Article Text

Abstract
Background It is not clear whether the COVID-19 pandemic and subsequent Society of Neurointerventional Surgery (SNIS) recommendations affected hospital stroke metrics.
Methods This retrospective cohort study compared stroke patients admitted to a comprehensive stroke center during the COVID-19 pandemic April 1 2020 to June 30 2020 (COVID-19) to patients admitted April 1 2019 to June 30 2019. We examined stroke admission volume and acute stroke treatment use.
Results There were 637 stroke admissions, 52% in 2019 and 48% during COVID-19, with similar median admissions per day (4 vs 3, P=0.21). The proportion of admissions by stroke type was comparable (ischemic, P=0.69; hemorrhagic, P=0.39; transient ischemic stroke, P=0.10). Acute stroke treatment was similar in 2019 to COVID-19: tPA prior to arrival (18% vs, 18%, P=0.89), tPA treatment on arrival (6% vs 7%, P=0.85), and endovascular therapy (endovascular therapy (ET), 22% vs 25%, P=0.54). The door to needle time was also similar, P=0.12, however, the median time from arrival to groin puncture was significantly longer during COVID-19 (38 vs 43 min, P=0.002). A significantly higher proportion of patients receiving ET were intubated during COVID-19 due to SNIS guideline implementation (45% vs 96%, P<0.0001). There were no differences by study period in discharge mRS, P=0.84 or TICI score, P=0.26.
Conclusions The COVID-19 pandemic did not significantly affect stroke admission volume or acute stroke treatment utilization. Outcomes were not affected by implementing SNIS guidelines. Although there was a statistical increase in time to groin puncture for ET, it was not clinically meaningful. These results suggest hospitals managing patients efficiently can implement practices in response to COVID-19 without impacting outcomes.
- COVID-19
- standards
- stroke
- thrombectomy
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The novel coronavirus disease 2019 (COVID-19) pandemic has affected the delivery of healthcare services in unprecedented ways.1 Studies have shown an absolute decrease in the number of stroke patient admissions and stroke alerts, and it has been suggested that patients may not be receiving care for stroke symptoms due to fear of contracting COVID-19 in the hospital.2 3
Recent studies demonstrate an association between COVID-19 diagnosis and stroke, although the exact pathophysiology has yet to be determined.4–7 Moreover, patients with COVID-19 and a history of cerebrovascular disease have a higher likelihood of developing severe symptoms and a higher risk for mortality.8 9
In order to protect patients and providers during the COVID-19 pandemic, the Society of NeuroInterventional Surgery (SNIS) published recommendations for the care of emergent neurointerventional patients with ischemic infarct in the setting of COVID-19.10 These recommendations were implemented at our institution, including intubating COVID-19 positive and unknown COVID-19 status patients prior to endovascular thrombectomy, cohorting patients by COVID-19 diagnosis, early intensive care unit (ICU) disposition, and postponing elective cases.10 Similarly, the American Heart Association/American Stroke Association’s temporary emergency guidance for US stroke centers states that stable stroke patients be treated in step-down or other units to preserve space in the ICU and to cohort patients by their COVID-19 diagnosis.11
While the SNIS recommendations may decrease the spread of COVID-19 and protect providers, they could lead to an increased time to endovascular therapy (ET) especially when considering the time to complete the intubation process. This could negatively impact patient outcomes.
The objectives of this study were: to describe the differences in the volume of stroke patient admissions and treatment patterns between patients admitted during the COVID-19 pandemic and those admitted in 2019; and to describe the differences in patient demographics, clinical characteristics, time to treatment, and intubation practices among patients with ischemic stroke treated with ET during the COVID-19 pandemic compared with 2019.
Methods
This was a retrospective cohort study of patients with acute stroke [ischemic stroke, hemorrhagic stroke, or transient ischemic stroke (TIA)] who were admitted to a comprehensive stroke center over two time periods: during COVID-19 (April 1 2020 to June 30 2020) and a comparable time period in 2019 (April 1 2019 to June 30 2019). Similar time periods were used to control for bias. April 1 was used as the cut-off for selecting patients for this study as that was when the SNIS recommendations were implemented at our institution. This study was approved by the HealthOne Institutional Review Board. Two groups are described: overall patients admitted with stroke (hemorrhagic, ischemic, or TIA), and patients with an ischemic stroke who were treated with ET.
