Article Text

Abstract
Introduction Stroke is a leading cause of adult death and disability. Although acute ischemic stroke (AIS) in pregnancy is rare, it has devastating consequences on the life of the mother and fetus. Pregnancy was an exclusion criterion in endovascular thrombectomy (EVT) trials and so there are no evidence-based treatment recommendations in this subgroup. The objective of this study was to evaluate the safety and feasibility of mechanical thrombectomy in large vessel occlusion (LVO) stroke in pregnancy.
Methods Patients with AIS due to LVO treated with EVT during pregnancy between 2000 and 2019 were identified at seven tertiary care centers. After IRB approval, retrospective analysis of prospectively maintained stroke/endovascular databases was performed.
Results A total of seven subjects were identified. The average age was 33.2 years (range 25–38 years) and the average initial National Institutes of Health Stroke Scale (NIHSS) score at presentation was 15 (range 9–28). Three patients received IV tissue plasminogen activator. Techniques of EVT included stent retriever thrombectomy, stent retriever-assisted continuous aspiration, direct contact aspiration, and multimodal techniques including a rescue balloon mounted coronary stent placement. While one patient was noted to have petechial hemorrhage, no individuals developed parenchymal hematoma. Mean discharge NIHSS score was 1.7 (range 0–5).
Conclusion EVT is a safe and effective treatment for acute stroke secondary to LVO in this series of pregnant patients. While EVT for acute stroke is standard of care in select patient populations, our study suggests that treatment should be considered in the gravid population.
- stroke
- thrombectomy
- brain
- thrombolysis
Statistics from Altmetric.com
Introduction
Stroke is the fifth leading cause of adult death and disability resulting in over $34 billion in annual cost.1 Based on the results of the National Institute of Neurological Disorders and Stroke (NINDS) trial, the Food and Drug Administration (FDA) approved intravenous alteplase (IV t-PA) as the standard of care for patients with acute ischemic stroke (AIS) presenting in the first 3 hours of symptom onset,2 3 and remained the only FDA-approved treatment in acute stroke between 1995 until 2015. The publication of six pivotal trials in 2015 demonstrated that endovascular thrombectomy (EVT) in addition to IV t-PA improved the outcomes in patients with AIS with large vessel occlusion (LVO).4–9 The DAWN and DEFUSE-3 trials subsequently demonstrated that EVT resulted in higher rates of functional independence up to 24 hours from last seen well time in patients selected based on core and clinical or perfusion mismatch.10 11 These trials had strict inclusion criteria and thus excluded many patients. Several studies have reported on the benefits of EVT in trial ineligible patients.12 13 Pregnancy was an exclusion criterion in all intravenous thrombolysis and EVT clinical trials.
The incidence of stroke in pregnancy in the USA and other Western countries is 3.8–11/100 000 gestations.14–16 Management of acute stroke in the pregnant woman poses a unique challenge as there is a potential morbidity and mortality risk to the mother and fetus. In the largest study of stroke in pregnancy and the post-partum period, Kittner et al did not find any specific etiology that predisposed pregnant women to stroke, with the exception of one subject’s use of cocaine.14 Currently, pregnancy is a relative contraindication for IV-tPA according to American Heart Association recommendations. There are very limited data on the management of LVO stroke in pregnancy. The objective of this study was to evaluate the safety and feasibility of EVT in LVO stroke in pregnancy.
Methods
A retrospective review of local prospectively-maintained AIS and endovascular databases was performed from January 2000 to May 2019 in seven participating centers in the USA and Brazil (centers A–G). Patients were included if they met the following inclusion criteria: (a) pregnant women who presented with AIS; (b) National Institutes of Health Stroke Scale (NIHSS) score ≥ 6; (c) found to have LVO (internal carotid or middle cerebral artery M1 segment occlusion); (d) treated with EVT. This study was approved by the local IRB at all participating centers. Demographic (age, sex), clinical (NIHSS score, last known well time) and radiological (non-contrast CT head and CT angiography) data were collected and analyzed by a vascular neurologist. The technical success of EVT was adjudicated using the modified Thrombolysis in Cerebral Infarction (mTICI) grade. Safety outcomes investigated included post-procedure hemorrhage, mortality, and pregnancy-related complications.
