration of the standard (A) and the bare wire thrombectomy (BWT) (B) retrieval technique. A microcatheter and a stent-retriever are positioned to bridge the thrombus. The stent-retriever is then unsheathed by pulling back the microcatheter to the proximal tip of the stent-retriever (A). After the struts of the stent-retriever have interacted with the thrombus, thrombus removal is achieved by retraction of the microcatheter and the stent-retriever. During this maneuver, antegrade blood flow should be interrupted in order to prevent thrombus migration. The microcatheter can be fully retracted before thrombus removal (BWT) in order to increase aspiration flow (B).
Methods
Calculations
For laminar flow conditions, the average flow  in a straight circular tube can be calculated with the Hagen–Poisseuille equation
in a straight circular tube can be calculated with the Hagen–Poisseuille equation  , if the radius (R) and the length (l) of the tube, the pressure difference (ΔP) in the tubing system, and the viscosity (η) of the fluid are known.12 For a concentric annular tube, the formula must be modified to take into account the additional cylinder in the inside of the channel, leading to:
, if the radius (R) and the length (l) of the tube, the pressure difference (ΔP) in the tubing system, and the viscosity (η) of the fluid are known.12 For a concentric annular tube, the formula must be modified to take into account the additional cylinder in the inside of the channel, leading to: with Re being the (inner) radius of the access catheter and Ri being the (outer) radius of the microcatheter/pusher-wire (figure 2).12 The average flow in the annular tube is significantly smaller than a circular tube with the same outer radius, which is due to two effects (see figure 2): (1) the inner tube is sealed off, which blocks some of the volume accessible to the liquid; and (2) the liquid is experiencing higher drag forces in the annular tube since the contact surface is increased. The position of the microcatheter/pusher-wire within the access catheter has a very important impact on flow, as schematically shown in figures 2B and C. Here, the flow is minimized for a concentric alignment and increases as the inner tube moves outward.12 As the position of the microcatheter/pusher-wire is unlikely to be concentric throughout in a realistic setting, we posit that the actual flow lies in a range between the maximal and minimal possible flow (figure 2). This effect can be included in our model through an additional friction term, which depends on the size ratio Re/Ri and the eccentricity of the specific tube set-up.12 In our modeling we have excluded secondary effects arising from the rigidity, curvature, and the surface properties of the catheters/pusher-wires.12
with Re being the (inner) radius of the access catheter and Ri being the (outer) radius of the microcatheter/pusher-wire (figure 2).12 The average flow in the annular tube is significantly smaller than a circular tube with the same outer radius, which is due to two effects (see figure 2): (1) the inner tube is sealed off, which blocks some of the volume accessible to the liquid; and (2) the liquid is experiencing higher drag forces in the annular tube since the contact surface is increased. The position of the microcatheter/pusher-wire within the access catheter has a very important impact on flow, as schematically shown in figures 2B and C. Here, the flow is minimized for a concentric alignment and increases as the inner tube moves outward.12 As the position of the microcatheter/pusher-wire is unlikely to be concentric throughout in a realistic setting, we posit that the actual flow lies in a range between the maximal and minimal possible flow (figure 2). This effect can be included in our model through an additional friction term, which depends on the size ratio Re/Ri and the eccentricity of the specific tube set-up.12 In our modeling we have excluded secondary effects arising from the rigidity, curvature, and the surface properties of the catheters/pusher-wires.12

Impact of tube position on flow. There is laminar flow in the investigated settings (A). Insertion of an inner tube causes flow reduction (B and C). Flow reduction is minimal if the inner tube is excentric (B) and maximal if the inner tube is concentric (C).
In vitro model
We compared aspiration flow through various access catheters with and without a microcatheter/pusher-wire in their lumen. A Penumbra aspiration pump (Penumbra, Alameda, California, USA) that provides constant negative/suction pressure was connected to the respective aspiration catheter via the standard tubing and a standard Y-adapter (Gateway PLUS; Boston Scientific, Marlborough, Massachusetts, USA) (inner diameter 3 mm). Microcatheters and pusher-wires were introduced via the Y-adapter. In order to assess aspiration flow we aspirated water with a constant negative pressure of 25.5 in Hg (the manufacturer's recommended pressure) for 120 s and assessed the weight of the aspirated fluid in grams. The water was kept at a constant temperature of 20°C in order to ensure a constant viscosity of 0.001 Pa s and a density of 0.9982 g/mL. The results of 10 measurements were averaged and converted to a volumetric dimension (mL). The aspiration flow (mL/s) was obtained by dividing the collected volume by time. The resistance of the aspiration tubing and the valve were experimentally determined (12.562×106 Pa s/m3) and accounted for in our calculations.
