Article Text

Abstract
The pipeline embolization device (PED) has become a routine firstline option for the treatment of an increasing population of intracranial aneurysms at many neurovascular centers. Intraprocedural complications during PED deployment, or complications associated with migration of the device, are rarely reported problems. Significant mismatch in luminal diameter between the inflow vessel and the outflow vessel or excessive dragging–stretching of the PED have been related to ‘watermelon seed’ or ‘accordion’ effects, respectively, resulting in stent migration. Here we present a novel balloon technique that was successfully used to realign an in situ flow diverting stent that had prolapsed into a large aneurysm. This represents a useful salvage technique and should be considered when encountering this potential complication.
- Aneurysm
- Flow Diverter
Statistics from Altmetric.com
Background
The pipeline embolization device (PED) (Medtronic-Covidien Neurovascular, Irvine, California, USA) has become a routine firstline option for the treatment of an increasing population of intracranial aneurysms at many neurovascular centers.1 Intraprocedural complications during PED deployment are infrequently reported, and complications associated with migration of the device are rarely reported problems.2–8 Stent migration can precipitate serious complications, including vessel thrombus, aneurysm rupture, endothelial damage during retrieval, or dislodging of embolic material with subsequent stroke.9–11
Here we present a technical report of a salvage technique that was used to overcome a proximal end device foreshortening and migration into the aneurysm sac.
Case presentation
A patient in his/her sixties presented with dizziness and fatigue. MR angiography and subsequent CT angiography demonstrated a wide neck 14 mm left supraclinoid aneurysm. Considering the location and size of the aneurysm, as well as the patient's age, endovascular treatment with a PED was recommended.
Treatment
Plavix 75 mg/day and aspirin 100 mg/day were given from 5 days prior to the intervention. The procedure was performed under general anesthesia. Heparin was administered at the beginning of the procedure and intermittently during the procedure to maintain the activated clotting time between 250 and 290 s.
A Navien 072 guide catheter (Medtronic-Covidien Neurovascular) was navigated into the left internal carotid artery (ICA) through a Flexor Shuttle 087 guiding sheath (Cook Medical, Bloomington, Indiana, USA); a Marksman microcatheter (Medtronic-Covidien Neurovascular) was advanced into the left middle cerebral artery (MCA) trunk.
We decided to deploy the distal end of the PED in MCA, considering the short landing zone of the distal ICA above the aneurysm neck.
A 4×18 mm pipeline Flex embolization device was deployed through the Marksman catheter across the neck of the aneurysm (figure 1A–C). The device diameter was chosen according to the diameter of the larger proximal parent artery, with the understanding that it would be slightly oversized in the distal ICA, hopefully resulting in stronger device purchase in the distal vessel.

(A) Digital subtraction angiography showing a large supraclinoid aneurysm. Fluoroscopic images—lateral view. (B, C). Pipeline Flex embolization device deployment 4×18 mm from the M1 segment to the proximal supraclinoid internal carotid artery. (D) First angiographic run after deployment showing the proximal end of the device herniated at the inflow entrance of the aneurysm.
Following PED deployment and Marksman withdrawal, the proximal aspect of the PED foreshortened. This caused the device to lose its purchase in the supraclinoid ICA and prolapse into the aneurysm (figure 1D).
Multiple attempts were made to regain access through the PED utilizing a variety of microwires and microcatheters shapes (‘hockey stick,’ 90°, and C shaped), but they all failed. Due to the location of the proximal end of the PED at the inflow entrance of the aneurysm, the microwire had to take two sharp 90° turns, the first in the proximal parent vessel near the neck and the second into the proximal device orifice from the aneurysm sac.
Finally, the decision was made to modify the location of the proximal end PED from the inflow to the outflow portion using a balloon technique, favoring the regain access.