The SNIS recommendations during the COVID-19 pandemic separated their guidance based on the patient’s COVID-19 status. All SNIS recommendations were implemented at this comprehensive stroke center. They recommend standard personal protective equipment (PPE) precautions for all admissions including those with a documented negative COVID-19 test within 48 hours of arrival.10 For patients positive for COVID-19 or those presumed positive, the SNIS recommends wearing enhanced PPE at all times (N95 or powered air purifying respirator), intubating patients prior to transport to the angiography suite, ideally a negative pressure environment, and not extubating patients in the angiography suite unless it is a negative airflow environment. Intubation maintains a closed circuit and therefore decreases the risk of COVID-19 exposure to healthcare staff. Patients with an undocumented COVID-19 status are recommended to be screened for symptoms and treated as if they are COVID-19 positive.
Additional recommendations from the SNIS include early ICU discharge for uncomplicated post-thrombectomy patients, development of aggressive protocols to recover thrombectomy patients in non-ICU settings, testing of all patients for COVID-19 after thrombectomy, and postponing elective and non-urgent cerebrovascular procedures. For centers with multiple angiography suites, they recommend cohorting patients by COVID-19 status and stocking designated COVID-19 treatment rooms with additional PPE.
For the overall stroke patient population, outcomes included the volume of stroke admissions per day, type of stroke, and acute stroke management [intravenous tissue plasminogen activator (IV tPA) treatment and ET]. For patients who were treated with ET, outcomes included time from arrival to groin puncture, intubation rate, re-intubation rate, total days intubated, number of times intubated, door to needle time, time from stroke onset to arrival, and clinical outcomes including recanalization achieved, ICU length of stay (LOS), hospital length of stay (HLOS), thrombolysis in cerebral infarction (TICI) score, discharge modified Rankin Scale (mRS), and discharge disposition.
