Article Text

Abstract
Background Stenting of the intracranial venous sinuses is used as a treatment in certain cases of idiopathic intracranial hypertension (IIH). Interest in, and experience of, this technique is growing, particularly in recent years. We sought to provide an updated systematic review and meta-analysis of the use of venous stenting in these patients, examining clinical outcomes.
Methods A literature search of venous stenting in IIH patients was performed. Using random-effects meta-analysis, we evaluated the following outcomes: clinical resolution of papilledema; headaches and pulsatile tinnitus; recurrence of symptoms after stenting; and complications.
Results Twenty articles from 18 different centers were included. In a total of 474 patients. 418 were female (88%). The mean age of the patients was 35, while the mean body mass index (BMI) was 35 kg/m2. Median follow-up was 18 months. The overall rate of improvement in papilloedema was 93.7% (95% CI 90.5% to 96.9%), while the overall rate of improvement or resolution of headache was 79.6% (95% CI 73.3% to 85.9%). Pulsatile tinnitus resolved in 90.3% (95% CI 83.8% to 96.70%), while the overall rate of recurrence of IIH symptoms after stenting was 9.8% (95% CI 6.7% to 13%). The rate of major complications was 1.9% (95% CI 0.07% to 3.1%).
Conclusions Venous sinus stenting in patients with IIH who are refractory to medical therapy appears to have an excellent safety profile and is associated with significant improvements in headaches, pulsatile tinnitus, and papilledema.
- idiopathic intracranial hypertension
- stent
- vein
- papilledema
- headache
Statistics from Altmetric.com
Introduction
Idiopathic intracranial hypertension (IIH) preferentially affects overweight females of childbearing age and may lead to significant visual disability and blindness.1 While multiple factors have been suggested to play a role in the development of IIH, recent interest has focused on stenoses of the intracranial transverse venous sinuses (TS).2 Stenting of the venous sinuses has emerged as a potentially promising treatment in carefully selected patients. However, the management of patients with medically refractory IIH remains controversial and the role of TS stenting when compared with more established techniques such as CSF diversion or optic nerve sheath fenestration is still unclear. We sought to provide an update on the status of endovascular management of IIH based on a systematic review and meta-analysis focusing on clinical outcomes in IIH patients who underwent venous stenting. Other groups have previously performed meta-analyses of patient outcomes following this technique. This begs the question whether it is worth repeating, and this has been raised in the literature before.3 Therefore, we sought to provide an update on the status of endovascular management of IIH based on a systematic review and meta-analysis focusing on clinical outcomes in patients who underwent venous stenting. We feel that it is worth updating the literature at this stage. The most recent meta-analysis on this topic (totaling 136 patients) was completed in December 2014,4 and studies published since then (including more than 270 patients) reflect more than 50% of our patient cohort.
Methods
Literature search strategy and selection criteria
For this systematic review and meta-analysis, a comprehensive literature search was performed by an experienced reference librarian of Ovid MEDLINE, Ovid EMBASE, and the Web of Science from their inception to January 31 2018 for any studies published in any language on the use of stenting for idiopathic intracranial hypertension. Key words included pseudotumor cerebri, idiopathic intracranial hypertension, stent, endovascular, lateral sinus, and transverse sinus in various and/or combinations. In addition, we searched ClinicalTrials.gov, meeting proceedings, and performed a reverse bibliography search from previously published systematic reviews and/or meta-analyses. Inclusion criteria were the following: studies reporting outcomes for patients classified as having IIH who underwent venous stenting; and a minimum of five consecutive patients. Studies were excluded if subsequent papers had looked at outcomes from the same patient group (ie, overlapping patient populations), if they had less than five patients, or if they did not report a consecutive case series. The study adhered to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA; http://prisma-statement.org/).