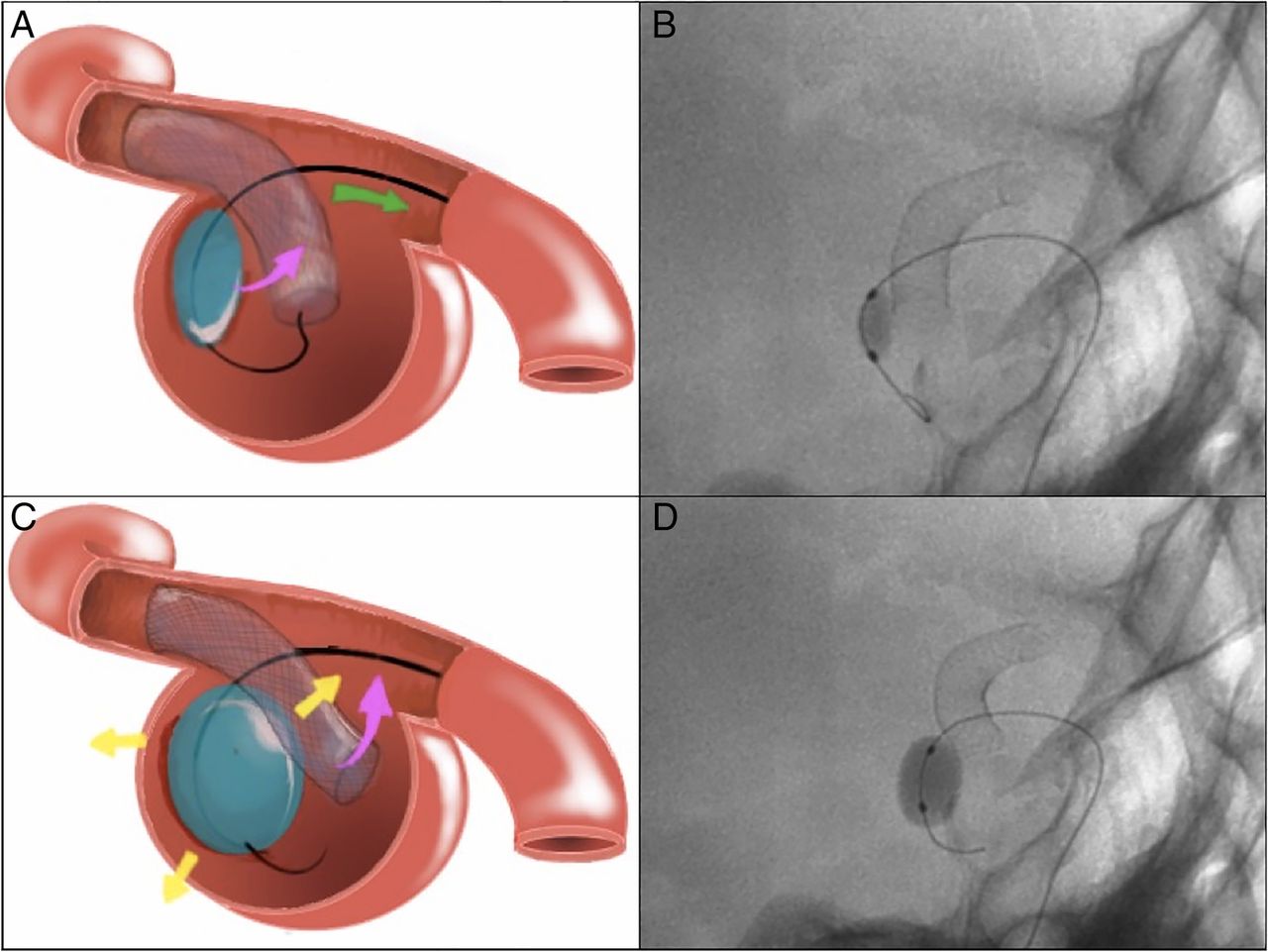
A 4×7 mm Hyperform balloon was advanced into the inflow entrance of the aneurysm, between the PED and the posterior aneurysm wall (figure 2A, B). The balloon was then inflated and the balloon catheter was gently retracted until the proximal end PED reached an ‘outflow position’ (figure 2C, D). The balloon was kept inflated and a second J shaped Synchro-2 microwire was navigated and advanced distally through the PED to the M2 segment. Considering the support of the Synchro-2 microwire, which maintained the PED at the ‘outflow position’, the balloon was deflated and then navigated through the PED over the wire (figure 3A, B).
