Article Text

Abstract
Purpose To compare the safety and efficiency of stent assisted coiling (SAC) with non-SAC for the management of ruptured intracranial aneurysms.
Methods A meta-analysis that compared SAC with coiling alone and balloon assisted coiling was conducted by database searching. The primary outcomes of this study were immediate occlusion and progressive thrombosis rate, overall perioperative complication rate, and angiographic recurrence. Secondary outcomes included mortality at discharge, hemorrhagic and ischemic complications, and favorable clinical outcome at discharge and at follow-up.
Results Eight retrospective cohort studies with 1408 ruptured intracranial aneurysms (SAC=499; non-SAC=909) were included. The SAC group tended to show a lower immediate complete occlusion rate than the non-SAC group (54.3% vs 64.2%; RR 0.90; 95% CI 0.83 to 0.99; I2=17.4%) and achieved a significantly higher progressive complete rate at follow-up (73.4% vs 61.0%; RR 1.30; 95% CI 1.16 to 1.46; I2=40.5%) and a lower recurrence rate (4.8% vs 16.6%; RR 0.28; 95% CI 0.16 to 0.50; I2=0.0%). With respect to safety concerns, overall perioperative complications in the SAC group were significantly higher (20.2% vs 13.1%; RR 1.70; 95% CI 1.36 to 2.11; I2=0.0%). However, no significant difference was found for mortality rate at discharge (6.3% vs 6.2%; RR 1.29; 95% CI 0.86 to 1.94; I2=0.0%), or favorable clinical outcome rate at discharge (73.4% vs 74.2%; RR 0.95; 95% CI 0.88 to 1.02; I2=12.1%) and at follow-up (85.6% vs 87.9%; RR 0.98; 95% CI 0.93 to 1.02; I2=0.0%; P=0.338).
Conclusions SAC has a lower recurrence rate than non-SAC. Nevertheless, further validation by well designed prospective studies is warranted for determining whether stents improve angiographic outcome without an increased complication rate or unfavorable clinical outcome.
- aneurysm
- balloon
- stent
- subarachnoid
- hemorrhage
Statistics from Altmetric.com
Introduction
Stent assisted coiling (SAC) is an endovascular treatment option for intracranial aneurysms. Several studies have demonstrated that the long term effectiveness of SAC is significantly better than that of balloon assisted coiling (BAC) or coiling only, and SAC achieved better complete occlusion rates and lower recurrence rates at follow-up.1 2 The application of stents in acutely ruptured intracranial aneurysms has also been proved to be feasible and safe.3 4 However, placement of stents in patients with acutely ruptured intracranial aneurysms still remains controversial because of the concern for thromboembolic complications, including thrombus formation related to the stent and hemorrhagic complications because of the use of antiplatelet medication.5 6
Complications of SAC in acutely ruptured aneurysms are substantially attributable to periprocedural antiplatelet medication.7 Hemorrhagic events may increase because of excessive antiplatelet therapy and thrombotic events may increase because of inadequate antiplatelet therapy. However, previous studies have provided evidence that application of stents and contemporary antiplatelet therapy was feasible in managing acutely ruptured intracranial aneurysms.4 8
To date, there have been no studies of endovascular treatment of ruptured intracranial aneurysms with or without stents. In addition, most of the existing literature comparing SAC and non-SAC did not focus on acutely ruptured aneurysms but included both ruptured and unruptured aneurysms.9–12 Hence this meta-analysis was performed to compare the safety and efficacy of SAC and and non-SAC for ruptured intracranial aneurysms.
Methods and materials
Literature search
This meta-analysis was performed according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines and recommendations. Online database searches included Pubmed, Ovid Medline, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, ACP Journal Club, and Database of Abstracts of Reviews of Effects (DARE), from their dates of inception to August 2018.
To achieve maximum sensitivity of the search strategy and identify all studies, we combined the following terms: ‘intracranial’, ‘cerebral’, ‘carotid’, ‘basilar’, ‘aneurysms’, ‘stent’, ‘balloon’, or ‘‘coil’, as either keywords or MeSH terms. In addition, the names of merchandised stent devices, such as ‘Neuroform’, ‘Enterprise’, ‘Leo stent’, ‘Lvis stent’, and ‘Solitaire’, were used as text words to extract relevant studies. Reference lists of included studies were manually searched. All identified articles were systematically assessed using the inclusion and exclusion criteria.
Inclusion and exclusion criteria
Inclusion criteria were: (1) studies compared SAC versus coiling alone or BAC approaches (non-SAC), (2) studies reported patients with definite intracranial ruptured aneurysms, verified by CT scan and CT angiography/MRI/DSA, (3) studies reported occlusion rate, complications, or clinical outcomes, and (4) studies included at least 10 patients in each group. Exclusion criteria were as follows: (1) reported patients with dissecting, bacterial, mycotic, and fenestrated aneurysms, (2) reported patients who received treatment other than SAC or coiling alone or BAC, and (3) had insufficient outcome data for comparison between the two cohorts. In addition, unpublished articles, reviews, meta-analyses, comments, letters, pilot studies, conference only studies, case reports, abstract only studies, and non-English language studies were excluded. All analyses were based on previous published studies, and thus no ethical approval or patient consent was required.