Data extraction and outcomes
Each study was analyzed by two independent reviewers to extrapolate the following data: patient demographics (gender, age, BMI, CSF opening pressure, mean trans-stenotic pressure gradients); presenting symptoms (headache, pulsatile tinnitus, papilledema); clinical outcomes were assessed as improvement or resolution of symptoms for headache and for pulsatile tinnitus (headache and pulsatile tinnitus were patient-reported outcomes and for visual field symptoms, improvement or resolution of papilledema accounted by formal visual examination was recorded; and clinical complications, a meta-analysis of which was also performed.
Risk of bias assessment
A modified Newcastle–Ottawa Scale for Cohort Studies was used to estimate risk of bias from the included studies. This is a validated tool which is recommended by the Cochrane Collaboration for the assessment of the quality of non-randomized studies included in systematic reviews and/or meta-analyses. Each study is judged on eight items which are grouped into three categories: selection of study groups, according to whether standard clinical criteria for the diagnosis of IIH was used; comparability of study groups in terms of clinical status, angiographic, and venous manometric features; and assessment of the outcomes of interest. Factors that result in a low-risk of bias using this scale include: well-defined selection criteria; well-defined intervention or treatment without the concomitant use of other interventions (eg, CSF drainage) which may potentially confound study outcomes; and rates of long-term follow-up for >90% of patients.
Statistical analysis
From each study, we estimated the cumulative incidence (event-rate) as well as the 95% CIfor each outcome. Event-rates were pooled across studies with a random-effects model meta-analysis.5 Heterogeneity across studies was assessed using the I2 statistic.6 Analysis was conducted with Open Meta-Analyst software7 and JMPversion 13.2. SAS Institute Inc. (Cary, NC, 1989– 2007). For assessment of predictors of outcomes and complications, an individual patient meta-analysis was performed and analyzed by means of a student’s t-test in order to compare clinical variables between the groups.
Results
Literature search, study characteristics, risk of bias
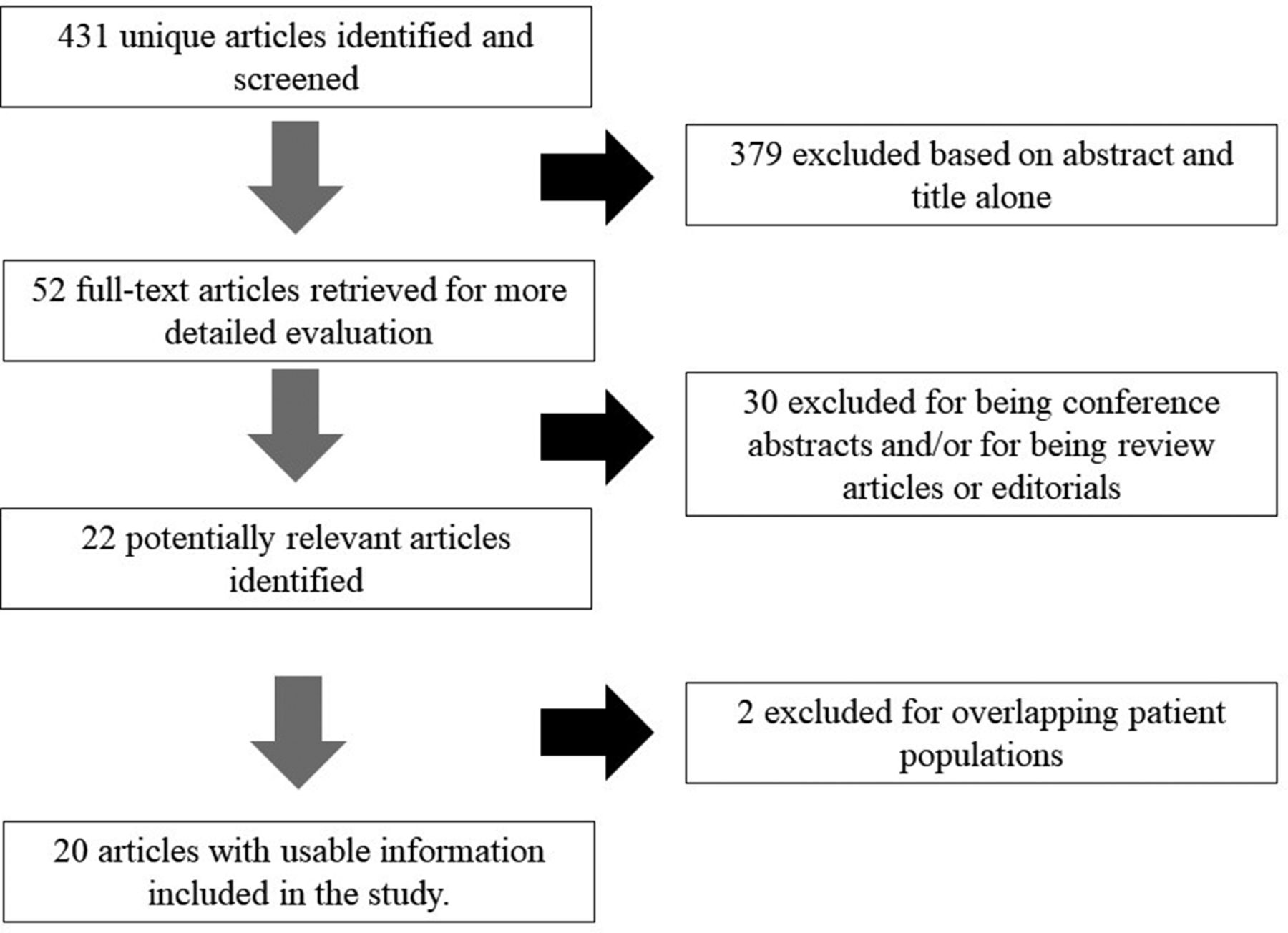