Results
Seven women were identified and all were aware of their pregnancy at the time of presentation. The mean age was 33.2 years (range 25–38 years). Two subjects were in the first trimester, two in the second trimester, and three in the third trimester of pregnancy. Six subjects were transferred to the comprehensive stroke center from peripheral hospitals and one subject presented directly to the comprehensive stroke center. Two out of seven patients in this series had a history of prior cryptogenic stroke.
Mean last known well time to presentation time was 205.5 min (range 60–611 min) and mean NIHSS at presentation was 15 (range 9–28). Three of the seven patients (42%) received IV t-PA before EVT. One subject (first trimester) had a spontaneous abortion and the other two subjects carried pregnancy to term and had a normal vaginal delivery. All seven cases used a right femoral approach for vascular access without any complications. Techniques of EVT varied in all seven patients and included stent retriever thrombectomy, a direct aspiration first pass technique (ADAPT) and, in one case, direct aspiration followed by two attempts with stent retriever thrombectomy and finally requiring a rescue balloon mounted coronary stent. All patients had post-procedure 24-hour CT head. One of the seven subjects had petechial hemorrhagic transformation 1 (HI-1), as defined by the ECASS-III classification.17 This subject had also received IV t-PA before mechanical thrombectomy. No symptomatic hemorrhages were reported in this series. Data on major early neurological improvement (reduction of NIHSS to <8 or reaching 0–1 at 24 hours18) were available in three subjects and all three subjects demonstrated early neurological improvement (table 1). Revascularization of mTICI 2b or higher was achieved in six of the seven patients and mTICI 2a in one patient.18 Average iodinated contrast usage was 156.5 mL (range 54–300 mL). Radiation exposure was available in three of the seven cases and averaged 2152 (mGy) (range 1200–3966 mGY). Two cases were performed under general anesthesia, four cases were given conscious sedation, and one had local anesthesia alone. Average discharge NIHSS score was 1.7 (range 0–5). All seven women had a good outcome (modified Rankin Scale score (mRS) <2) at 3 months without procedural or safety concerns.
Individual patient characteristics in the series
The etiology of stroke remained embolic stroke of unknown source in six patients. One case was suspected to have underlying intracranial atherosclerotic disease in the setting of polycystic ovarian disease. One patient was found to have a patent foramen ovale. None of the patients had any hypercoagulable condition identified despite a comprehensive work-up.
Discussion
In this study,we report on the safety and feasibility of endovascular treatment of AIS in pregnancy in seven cases. EVT was feasible and did not result in adverse events to the mother. Given the rarity of LVO in pregnancy and due to the exclusion of such patients from clinical trials, data related to the safety and feasibility of EVT are scarce. The reports of EVT exist only from single-center anecdotal case reports.19–23
Management of AIS in pregnancy is challenging. First, IV t-PA administration in pregnancy for suspected stroke is a complex decision with limited evidence. Recombinant tissue plasminogen activator is a large molecule and hence does not cross the placenta, precluding its entry in the fetal circulation.24 In a study of 28 pregnant patients who received IV t-PA for a variety of indications, maternal mortality was reported to be 7% and fetal mortality 23%.24 In a separate study of pregnant patients, maternal hemorrhagic risk was reported to be 8% with maternal mortality of approximately 1.2%.25 American Heart Association/American Stroke Association guidelines recommend IV t-PA administration be considered when the anticipated benefits of treating moderate to severe stroke outweigh the risk of uterine bleeding (Class IIb; level of evidence C).26
There are limited data on the outcome of pregnancy in the setting of LVO stroke. In the literature, a total of seven case reports have been described where a pregnant patient underwent EVT with or without IV t-PA.19–23 All seven case reports in the literature reported good outcomes (mRS ≤2). The previously published case reports are summarized in table 2. In our series, different techniques of thrombectomy were used based on operator experience and preference. Despite the procedural diversity, 85% (6/7 subjects) achieved a TICI 2b or higher grade of recanalization. The good outcomes in the pregnant population are likely related to young patient age as well as relative absence of traditional comorbidities; similar better outcomes were reported by Limaye et al in a study on pregnancy and subarachnoid hemorrhage.27
Individual patient characteristics in published cases of endovascular thrombectomy in pregnancy in the literature
Another important aspect of management is that of fetal exposure to iodinated contrast. Although iodinated contrast can cross the placenta, animal studies have not reported teratogenic or mutagenic effects from contrast exposure. Human studies have not demonstrated any inhibitory effect of free iodide on neonatal thyroid gland function.28 An embryo is most susceptible to adverse effects from radiation during organogenesis and the early fetal period. The radiation exposure available from three subjects ranged from 1200 to 3966 mGy to the mother and 4–5 times less than previously reported.19 In addition, all the cases were performed with low-dose fluoroscopy and an abdominal radiation shield to reduce radiation exposure to the fetus (figures 1–3).