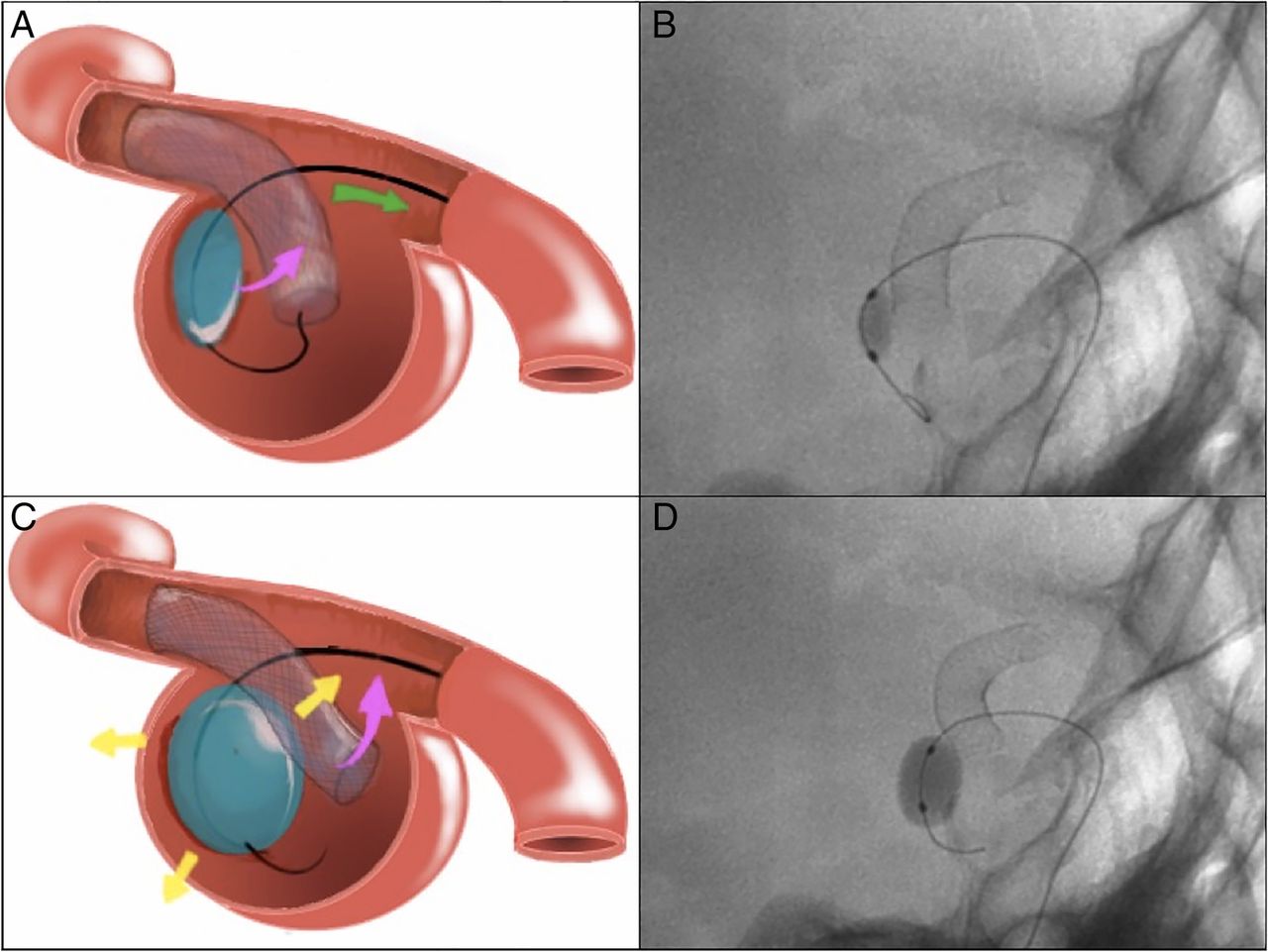
Illustrations and fluoroscopic images. Lateral view. (A, B) A 4×7 mm Hyperform balloon was advanced into the inflow entrance of the aneurysm, between the pipeline embolization device (PED) and the posterior aneurysm wall. (C, D) The balloon was then inflated, and the balloon catheter was gently retracted until the proximal end of the PED reached an ‘outflow location’.