Continuous data are summarized as mean (SD) or median (IQR) based on the data distribution and were compared using student’s t-test or Kruskal–Wallis test when appropriate. Dichotomous and categorical data are summarized as proportions (counts) and were compared using Pearson’s chi-squared or Fisher’s exact test. An alpha of 0.05 was used to indicate statistical significance.
Results
Overall stroke population
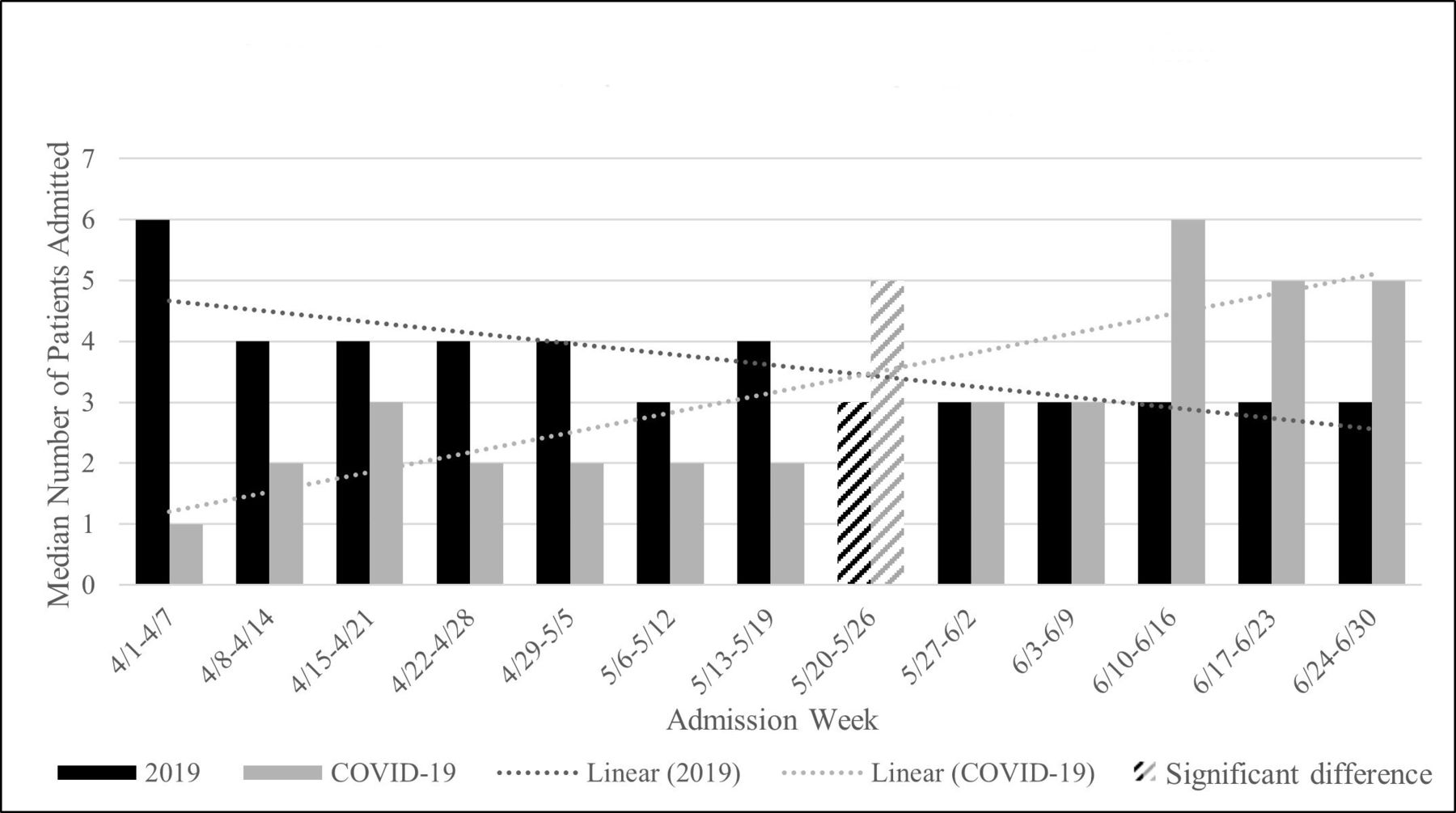
There were 637 patients, 52% (333) in 2019 and 48% (304) during COVID-19, a 9% (29) decrease in stroke admissions. Figure 1 displays the median number of patients per day admitted by admission week for each study group. From April through mid-May, there was consistently a higher median number of patients per day in 2019 than during COVID-19, however, none of these differences were significant. Over time, the median number of patients per day decreased in 2019, whereas it increased during COVID-19. By the week of May 20 to May 26, the median number of patients per day shifted, and there was a significantly lower median number of patients admitted in 2019 than there was during COVID-19, 3 vs 5, P=0.03. From mid-to-late June there was consistently a lower median number of patients per day in 2019 than during COVID-19.
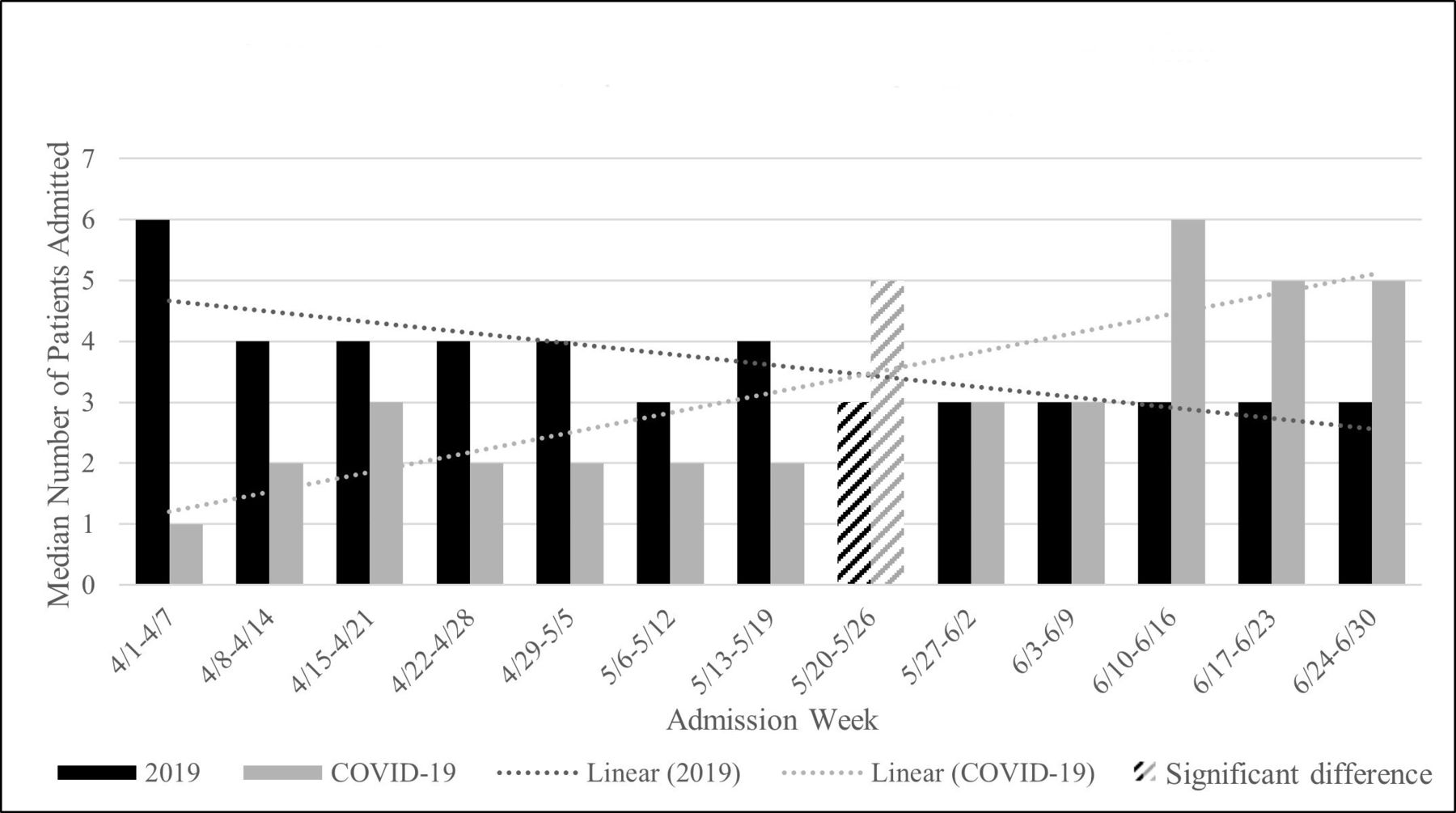
Median number of patients admitted per day by admission week and study group.
Across the entire study period, there was a median of four admission per day in 2019 and three admissions per day during COVID-19, P=0.21 (table 1). As shown in table 1, there were no differences in age, race, or transfer status by study period. There was a significantly higher proportion of males admitted in 2019 compared with during COVID-19, 57% vs 45%, P=0.002. A majority of patients had ischemic strokes, 77% in 2019 vs 78% during COVID-19, P=0.69. The proportion of patients with hemorrhagic strokes was also comparable, 16% in 2019 vs 19% during COVID-19, P=0.68. There was a higher proportion of patients with TIA in 2019, 11%, than during COVID-19, 8%, but this was not significant, P=0.10.