The initial literature search resulted in 431 articles, which were all screened based on title and abstract. Fifty-two full-text articles were subsequently retrieved for more detailed evaluation, after 379 were excluded. Of these 52, 30 were excluded for being either review articles, not specifically looking at outcomes of venous stenting for IIH or being conference abstracts only with insufficient information to include. Of the remaining 22 articles, two were excluded for overlapping patient populations. This resulted in 20 articles from 18 groups (as defined by the affiliation of the senior author) looking at a total of 474 patients. The smallest studies had six patients, while the largest had 52. Fourteen studies were retrospective studies while six were prospective observational studies. All patients had a clinical diagnosis of IIH, although it was not clear in all papers if this diagnosis was made according to the modified Dandy criteria. Most of the included studies had a moderate risk of bias using the modified Newcastle–Ottawa scale (table 1).
Patient characteristics
Baseline characteristics and patient presentation
Patient characteristics are summarized in table 1. Of the 474 patients included, 419 were female (88%). Of the 18 studies (429 patients) in which it was documented, 342 of the patients underwent venous sinus stenting as a primary treatment (78%). The mean age of the patients was 35 (range: 5–67), while the mean body mass index (BMI) was 35 kg/m2 (range: 15–73). Mean CSF opening pressure, recorded in 285/474 patients (60.1%), was 37 cmH2O (range: 14–73). Nineteen of the studies measured the pressure gradient across the venous stenoses, and the mean value was 21 mm Hg (range: 0–56). Median follow-up duration for all studies was 18 months (range:<1 month to 198 months). Total patient-year follow-up was 664.5 years
Clinical outcomes
Papilledema
Eighteen of the studies reported improvement in papilledema, for a total of 370 patients (see table 2, summarizing overall outcomes). The overall rate of improvement in papilledema was 93.7% (95% CI 90.5% to 96.9%), with 336 of the reported 370 patients showing an improvement. The I2 was 52.35%, indicating significant heterogeneity between studies. Outcomes for papilledema and/or visual symptoms are summarized in a forest plot in figure 1.