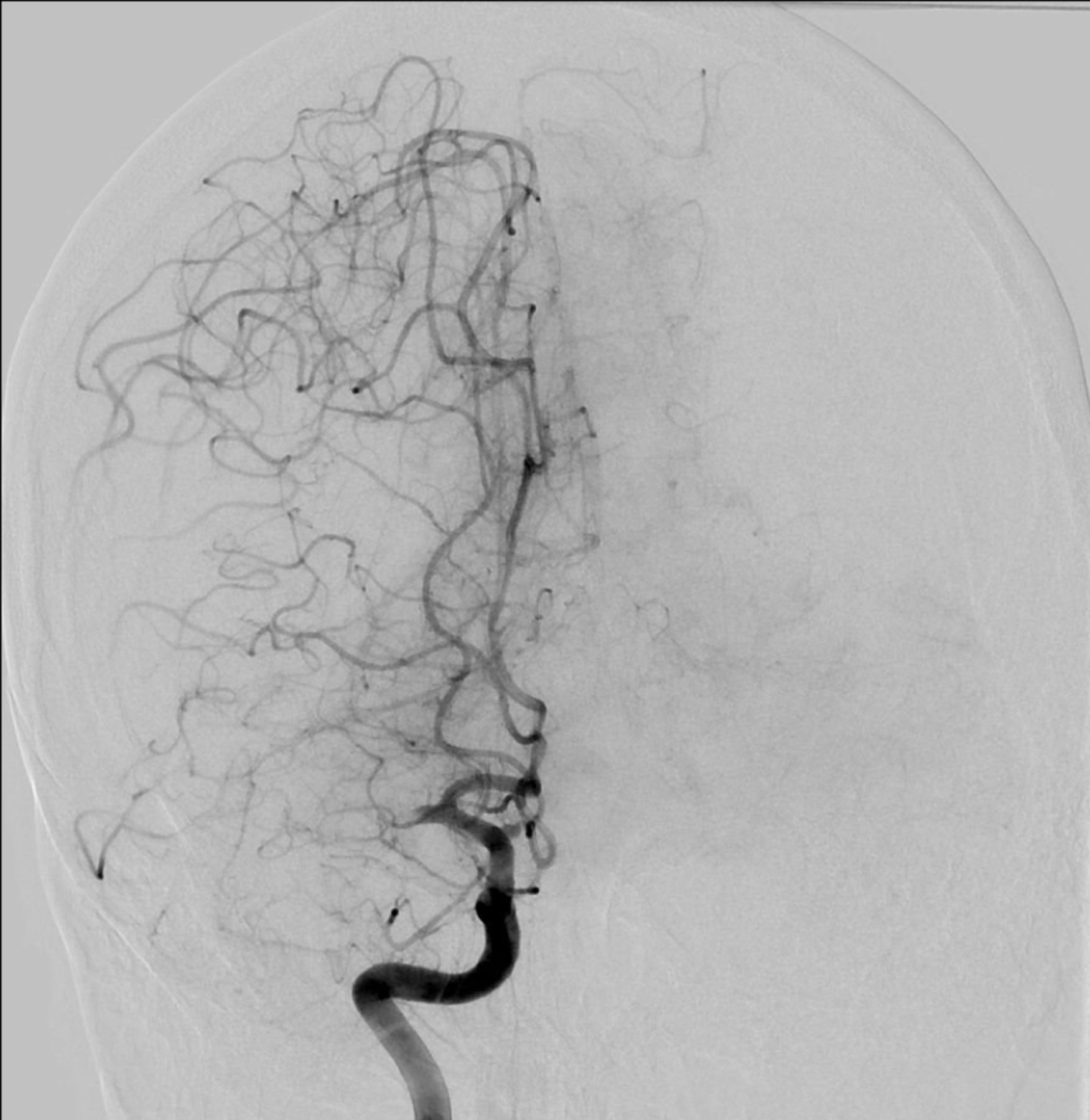
Digital subtraction angiography showing a right M1 occlusion in the anteroposterior projection (patient #1).