Selection and data extraction
Database search and review were independently performed by two junior physicians (XZ and QZ), with disagreements settled by the senior physicians (JL and QH). All data were extracted from article texts, tables, and figures. The primary outcomes were immediate occlusion and progressive thrombosis rate, overall perioperative complication rate, and angiographic recurrence. Secondary outcomes included mortality at discharge, hemorrhagic and ischemic complications, and favorable clinical outcome at discharge and at follow-up. Favorable clinical outcome was defined as a modified Rankin Scale score of 0–2 or Glasgow Outcome Scale score of 4– 5.
Quality assessment and statistical analysis
The Newcastle–Ottawa Scale was used to evaluate the bias of cohort studies. Meta-analysis was performed using the software package Stata 13. Dichotomous variables were presented with risk ratios (RR; SAC vs non-SAC) with 95% CI. Statistical heterogeneity was evaluated using I2. A random effect model was used if I2 >50%, otherwise a fixed effect model was used. Statistical significance was set at P=0.05.
Results
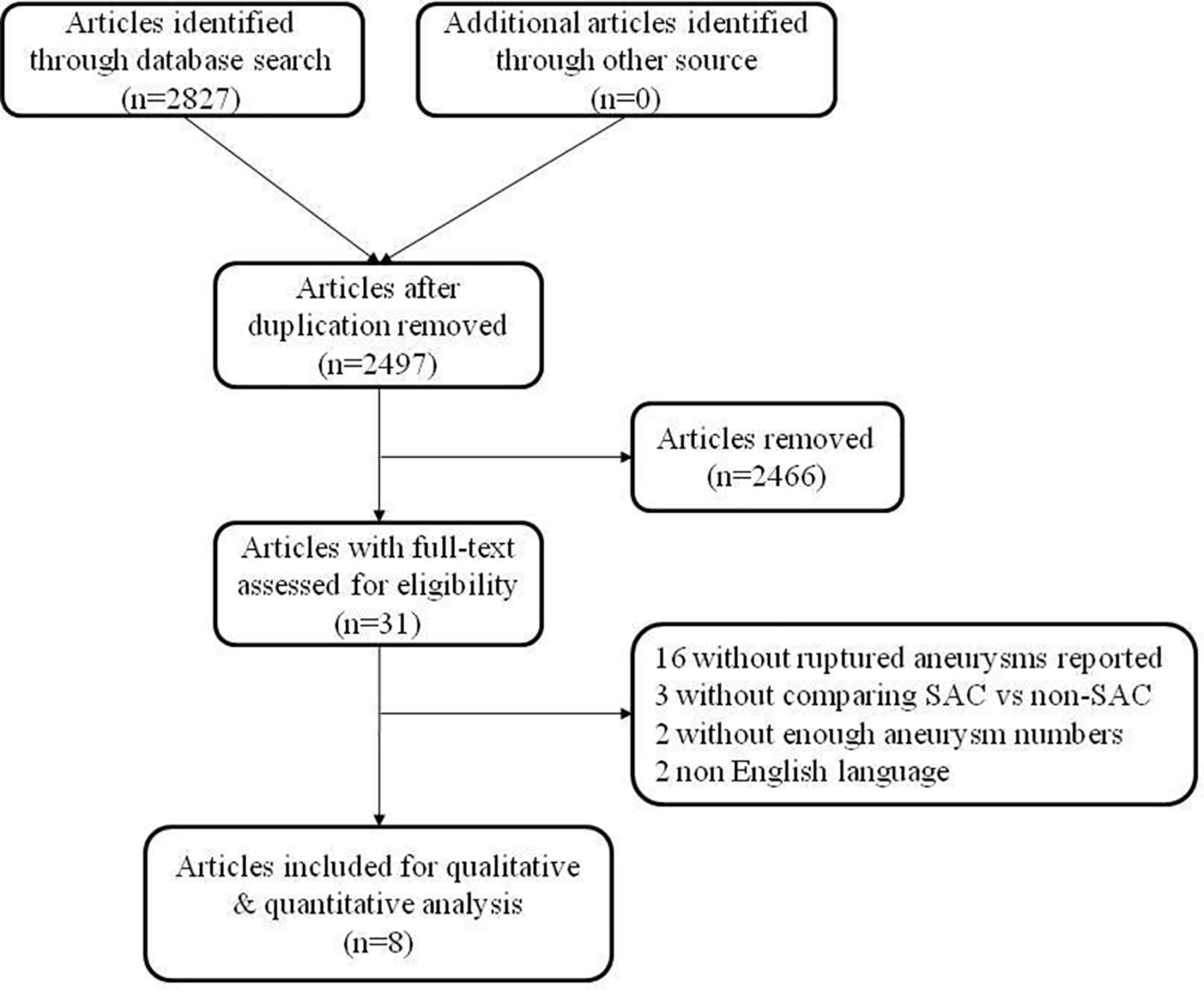
A total of 2827 articles were retrieved after the first round search strategy, 2796 of which were excluded by title or abstract screening. Of the 31 articles left, full texts were accessed, and 8 articles13–20 fulfilling the inclusion criteria were included. The search selection process is illustrated in figure 1.