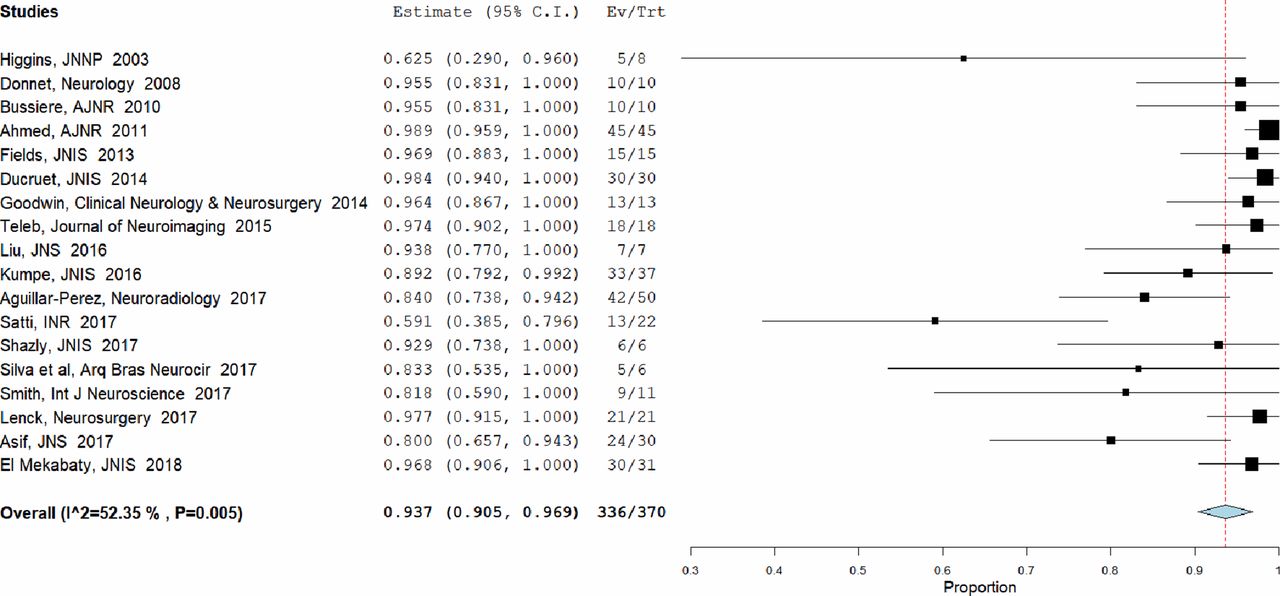
Forest plot – papilledema outcomes.
Outcome data
Headache
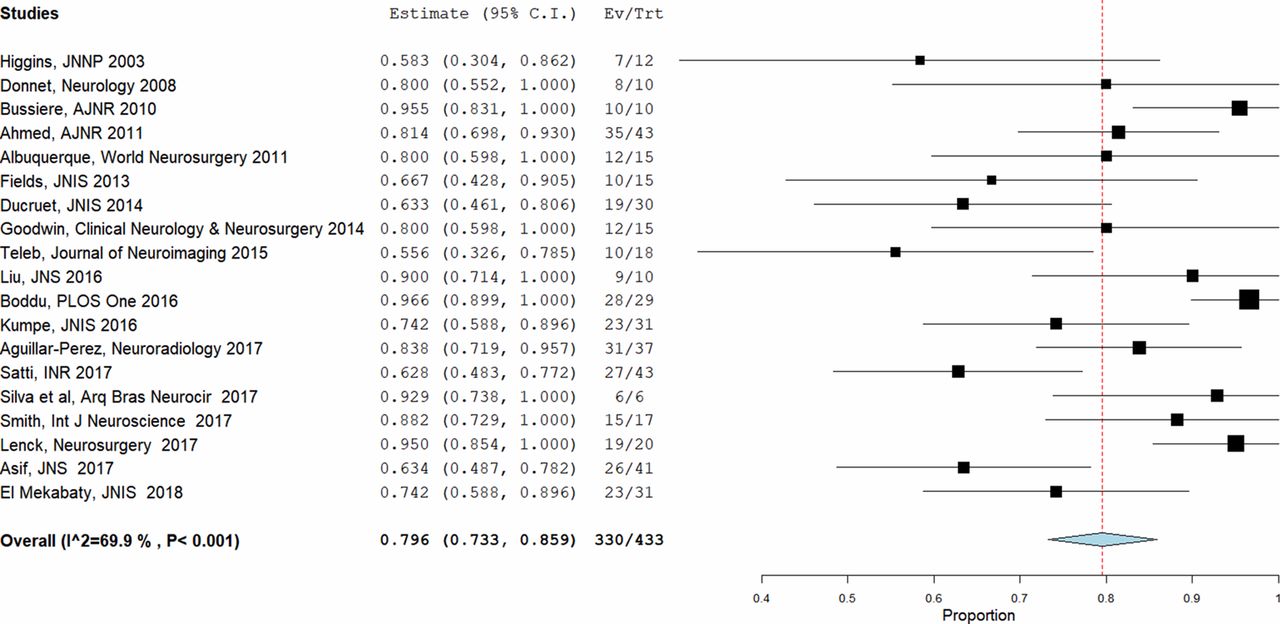
Nineteen of the studies reported improvement in headache, including a total of 433 patients. None used a quantifiable pain or headache scale, and a ‘significant improvement’ or ‘resolution’ of headache was recorded where