In our experiments we used the following access catheters: Cook Flexor 8 F sheath (diameter 2.87 mm; length 0.9 m) (Cook Medical, Bloomington, Indiana, USA), FlowGate 8 F balloon catheter (diameter 2.1 mm; length 0.9 m) (Concentric Medical, Mountain View, California, USA), Guider Softip 6 F and 8 F guiding catheter (diameter 2.2 mm and 1.6 mm; length 1.0 m) (Boston Scientific), Envoy MPD guiding catheter with an angled tip 6 F and 7 F (diameter 1.9 mm and 2.0 mm; length 1.0 m) (Cordis, Miami Lakes, Florida, USA), Navien distal aspiration catheter 5 F (diameter 1.5 mm; length 1.25 m) (Covidien, Irvine, California, USA), and Sofia distal aspiration catheter 5 F (diameter 1.4 mm; length 1.25 m) (Microvention, Tustin, California, USA). As a microcatheter we used the Rebar 0.18 inch microcatheter (tapered with a distal and proximal diameter of 2.3 F and 2.8 F, respectively) and 0.27 inch microcatheter (2.8 F diameter) (Covidien, Mansfield, Massachusetts, USA). As most pusher wires of stent-retrievers have comparable diameters, we only used one stent-retriever: Trevo proVue (diameter 0.46 mm) (Stryker, Kalamazoo, Michigan, USA). Nominal metric specifications of catheter/wires were adopted as indicated by the manufacturers and not rounded when they needed to be converted to the metric system. For simplification of calculations the diameter of tapered catheters was calculated as the average between the wider proximal and the thinner distal end.
Clinical study
In our prospectively maintained stroke registry we identified 309 patients who received endovascular treatment for LVO stroke between 1 February 2010 and 15 April 2015. Two hundred and seventy-three (88%) of these patients received endovascular treatment with stent-retrievers. One hundred and seventeen of the latter met the inclusion criteria of endovascular treatment with the BWT technique and were included in our retrospective analysis.
Radiological and procedural data for this study comprised site of LVO, type of intra-arterial treatment (including systemic thrombolysis and devices), number of stent-retriever passes, result of recanalization (TICI), and peri- and post-treatment complications.13 Clinical assessment comprised clinical presentation (National Institutes of Health Stroke Scale, NIHSS) at admission and disability (modified Rankin Scale, mRS) at follow-up (day 90).14 ,15 Hemorrhagic events were defined according to the European Cooperative Acute Stroke Study (ECASS) classification.16 Radiological data were assessed by the treating neuroradiologist and re-evaluated by a colleague who was blinded to all clinical data. If there was disagreement between the observers, a reference standard was established for statistical analyses in a consensus reading. Primary endpoints were defined as successful vessel revascularization (TICI ≥2b) and all complications associated with the BWT technique.
Statistical analysis
Data are expressed as mean±SD unless indicated otherwise. Mann–Whitney U tests were used for comparing aspiration flow after testing our data for normal distribution with a Shapiro–Wilk test. p Values of an α level ≤0.05 were defined as significant. All statistical analyses were performed with SPSS V.23 software (IBM, Armonk, New York, USA).