Stroke patient volume and diagnoses
Among patients with ischemic strokes, there was a similar proportion of patients who received tPA prior to arrival in 2019 and during COVID-19 (18% vs, 18%, P=0.89), as well as in patients who received IV tPA treatment on arrival (6% vs 7%, P=0.85). The door to needle time was similar between groups (14 min vs 22 min, P=0.10). There was also a similar proportion of patients who received ET in 2019 and during COVID-19 (22% vs 25%, P=0.54).
Patients treated with endovascular therapy
There were 112 patients treated with ET, 49% (55) in 2019 and 51% (57) during COVID-19. Similar to the overall stroke population, the mean number of patients treated with ET per day in 2019 decreased over time, whereas the mean number of patients treated with ET per day during COVID-19 increased over time (figure 2). In early April through April 21st, there was a higher mean number of ET patients per day in 2019 than during COVID-19, but this was not significant. By the week of April 22nd to April 28th, the mean number of patients treated with ET per day was the same for each group. In the week of June 17th to June 23rd, there was a significantly lower mean number of ET patients per day in 2019 than during COVID-19, P=0.02.

Mean number of endovascular therapy patients per day by admission week and study group.
Across the entire study period, there was no difference in the mean number of patients treated with ET per week (table 2). As shown in table 2, there were no differences by study period in age, race, comorbidities, or transfer status. There was a higher proportion of male patients in 2019 than during COVID-19 (64% vs 46%), but this was not significantly different, P=0.06.