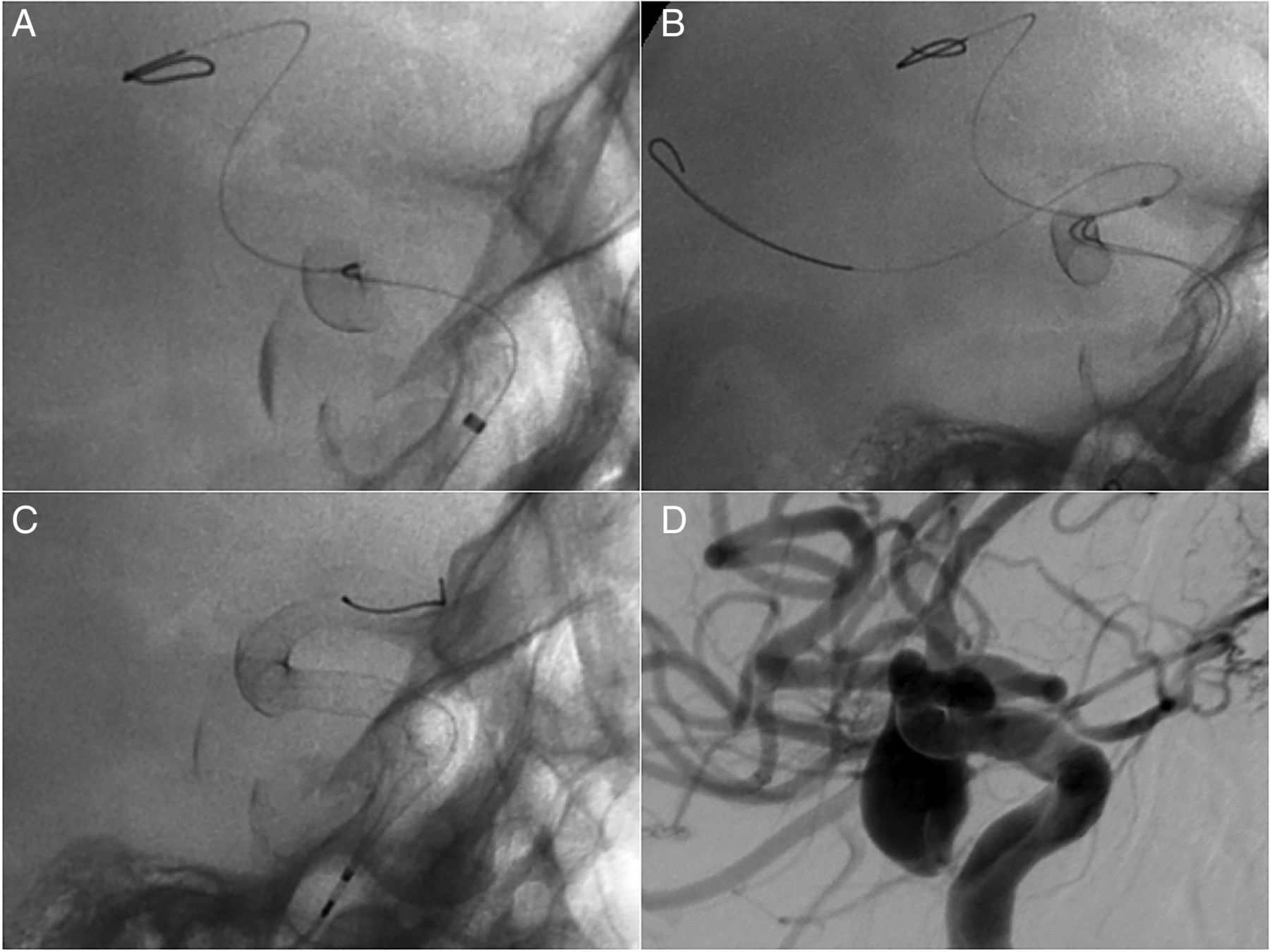
Illustrations and fluoroscopic images. Lateral view. (A, B) A J shaped Synchro-2 microwire was advanced distally through the stent until M2. The balloon was deflated and then navigated through the pipeline embolization device (PED) over the wire. (C–E) The balloon was inflated again inside the PED, and the balloon catheter was retracted until realignment in the aneurysm neck. (F) The balloon was deflated keeping the loop of the Synchro-2 microwire.
The balloon was inflated again inside the PED and the balloon catheter was retracted until realignment in the aneurysm neck. Once the balloon was deflated, the loop of the Synchro-2 microwire was eliminated (figure 3C, D).
