Article Text

Abstract
Introduction Imaging still serves as an integral tool for stroke validation and intervention. Limited data is available as to whether performing CTA immediately following non-contrast CT (NCCT) will delay overall treatment time. Centers conducting concurrent NCCT and CTA relative to those performing NCCT alone were evaluated to determine whether having additional imaging extends hospital workflow, prolonging time to IV rtPA and subsequently to endovascular intervention, where warranted.
Materials and methods A total of 108 patients were enrolled in the THERAPY trial, a randomized controlled trial designed to assess the benefits of adjunctive mechanical thrombectomy plus IV rtPA versus IV rtPA alone. Standard emergency department (ED) protocols for participating centers are registered as either conducting concurrent NCCT and CTA (N = 22) or postponed acquisition of CTA (N = 13). The effects of having concurrent imaging modalities are evaluated for all patients as well as singly for patients undergoing endovascular therapy.
Results Patients having the relevant data for analysis totaled 105 amongst 35 centers. Sixty-six patients received concurrent imaging processes across 22 centers, while 39 patients between 13 centers received sequential NCCT and CTA imaging.
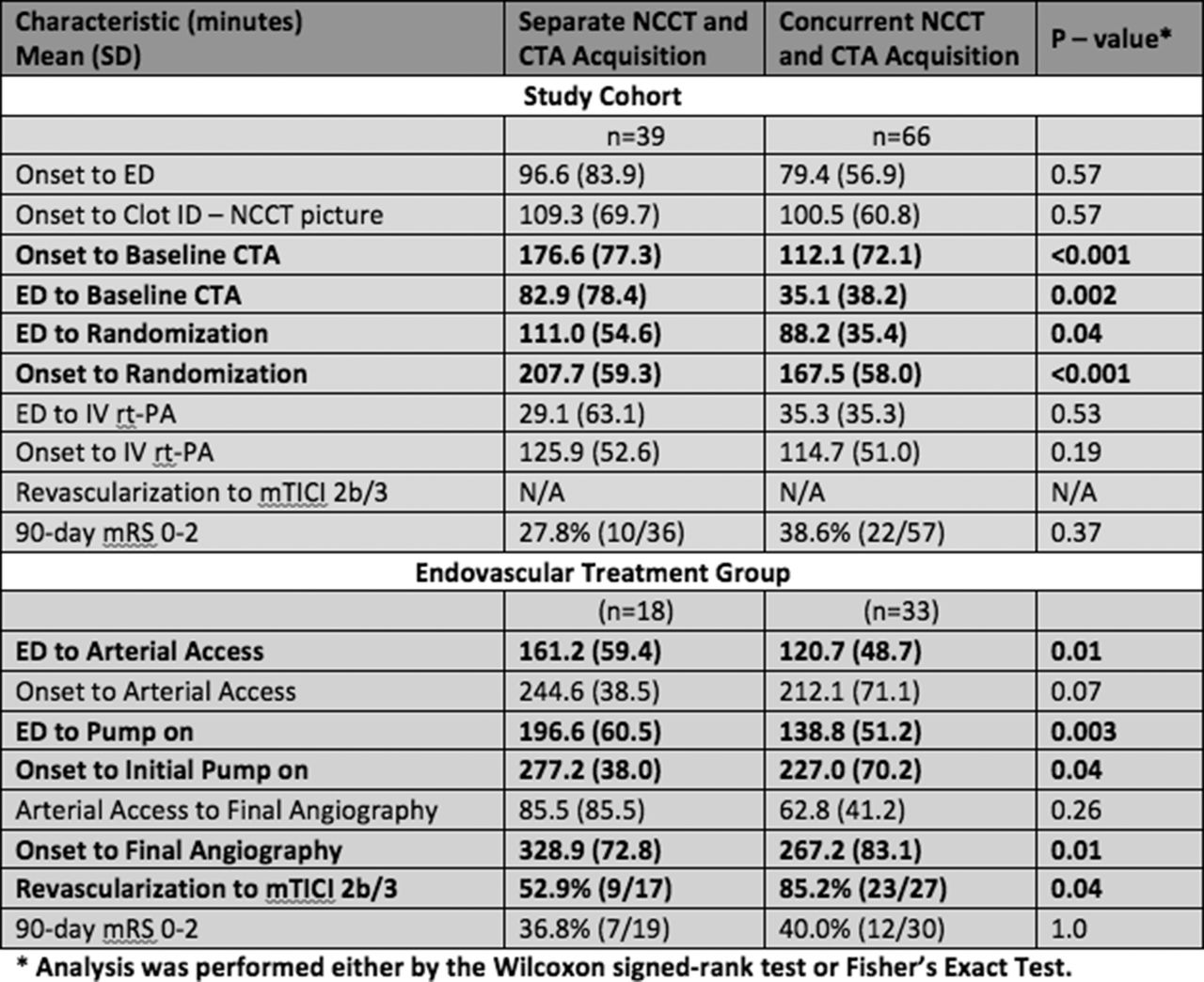
For all patients, clear benefits of having both NCCT and CTA in conjunction were a reduction in time from presentation at the ED to randomization, and consequently from onset to randomization (Table 1). No significance difference in time was observed from admission to IV rtPA administration in this population.
{kind=link}
Separate and concurrent NCCT/CTA angiography-related hospital processing times
More significant differences were observed in the EVT cohort, including a reduction in the time from presentation to arterial access of roughly 40 minutes (p = 0.01) for patients having NCCT and CTA performed concurrently. As a result, downstream effects of the procedure demonstrated a reduction in time from presentation to aspiration thrombectomy initiation, from onset to aspiration, and from onset to final angiography (all p < 0.05). Notably, these patients demonstrated a higher rate of revascularization to mTICI 2 b-3 (p = 0.04).
Conclusion The effects on procedural and clinical outcome of having combined imaging efforts were less apparent in the entire cohort relative to the EVT cohort. These results suggest having concurrent NCCT and CTA imaging improves time from presentation to endovascular therapy, without significant delay to IV rtPA infusion. More patients were observed to achieve mTICI 2 b-3 if both imaging procedures were obtained in conjunction, possibly as a result of the reduction in time to endovascular intervention in this cohort. Further data from a larger sample size will help validate these findings.
Disclosures O. Zaidat: 6; C; Penumbra, Inc. B. Mehta: None. A. Yoo: 1; C; National Institute of Health, Penumbra, Inc., Remedy Pharmaceuticals. R. von Kummer: 2; C; Penumbra, Inc. P. Khatri: 1; C; Penumbra, Inc. R. Gupta: 6; C; Penumbra, Inc. D. Lopes: 6; C; Penumbra, Inc. D. Frei: 3; C; Penumbra, Inc. 6; C; Penumbra, Inc. H. Shownkeen: None. D. Meyer: 5; C; Penumbra, Inc. V. Bach: 5; C; Penumbra, Inc. H. Buell: 5; C; Penumbra, Inc. S. Kuo: 5; C; Penumbra, Inc. A. Bose: 4; C; Penumbra, Inc. 5; C; Penumbra, Inc. S. Sit: 4; C; Penumbra, Inc. 5; C; Penumbra, Inc. J. Mocco: 1; C; Penumbra, Inc.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work noncommercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/