Characteristics for patients treated with endovascular therapy
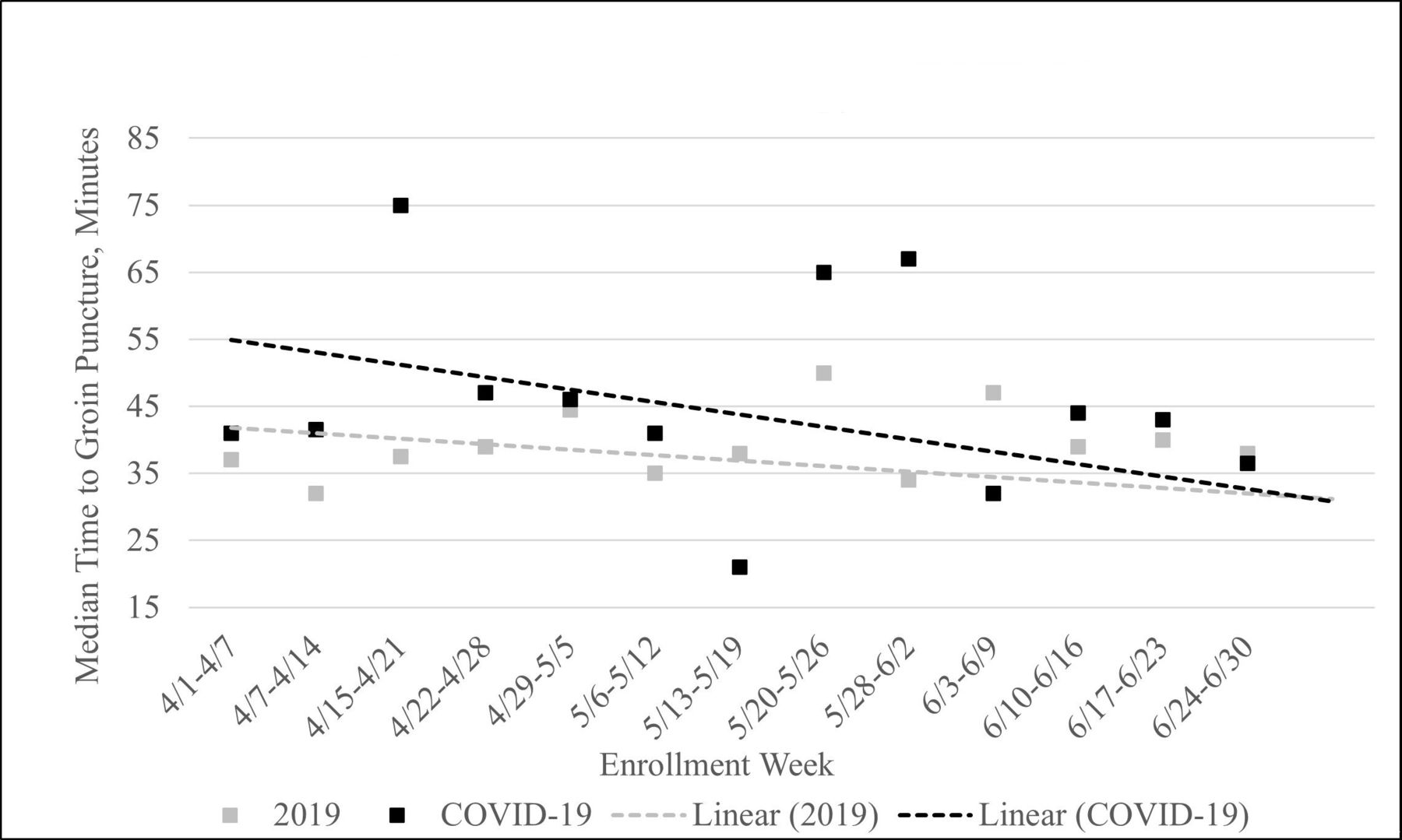
Figure 3 displays the median time from arrival to groin puncture for ET summarized by enrollment week for each study group. Patients admitted during COVID-19 typically experienced longer times from arrival to groin puncture than patients admitted in 2019. There appeared to be an increase in the median time from arrival to groin puncture over time in 2019, whereas during COVID-19 the median time from arrival to groin puncture was relatively consistent with a very slight downward trend. There was only one week with significant difference in the median time from arrival to groin puncture for ET: from May 28th to June 2nd the median time from arrival to groin puncture for ET was significantly longer during COVID-19 than in 2019, P=0.01. For the remaining weeks, the median time from arrival to groin puncture for ET were statistically similar between groups.
{kind=link}
{kind=link}
{kind=link}
TIme from arrival to groin puncture for endovascular therapy by week.