The balloon was then removed, keeping the Synchro-2 microwire in place (figure 4A) until a Marksmann microcatheter was navigated distally in the MCA through the stent (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fluoroscopic images. Lateral view. (A) The balloon has been removed and the loop of the Synchro-2 microwire was eliminated. (B) A Marksmann microcatheter was navigated distally in the middle cerebral artery through the stent. (C, D) Two additional telescoped pipeline Flex devices were deployed for artery reconstruction.
We were able to complete the embolization with placement of two additional telescoped pipeline Flex devices, which provided complete coverage of the aneurysm and artery reconstruction (figure 4C, D).
Outcome and follow-up
The patient had an uneventful postoperative course and was discharge home on postoperative day 3.
Discussion
The use of the PED has been shown to be effective for the treatment of cerebral aneurysms.1 As is the case with any endovascular treatment, there are a number of potential complications that are directly related to deployment of the device.2–7 If managed effectively, these complications may remain clinically silent; however, if they are not dealt with appropriately, disastrous complications may result.5
Depending on the proximal and distal purchase of the PED, prolapse of one end of the device into a large aneurysm may occur with any subsequent manipulation of the device, or even spontaneously.2 ,6
Significant mismatch in luminal diameter between the inflow vessel and the outflow vessel or excessive dragging–stretching of the PED have been related to ‘watermelon seed’ or ‘accordion’ effects, respectively, resulting in stent migration.6
Moreover, the operator must have in mind that until scarring and endothelization of the device occurs, the accordion-like behavior of the device and its elasticity raises the risk of movement of the PED inside the vessel, either by migration or retraction.5
In the presented case, we believe that there were two causes of the prolapse: a short proximal landing zone and too much unsheathing during delivery, all resulting in an ‘accordion effect’.
Different techniques have been described to solve PED migration, including open surgery,7 snare assisted rescue,2 ,3 balloon anchoring for distal end herniation,8 or stent-in-stent techniques.4 While distal end PED migration allows more endovascular rescue options, a proximal end migration requires more complex maneuvers to regain distal access through the stent, such as the presented case.2–4 We felt that reducing the loop of the microwire would not provide enough support to realign the device, considering the acute angle of the herniated PED. Although anchoring techniques, where the balloon is inflated distal to the stent, have been described,8 we preferred to inflate the balloon gently in a proximal ‘free segment’ than in the MCA or ICA, avoiding the potential risk of endothelial damage during traction maneuvers.
We found two critical steps that should be kept in mind during balloon inflation in the described position: first, the risk of proximal migration of the distal end of the stent, and second, the risk of aneurysm perforation. In this sense, compliance balloons with a short distal tip and slight retraction during inflation could minimize these potential complications. Because of the inherent risk, this technique should be reserved for large/giant aneurysms.
In our case, the main limitation was the intra-aneurysmal position of the proximal end of the PED at the inflow entrance. Once it became apparent that an additional PED would not be successfully placed without manipulating the existing PED, the decision was made to attempt realignment of the PED using a balloon anchoring technique, keeping vessel deconstruction in mind as a backup plan. This maneuver ultimately proved to be successful, and allowed for placement of a subsequent PED and completion of the embolization.
Avoiding complications in the first place is, of course, preferable to successfully managing them once they occur. The use of a longer PED or telescoping another device might have been helpful to avoid this complication.
This represents a useful salvage technique and should be considered when encountering this potential complication.
Key messages
Accurate stent sizing and adequate apposition to the vessel wall may minimize the occurrence of migration phenomenon.
Significant mismatch in luminal diameter or excessive dragging–stretching of the pipeline embolization device have been related to ‘watermelon seed’ or ‘accordion’ effects.
The use of a longer flow diverter or telescoping another device might have been helpful to avoid device prolapse into the aneurysm.
References
Footnotes
Republished with permission from BMJ Case Reports Published 23 March 2016; doi:10.1136/bcr-2016-012263
Contributors Study concept and design, analysis and interpretation of the data, drafting of the manuscript, critical revision of the manuscript for important intellectual content, administrative, technical, and material support, and study supervision: MM-G. Illustrations: AH. Acquisition of the data: all authors.
Competing interests MM-G is a consultant for Medtronic Neurovascular and Proctor for the pipeline embolization device.
Patient consent Not obtained.
Ethics approval The study was approved by the institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.