Post-thrombectomy digital subtraction angiography shows TICI 2b flow.
{kind=link}
{kind=link}
{kind=link}
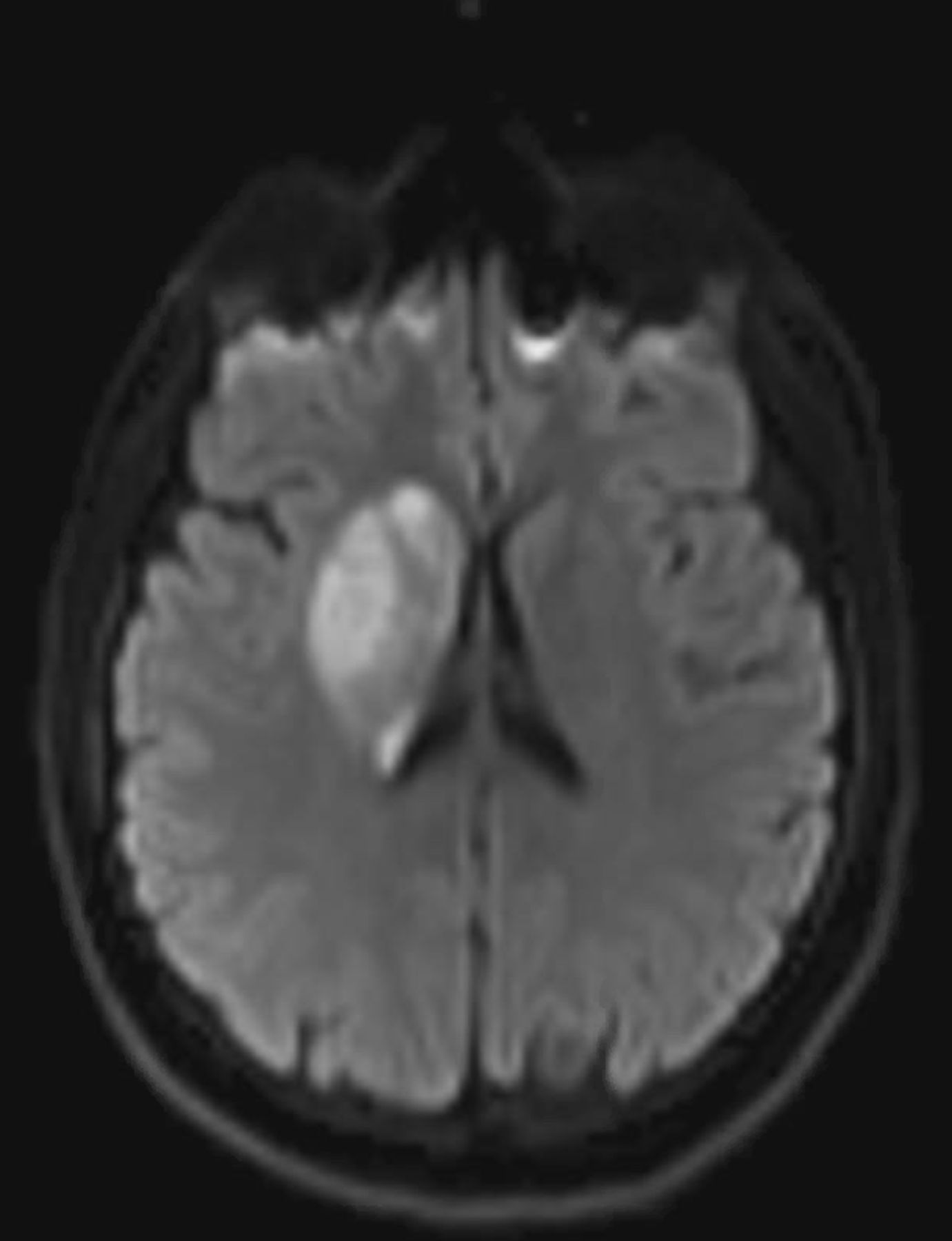
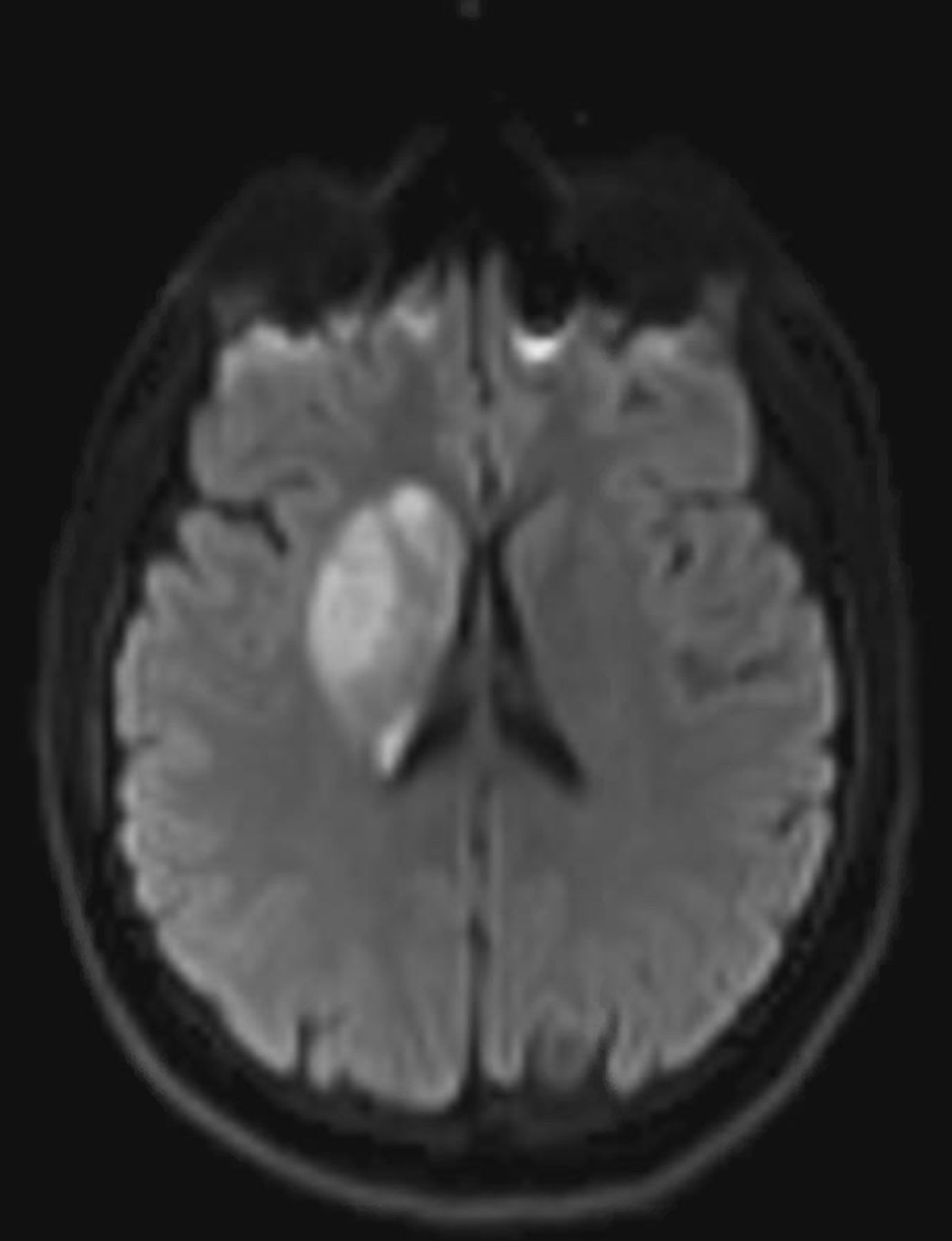
MRI shows restricted diffusion of the right lenticular nucleus and basal ganglia signal on diffusion-weighted imaging.
Despite the small sample size, our study is the largest series of pregnant patients undergoing EVT for management of AIS due to LVO. In a population-based study by Wiebers et al in the city of Rochester, Minnesota from 1955 through 1979, only one ischemic stroke was reported in 26 099 women giving birth.15 Our study is limited by its retrospective nature but is generalizable as these seven cases were performed in seven different institutions and in two countries.
Conclusion
EVT is a safe and feasible procedure for treating AIS due to LVO in pregnancy. We recommend that it should be considered for pregnant women presenting with AIS due to LVO.
References
Footnotes
Twitter @kaustubhslimaye
Contributors All authors were involved in all of the following: (1) conception and design, or acquisition of data, or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content; (3) final approval of the version to be published; and (4) agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.