The overall median time from arrival to groin puncture for ET was significantly shorter in 2019 than during COVID-19 (38 min vs 43 min, P=0.002), table 2. The median time from the patient’s symptom onset to hospital arrival was statistically similar for patients in 2019 compared with patients during COVID-19, 310 min vs 221 min, P=0.14. As shown in table 2, the median time from arrival to recanalization, the door to needle time, the proportion of patients who received tPA prior to arrival, and who received tPA on admission were similar between groups.
Compared to 2019, there was a significantly higher proportion of patients who were intubated during COVID-19, 45% vs 96%, P<0.0001. The time to extubation, proportion of patients who were intubated again after the initial extubation (re-intubated), total days intubated, and the total number of times intubated during the patient’s entire hospitalization, were statistically similar between groups. A lower proportion of patients had a TICI score of 2B, 2C, or 3 in 2019 than during COVID-19, 85% vs, 92%, P=0.26. No differences were observed for intensive care unit length of stay, or hospital length of stay. The median discharge mRS was 4 for both groups, P=0.84.
Discussion
In the midst of the COVID-19 pandemic, guidelines for many aspects of medicine have changed and the world of neurointerventional surgery is no different.10 As the number of COVID-19 positive patients continues to rise, a link between COVID-19 and large-vessel occlusions requiring mechanical thrombectomy has been observed.5 6 12 As a corollary to the rise of COVID-19 positive patients and risk for stroke among said patients, there is an increased risk of healthcare workers contracting the illness as well.13 In response to COVID-19 the SNIS provided a guideline for the management of neurointerventional patients.10 The study was successful in describing differences in patient demographics, clinical characteristics, time to treatment, and intubation rates before and after the implementation of the SNIS guidelines.
In this retrospective cohort study the characteristics for ET patients were similar. Although there was a 9% decrease in strokes (333 patients in 2019 and 304 during COVID-19), there were no differences in the time from onset to arrival, type of stroke, or number of stroke patients admitted per week. Implementing the SNIS guidelines resulted in a significant increase to the proportion of patients intubated and time to groin puncture for ET, however overall patient outcomes including TICI score, discharge mRS, HLOS, and discharge disposition, were not significantly impacted. This suggests that, while there was a slight increase in the median time from arrival to groin puncture, there was no significant impact of the COVID-19 pandemic and SNIS guidelines on patient outcomes including recanalization rates.
Bres Bullrich et al also observed a decrease in the number of coded strokes during COVID-19 but no difference in the number of stroke admissions per day.3 The decrease in coded strokes was more than double that observed in this study, 20% vs 9%. Another study at five US comprehensive stroke centers reported a significant decrease in the trend of stroke and TIA admissions between December 31 to April 21 in 2019 compared with the same time period the following year.2 The cut-off times for inclusion in this study (April 1 to June 30) could have played a role in why there was no difference observed for overall stroke admissions in this study. It was observed that early in the pandemic there were less stroke admissions and over time the stroke admissions increased. For one week (May 20th to May 26th) there was actually a statistically higher median number of patients admitted during COVID-19 than the year prior. Anecdotally, that was when the physicians remarked that things began to pick up and more patients were admitted during the COVID-19 pandemic period. Although it was anticipated that fear of hospital might be leading to delayed care among stroke patients, time from onset to arrival was comparable between groups in our study and among a study conducted by Sharma et al2, whereas Frisullo et al reported a significant increase of 226 min in the median time from onset to arrival.14 Schirmer et al also reported a significant increase in time from onset to arrival among patients admitted during COVID-19 when compared topatients admitted in 2019, 603 vs 442 min, P<0.02.15
The tPA administration rate and door to needle time also was not affected by the COVID-19 pandemic in this study. Zhoa et al compared the type of treatment used during COVID-19 to previous time periods and reported a significant decrease in the number of patients treated with thrombolysis or thrombectomy.16 However, multiple factors could have played a role in their decreased rate of thrombolysis treatment: their center was designated as a COVID-19 treatment center, the study was conducted in China at the height of the pandemic, and they also observed a 40% decrease in stroke admissions. Another study also reported a significant reduction in the proportion of patients treated with thrombolysis.14 Tan et al reported 77% of COVID-19 patients with stroke were treated with thrombolysis, which is much higher than the tPA administration rate in this study for all patients with ischemic stroke, 37% prior to arrival and 9% in hospital.5 This finding could be due to differences in the type of occlusion, as prior studies examining strokes among COVID-19 positive patients have remarked on the higher rate of large-vessel occlusions.7
Prior to the COVID-19 pandemic the indication for intubation of patients undergoing ET at our institution included the following: patients with distal occlusions, patients unable to protect their airway, and patients who were unable to follow commands and thus posed a risk with movement. Given the near universal intubation policy for all patients undergoing ET which was implemented based on SNIS guidelines during COVID-19, the intubation rate expectantly differed significantly with 45% in 2019 vs 96% of patients intubated during COVID-19. All patients were successfully extubated and there was no difference in the median total days intubated between groups. The SNIS guidelines also recommend that intubation take place in a negative pressure room prior to the patient being brought to an angio suite for ET.10 This recommendation could have impacted the overall arrival to groin puncture time by increasing the transport time.