relevant. Overall, reported headache improvement was present in 330 of 433 patients or 79.6% (95% CI 73.3% to 85.9%). There was significant heterogeneity between the studies which looked at headache, with an I2 value of 69.9%. A forest plot is presented in figure 2, which summarizes outcomes for headache.
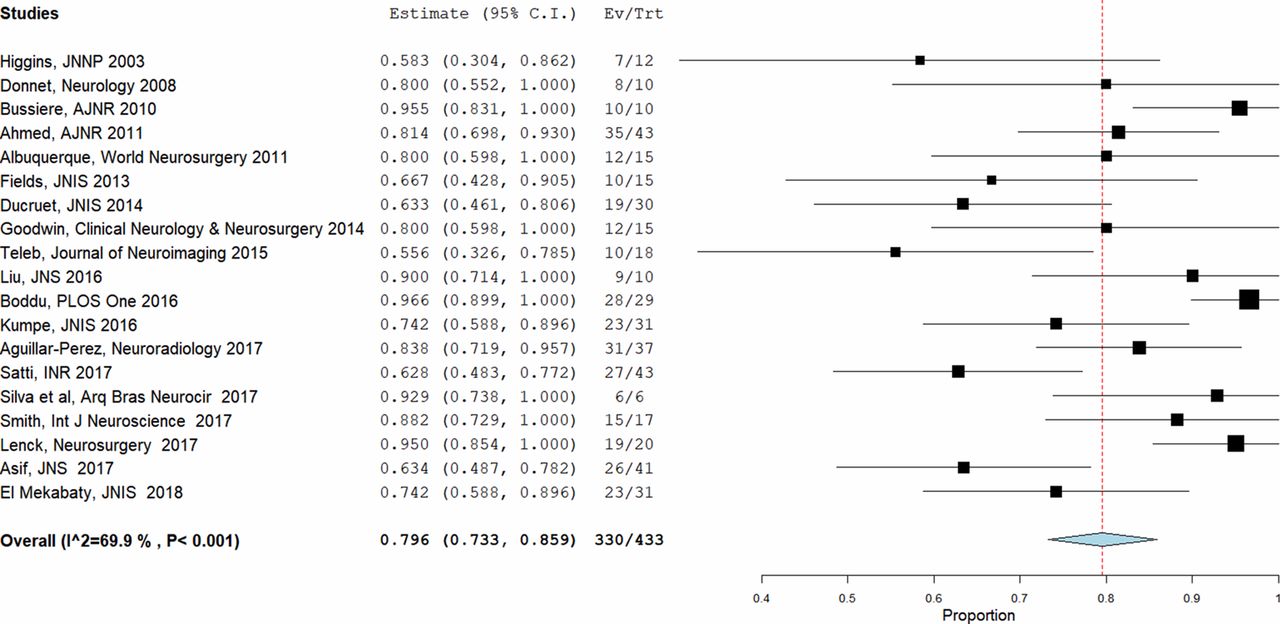
Forest plot – headache outcomes.