Results
In vitro model
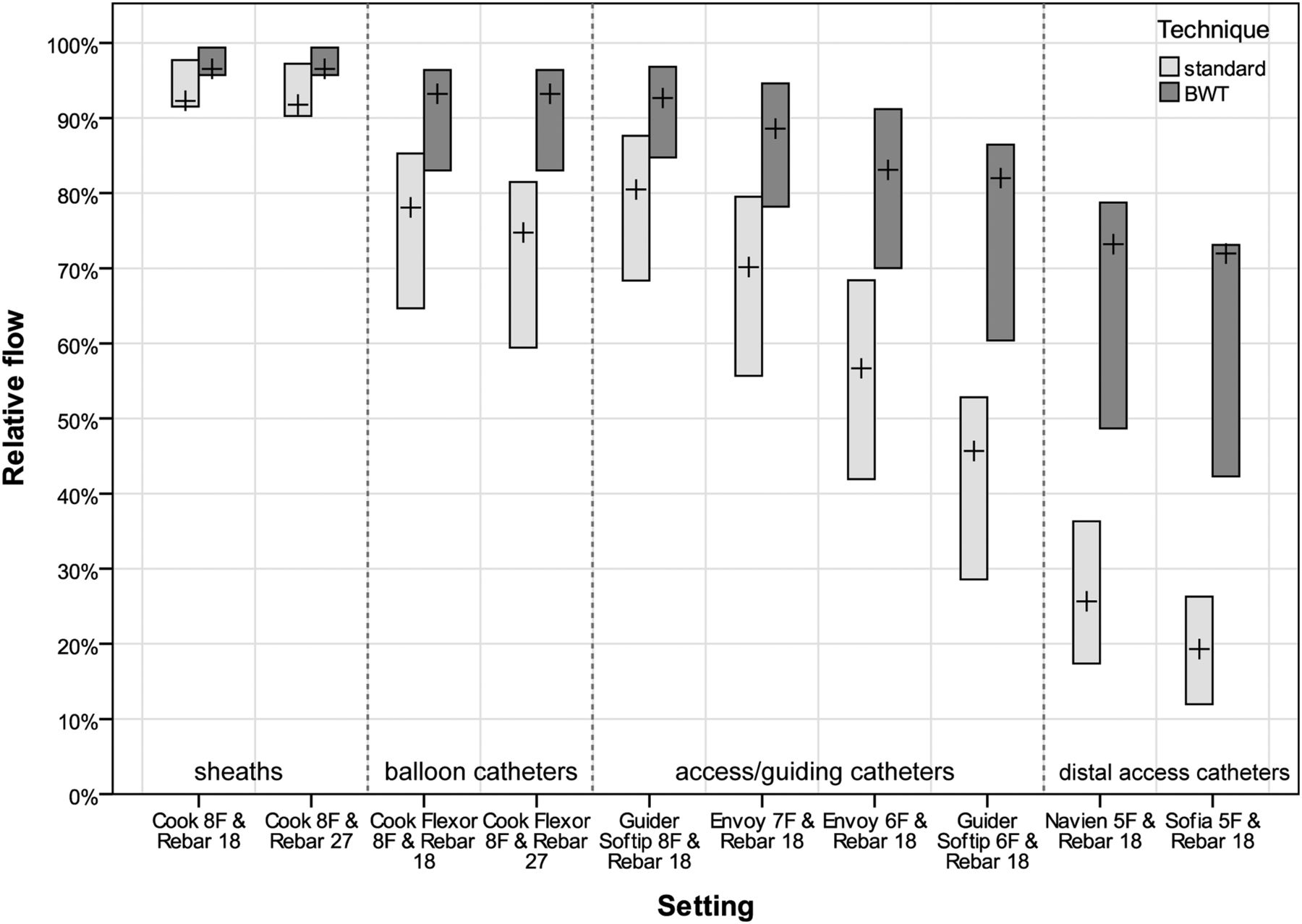
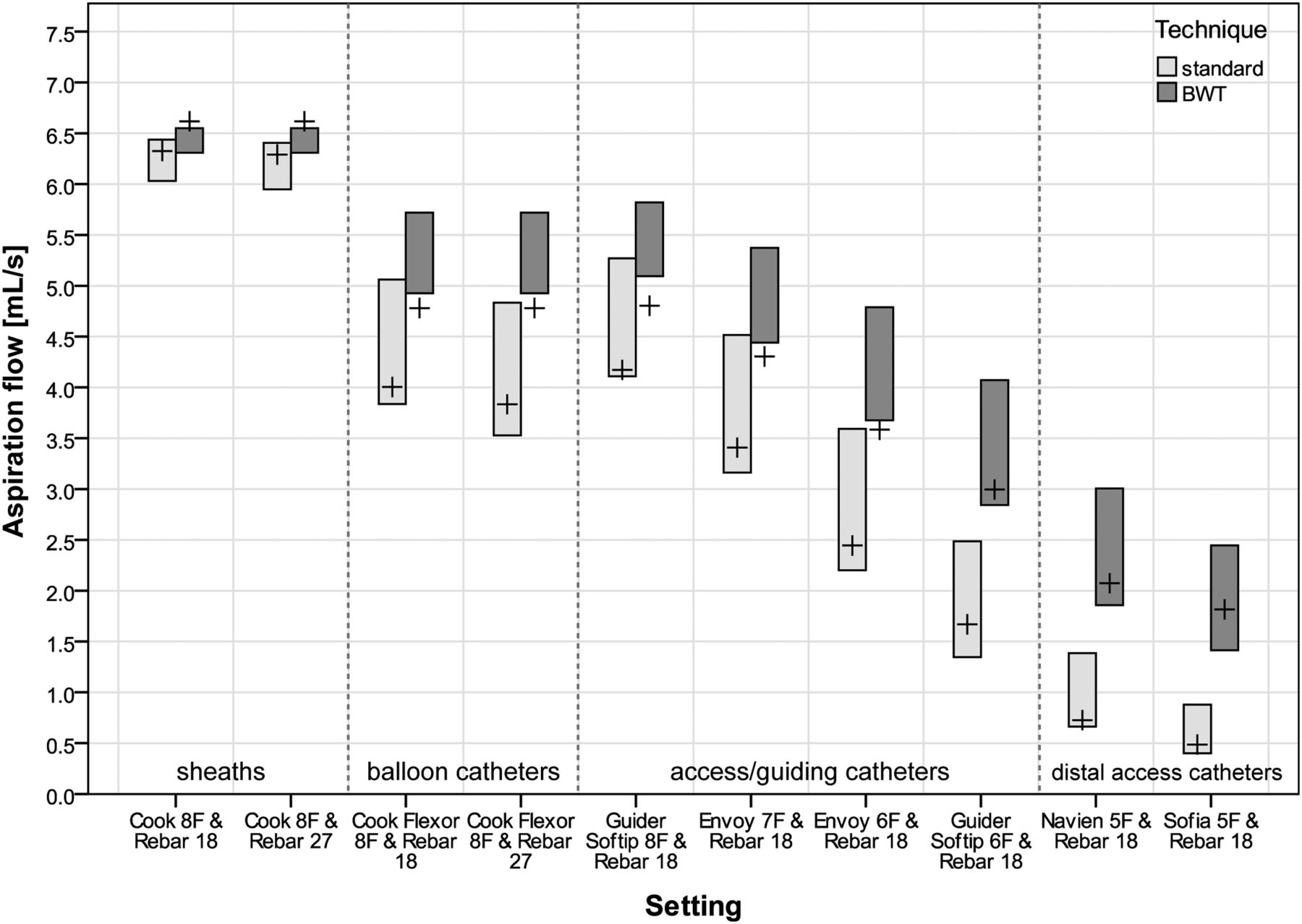
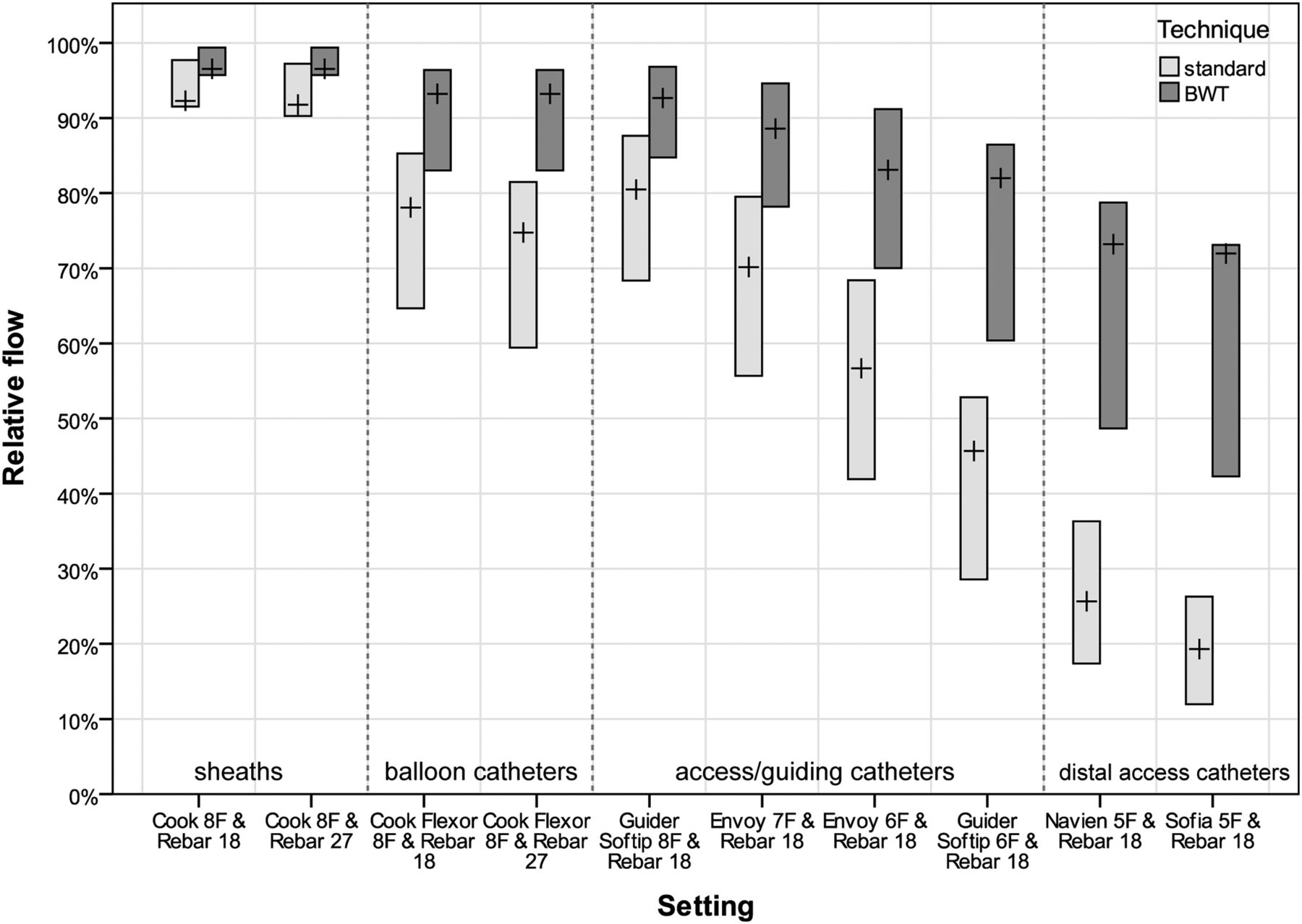
Table 1 and figures 3 and 4 summarize the results of our experiments. Removal of the microcatheter in all tested settings resulted in significantly increased aspiration flow through the access catheter (p<0.001). Figure 3 illustrates absolute results of our experiments and figure 4 illustrates the relative flow reduction with respect to an empty access catheter. This representation allows for visualizing our data independent of aspiration pressure, viscosity of the fluid, and length of the tubes. The Penumbra aspiration tubing and the Y-connector that connect the access catheters to the pump restricted flow rates significantly (p<0.001). Examples of theoretical flows through a catheter versus a catheter plus the Penumbra aspiration tubing were 6.51 mL/s vs 3.34 mL/s in a Sofia 5 F catheter (length 1.25 m) and 159.77 mL/s vs 6.59 mL/s in a Flexor 8 F sheath (length 0.9 m).
Aspiration flow of water through various access catheters depending on whether the microcatheter was kept in the access catheter (regular technique) or not (BWT technique)

Aspiration flow of water through various access catheters depending on whether the microcatheter was kept in the access catheter (regular technique) or not (bare wire thrombectomy technique). Bars represent the calculated range of flow, depending on position of the inner tube; crosses represent the measured flow. Water with a temperature of 20°C was aspirated with a constant negative pressure of 25.5 in Hg. Values for blood are approximately 3–4 times lower due to its higher viscosity.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative aspiration flow through various access catheters depending on whether the microcatheter was kept in the access catheter (regular technique) or not (bare wire thrombectomy technique). Relative values are independent of aspiration pressure, viscosity of the aspirated fluid, and length of the tubes. 100% represents flow through an empty access catheter. Bars represent the calculated range of flow, depending on the position of the inner tube; crosses represent the experimentally measured flow.