The median time from arrival to groin puncture for ET differed by a value of five minutes and this difference was statistically different. Frisullo et al also reported a significant increase in the time from arrival to groin puncture, 120 min during COVID-19 compared with 93 min in 2019, P=0.048.14 In their study they followed the WHO recommendations on cohorting patients by COVID-19 status but made no other mention of changes to treatment during COVID-19.14 The increase observed in their study could have been in part due to the high infection rate of COVID-19 in Italy at the time of their study, their designation as a COVID-19 treatment center, and use of preoperative screening for COVID-19 that could have delayed care. In our study we also observed that as time progressed during the COVID-19 pandemic, the median time from arrival to groin puncture slightly decreased. This could be a result of treating physicians acclimating to the new guidelines implemented and improving the metric over time. In addition to implementing the SNIS guidelines, at our center the anesthesiologists were stationed in the control room, responded to all stroke alerts, and were conducting intubation. Through this process, anesthesiologists were getting information on the patients earlier than normal, which may have facilitated a faster time to intubation and thus may have affected the time from arrival to groin puncture. Other than the implementation of SNIS guidelines, there are several other factors that could affect the median time from arrival to groin puncture time at individual stroke centers. At our institution, the expeditious time from arrival to groin puncture may result from acute stroke protocols that implement an alert to the neurologist, neurointerventionalist, and anesthesiologist, and protocols which standardize neurointerventional thrombectomy: the latter has been shown to result in faster times from arrival to groin puncture.17 Another factor depends on the relative expertise of the anesthesiologist or emergency medicine physician in performing intubations. This could be in part why the time from arrival to groin puncture was shorter in this study when compared with Frisullo et al.14 Although the difference in time from arrival to groin puncture was significant, it was only five minutes different and did not appear to affect patient outcomes.
Limitations
This study was limited by the short period of enrollment (three months). This study also represents patients admitted to a single comprehensive stroke center and therefore may not be generalizable to other stroke centers. The time of stroke onset may not have been known or could be an estimation.
Conclusions
Although many centers have reported a significant decrease in stroke patient admissions, the COVID-19 pandemic did not significantly affect patient volume or the time from stroke symptom onset to arrival at our institution. As the pandemic continues, it is important for hospitals to be informed that COVID-19 may not impact stroke volume, so providers are prepared to manage both stroke and COVID-19 patients efficiently. Additionally, we were able to adopt and implement the SNIS guidelines to protect staff and the procedure environment efficiently enough to not compromise patient outcomes.
A more universal implementation of the SNIS recommendations, including intubation prior to ET, increased the median time from arrival to groin puncture by five minutes. While the difference in time was statistically significant, patient outcomes were not negatively impacted. This study shows that implementation of the SNIS guidelines does not negatively affect patient outcomes in terms of recanalization rate, mRS, HLOS, or discharge disposition, suggesting that hospitals who manage stroke patients efficiently can implement safe management practices in response to COVID-19 without impacting outcomes.
We recommend following SNIS guidelines to prevent the spread of COVID-19 during the pandemic or possible future pandemics. By implementing this policy there is the benefit of helping prevent the spread of COVID-19 to healthcare workers while still providing the best patient care.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Hospital Corporation of American (HCA) HealthONE Institutional Review Board. The study approval number is 779 117.
References
Footnotes
Twitter @donfreimd
Correction notice This article has been corrected since it appeared Online First. Author Kristin Salotollo has been corrected to Kristin Salottolo.
Contributors All authors were involved in the study conception. SJ and KS were involved with study design. ES, AN, and KM were involved with acquisition of data. SJ and KS were involved with analysis of data. All authors were involved with interpretation of data. SJ, KS, and ES were involved with drafting the manuscript. All authors assisted with revising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.