Pulsatile tinnitus
Outcomes for pulsatile tinnitus (PT) were specifically recorded in 11 of the studies, a total of 154 patients. Overall improvement in PT was seen in 134 of these 154 patients, or 90.3% (95% CI 83.8% to 96.70%), and the I2 figure was 63.03%, indicating significant study heterogeneity. Figure 3 contains a forest plot summarizing outcomes for PT.

Forest plot – pulsatile tinnitus outcomes.
Recurrence of IIH after stenting
Of the 474 patients, 59 had a reported recurrence of their initial symptoms after stenting requiring a second procedure – this was a repeat endovascular procedure in 43 (9%), and a subsequent CSF diversion procedure in 16 (3%). On meta-analysis, the overall rate of recurrence after stenting was 9.8% (95% CI 6.7% to 13%).
Safety and complications
All of the studies recorded ‘major’ and ‘minor’ complications, but the definition of these was not standardized. In terms of neurological complications, four patients experienced either a subdural hematoma (n=3) or subarachnoid hemorrhage (n=1) during or immediately after VSS. From these patients, all made a complete clinical recovery without long-term morbidity. Six of the studies reported that patients experienced transient worsening of headache,8–13 but not all of them specified in how many patients this occurred. For non-neurological complications, two of the studies reported a single patient experiencing a retro-peritoneal hematoma (which required transfusion but no other intervention),10 14 while two of the papers reporting a patient experiencing a post-operative pseudoaneurysm.15 16 One series reported a patient with a post-operative urinary tract infection.17 The overall mortality rate was 0%. On meta-analysis, the overall rates of major complications (ie, those with intracranial hemorrhage) was 1.9% (95% CI 0.07% to 3.1%).
Predictors of outcomes and complications
None of the clinical variables analyzed (age, BMI, pre-stenting CSF opening pressures, and whether stenting was performed as a first procedure) showed any statistically significant correlation with improvements in headache, papilloedema, or pulsatile tinnitus. Of them all, increased BMI showed the strongest positive correlation with subsequent improvement in headache but this did not reach statistical significance (P=0.121). Similarly, transtenotic gradient pressure before stenting was correlated with improvements in pulsatile tinnitus, but again this did not reach statistical significance (P=0.169). Given the low rate of major complications (n=4, or 1.9%), the study was underpowered to perform an analysis of predictors of complications.
Discussion
Our systematic review and meta-analysis of 474 patients with a clinical diagnosis of IIH who underwent venous stenting found that the procedure is associated with substantial improvement in clinical symptoms in most patients and has a satisfactory safety profile. The most significant symptomatic improvements were reported in papilledema, where 93.7% of patients experienced an improvement or resolution. Pulsatile tinnitus also showed substantial improvement, with a 90.8% rate of resolution, while outcomes for headache were more variable, with 79.6% of patients reporting an improvement or resolution of their symptoms. Despite an overall positive effect of stenting in IIH, there was significant heterogeneity of outcomes in the published studies. Overall, our study suggests that venous sinus stenting may have at least a comparable efficacy and a superior safety profile to other more established treatments such as optic nerve sheath fenestration and CSF diversion. One recently published meta-analysis on treatment options for medically refractory IIH demonstrated rates of headache improvement of only 44% after optic nerve sheath fenestration and 80% after CSF diversion. CSF diversion was also associated with lower rates of improvement in papilledema (70%) and 39.2% and 7.6% minor and major complication rates respectively.4 In our study, the most substantial symptomatic improvements after venous stenting were seen in papilledema, where 93.7% of patients experienced an improvement or resolution. Pulsatile tinnitus also showed substantial improvement, with a 90.8% rate of resolution, while outcomes for headache were more variable, with 79.6% of patients reporting an improvement or resolution of their symptoms. Subdural hematoma and subarachnoid hemorrhage have been reported as major neurological complications of VSS and occurred in less than 1% of patients. All of these patients had a complete clinical recovery, resulting in a long-term morbidity rate of 0%. There were no cases of a fatal complication in the included series. Therefore, the present meta-analysis confirms the high rates of symptom improvement demonstrated in earlier reviews.4 There appeared to be a lower rate of procedure-related complication in the more recent studies and those with larger patient numbers, suggesting a learning curve effect in venous sinus stenting.3
Mean CSF opening pressure was 37 cm H20 prior to the procedure, and decreased to 21 following the procedure, although the post-procedural CSF opening pressures were only measured in four of the studies.