Clinical experience
Sixty of the 117 patients (51%) were women. Mean age was 70.6±14.6 years (median 75.0; range 11.3–105.1 years). Mean NIHSS at admission was 17.8±6.8 (median 18; range 3–33). Target occlusion sites were the carotid T in 21 cases (18%) and the proximal internal carotid artery (ICA) in 14 (12%); 9 (7%) of the latter were dissections of the ICA. There were eight cases (7%) with occlusion of the proximal ICA and the middle cerebral artery (MCA). One (1%) of the latter also had anterior cerebral artery (ACA) occlusion. In addition, there were four cases (3%) with occlusion of both the MCA and the ACA. The MCA and ACA alone were occluded in 59 cases (50%) and 1 case (1%), respectively. Occlusion sites of the MCA were the M1 segment in 50 cases, the bifurcation in 5 cases, the M2 segment in 14 cases, and the M3 segment in 2 cases.
Seventy-eight patients (67%) received systemic thrombolysis. Twenty-three patients (20%) received additional intra-arterial thrombolysis. Sixteen of the latter also received systemic thrombolysis. A total of 302 retrieval maneuvers were performed using the BWT technique. Fifty-two (17.0%) retrieval maneuvers were made with a Solitaire device and 173 (56.4%) retrieval maneuvers were made with a Trevo device. The remaining 77 retrieval maneuvers were made with the following devices: Separator 3D (28 maneuvers) (Penumbra), MindFrame Capture (19 maneuvers) (MindFrame, Irvine, California, USA), pREset (16 maneuvers) (Phenox, Bochum, Germany), ReVive (8 maneuvers) (Codman Neurovascular, Raynham, Massachusetts, USA), Aperio (6 maneuvers) (Arcandis, Pforzheim, Germany). Distal access catheters (≤6 F) were used in 60 cases (51.3%). Complete or near complete revascularization (TICI ≥2b) was achieved in 106/117 patients (91%). The rate of patients achieving good functional outcome (mRS ≤2) was 32% (29/92 patients for whom follow-up was available). There were five cases (4%) of small asymptomatic parenchymal hemorrhage (PH1) and eight cases (7%) of larger parenchymal hemorrhage (PH2). Three (3%) of the latter were symptomatic. There were four cases (3%) of vessel perforation by the pusher-wire and/or microcatheter with consecutive subarachnoid hemorrhage (SAH) that was accompanied by small parenchymal hemorrhage (PH1) in one case and large parenchymal hemorrhage (PH2) in another case. Retrieval with a Mindframe device in an M3 branch caused SAH with adjacent PH1 in one case. There were no complications associated with the BWT technique. In particular, there were no cases of kinking or detachment of the respective stent-retriever.
Discussion
Endovascular thrombus removal with stent-retrievers has emerged as a common treatment option for LVO stroke.1–5 Flow control during endovascular stroke treatment is one of the crucial factors for successful revascularization.7 Even though it is unknown which precise flows are necessary for full flow control, Chueh et al7 ,8 have shown in an experiment that antegrade flow should be reduced to a minimum in order to prevent (micro)thrombus migration during thrombus retrieval.9–11 It was found that balloon catheters restrict antegrade flow best by occluding the respective artery.7 Nevertheless, the issue of impaired aspiration flow remains, because the retrieval technique recommended by the stent-retriever manufacturers implies partial occlusion of the respective access catheters, which in turn impairs aspiration flow. Our study shows that there is always significantly more aspiration flow if the pusher-wire of the stent-retriever instead of the microcatheter is kept in the access catheter (figures 3 and 4). The smaller the access catheters, the more important is this effect. For instance, keeping the microcatheter in an 8 F compared to a 7 F access catheter/sheath resulted in a flow reduction of 5% and 20%, respectively. In absolute terms, aspiration flows dropped from 6.6 to 6.3 mL/s (8 F) and from 4.3 to 3.4 mL/s (7 F). One must consider that the viscosity of blood is 3–4 times higher than water (0.003–0.004 Pa s), so flow rates of blood are 3–4 times lower than our results for water (table 1 and figure 3). When the viscosity of blood is accounted for, expected flow rates are almost negligibly small if distal access catheters (≤6 F) are occluded by a microcatheter (table 1 and figure 3). In fact, a 0.018 inch microcatheter that remains in a 5 F or 6 F access catheter occludes it to such a degree that almost no aspiration blood flow can be achieved with the recommended setting of the Penumbra pump (table 1 and figures 3 and 4).17 In other words, pressure must be 3–4 times greater to achieve the same flow as with the BWT when a microcatheter is kept in a 5 F access catheter (table 1). On the other hand, this means that flow must be tripled or quadrupled in order to achieve the same suction. These findings might be taken for granted at first sight, however, they have important implications: given that the normal blood flow in the MCA is approximately 2.0±0.5 mL/s, our results imply that the advantage of distal aspiration is practically annulled when a stent-retriever is combined with a distal aspiration catheter (≤6 F) and the microcatheter is kept in place