In our study, the rate of recurrence of symptoms requiring a second invasive procedure was 12% after VSS. This appears to be much lower than the 43% retreatment rate observed after CSF diversion procedures.4 These recurrences were treated with another stent in 72.8% of those patients, while a CSF diversion procedure was performed in 27.2%. Recurrence seems to preferentially affect young obese patients with extrinsic stenoses and high CSF opening-pressures and is usually related to a de-novo stenosis outside the stented portion of the sinus.18 This supports the pathophysiological hypothesis of formation of extrinsic stenoses, suggesting that these stenoses are caused by compression of the transverse sinus by the congested brain and CSF spaces against the calvarium. Based on those results, some authors suggest that the length of the stent should be chosen according to the type of the stenosis to avoid recurrence of IIH.18 19 One long stent or even two stents may be required in patients with extrinsic stenoses in order to cover the transverse sinus from the torcula to the sigmoid sinus. Conversely, a single shorter stent usually seems to be enough to treat patients with intrinsic stenosis. This technical key may help reduce the recurrence rate and thus improve the results of VSS in medically refractory IIH.
Our study has limitations. Not all of the studies we have included documented the mean opening CSF pressures on lumbar puncture. However, in all included cases the primary authors documented that patients fulfilled clinical criteria for a diagnosis of IIH. For the purposes of this study we are therefore presuming that this important criterion was fulfilled before subjecting the patients to treatment, medical or otherwise, especially as these studies largely arise from experienced centres in the treatment of IIH. One other important limitation is that the included studies did not document whether trans-stenotic pressure gradients were measured under sedation or general anesthesia. This is important, as it has been documented that GA has a marked effect on intracranial venous pressure measurement.20 All of the studies were single-arm series – indeed to date there is no randomized data comparing venous stenting to other interventions. However, this is true of the early days of any emerging technique and a number of randomized trials are currently recruiting for this purpose. Other factors include that none of the studies used a standardized tool for the clinical evaluation of headache. Moreover, there is a variable range of follow-up in the studies.
Limitations common to all meta-analyses include statistical heterogeneity, the presence of publication bias, and the retrospective nature of some of the included studies, which can introduce significant selection bias. Many of the included studies had a small sample size. However, we rigorously examined the datasets from each paper before inclusion in order to minimize the bias wherever possible. We feel that this data therefore represents the best current available evidence for the use of venous sinus stenting.
Conclusion
Our study indicates that according to the published data, venous stenting for IIH appears to have an excellent safety profile and is associated with significant improvements in headaches, PT, and papilledema. Studies were mainly performed in experienced centers with rigorous patient selection criteria. Thus our data should not be generalized to all patients with IIH nor to all centers attempting to treat these challenging cases. As there is no randomized data supporting the use of venous sinus stenting in patients with medically refractory IIH, we believe that this meta-analysis provides enough evidence to support such a study in carefully selected patients.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
PRISMA flow diagram.
References
Footnotes
Contributors All authors contributed equally to the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from the study.