as recommended.18 This is why we completely retract the microcatheter when (additional) aspiration (with a distal access catheter) is necessary. Even though our personal communication with other interventional neuroradiologists implies that this technique is not uncommon, it is noteworthy that some manufacturers discourage fully retracting the microcatheter. Stryker, the manufacturer of the Trevo devices, for example, explicitly warns of kinking and detachment of its retrievers when the microcatheter is removed. Hence, the most important question in daily clinical practice is whether the BWT technique produces improved revascularization rates without increasing complication rates. However, only a large randomized and prospective study will enable us to determine whether the BWT technique is superior to the recommended standard technique. As our data do not allow such an analysis, our study is restricted to the discussion of the effectiveness and safety of our method. In fact, our revascularization (TICI ≥2b) rate of 91% is comparable to (and slightly higher than) the results provided by recent large randomized studies that reported revascularization rates of 56–88%.1–5 However, given the retrospective and non-randomized nature of our study, our data do not allow us to ascribe our recanalization rate solely to the BWT technique. Nonetheless, it is noteworthy that we achieved high revascularization rates despite the inclusion of occlusions of the proximal ICA and occlusions of the posterior circulation (both of which were not included in the aforementioned prospective studies).
The more important parameter for our BWT technique may be the complication rate. Given that there were no complications associated with the BWT technique in 302 retrieval maneuvers, this technique can also be regarded as safe. Again, our results must be interpreted with caution due to the retrospective nature of our analysis. Also, our comparison with the literature might be biased, as it is likely that other neuroradiologists have used the BWT technique without reporting it. In the end, even though we cannot advise the use of a device against the manufacturers’ recommendations, our data imply that the BWT technique is a safe technique that allows significantly more flow control than the recommended standard technique.
Study limitations
A limitation of our study is the lack of in vivo experiments and the limited design of our in vitro experiment. We decided not to conduct animal experiments as aspiration of the necessary amounts of blood would be lethal. We also decided not to conduct in vitro experiments with blood as data in the literature suggest that the viscosity of blood is altered contingently by the necessary anticoagulants.19 ,20 As an experiment that involves all possible combinations of stent-retrievers, microcatheters, sheaths, and access catheters is almost impossible to conduct, we decided to focus on the most common settings in a simple but valid in vitro experiment. To keep our experiment as simple as possible, we conducted our experiments with water instead of simulating the viscosity of blood with a mixture of glycerol and water. We modeled the experimental set-up as a completely straight and rigid annular tube, with no-slip boundary conditions at the surfaces. Although this model might seem oversimplified at first glance, it perfectly captures the essential physics of the problem, as reflected by the excellent agreement between our experimental findings and the theoretical predictions.12 ,21 ,22 A further limitation is the retrospective analysis of our clinical data and the small sample size. Even though we could show that the BWT technique is effective and safe, future prospective randomized studies are needed to determine whether improved flow control also results in improved clinical outcome rates.
Conclusions
Our in vitro experiments show that the BWT technique results in significantly improved aspiration flow rates compared with the standard deployment technique. This effect is particularly pronounced when the access catheter has a diameter of ≤7 F. Our clinical experience shows that the BWT technique is effective and safe. The aim of future studies should be to evaluate whether increased aspiration also results in improved procedural and clinical outcome.
References
Footnotes
ON and JPA contributed equally.
Contributors Conception and design: all authors. Acquisition of data: all authors. Analysis and interpretation of data: all authors. Drafting the article: all authors. Critically revising the article: all authors.
Competing interests M-AB has received non-financial support from Covidien, Stryker, and Terumo/Microvention. MW has received grants from Stryker Neurovascular and Siemens Healthcare; grants from Stryker Neurovascular, Silkroad Medical, Siemens Healthcare, and Bracco; and non-financial support from Codman Neurovascular, Covidien, Abbott, St Jude Medical, Phenox, Penumbra, Microvention/Terumo, B. Braun, Bayer, Acandis, and ab medica.
Ethics approval Ethics approval was obtained from the local ethics committee of RWTH Aachen University.
Provenance and peer review Not commissioned; externally peer reviewed.