Flowchart of study selection. SAC, stent assisted coiling.
Baseline characteristics of included studies
All of the eight included articles were retrospective cohort studies comparing SAC with non-SAC for the treatment of ruptured intracranial aneurysms.13–20 Detailed baseline characteristics of the included studies are summarized in tables 1 and 2. In total, in these studies, 554 ruptured aneurysms underwent SAC and 1303 ruptured aneurysms underwent coiling without stent placement. Mean age of patients receiving SAC ranged from 53.7 to 65.6 years compared with 53.9 to 56.5 years for the non-SAC group. Aneurysm size in the SAC group ranged from 5.1 to 8.4 mm, while in the non-SAC group it ranged from 5.0 to 6.7 mm. The percentage of women was 39.1– 86.4% in the SAC group and 48.1–80.0% in the non-SAC group. Further detailed information and the risk bias of the included studies using the Newcastle–Ottawa Scale are shown in table 1.
Baseline characteristics and design of the included studies
Comparison between stent assisted coiling and non-stent assisted coiling for the treatment of ruptured intracranial aneurysms
Analysis of primary outcomes
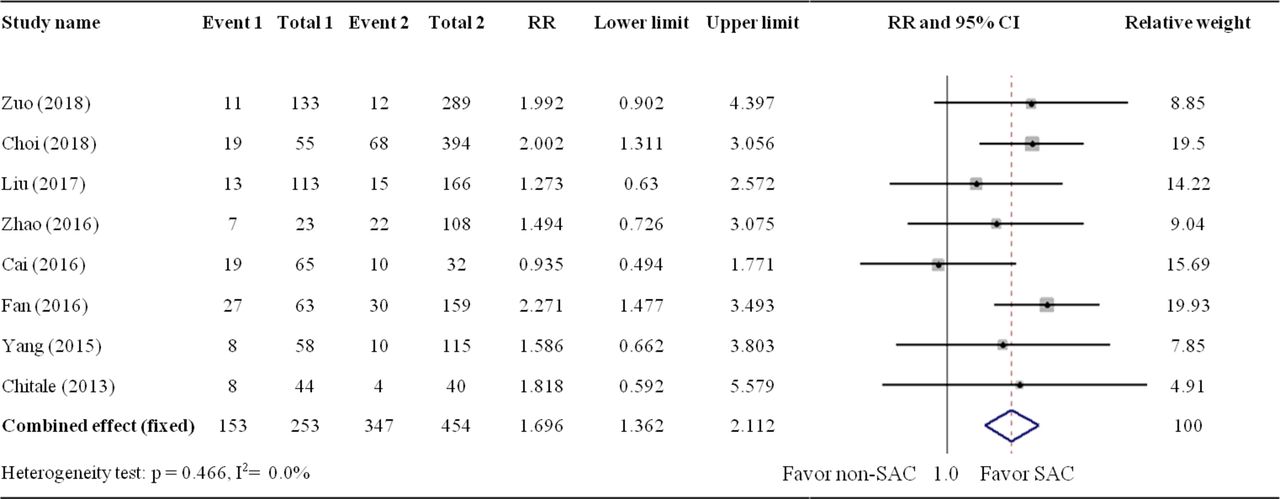
Seven studies13 16–21 with a total number of 1408 ruptured intracranial aneurysms (SAC=499; non-SAC=909) reported the immediate occlusion rate after endovascular treatment. In a fixed effect model, the immediate complete occlusion rate in the SAC group was significantly lower than that in the non-SAC group (287/554 vs 584/1303; 54.3% vs 64.2%; RR 0.90; 95% CI 0.83 to 0.99; I2=17.4%; P=0.297) (figure 2). In contrast with the immediate occlusion rate, the SAC group showed significant angiographic improvement during follow-up compared with the non-SAC group (174/237 vs 228/374; 73.4% vs 61.0%; RR 1.30; 95% CI 1.16 to 1.46; I2=40.5%; P=0.169)13 16–18 and a significantly lower rate of recurrence at follow-up (14/290 vs 74/447; 4.8% vs 16.6%; RR 0.28; 95% CI 0.16 to 0.50; I2=0.0%; P=0.644) (figures 3 and 4). All eight studies reported overall perioperative complications. In a fixed effect model, the overall perioperative complication rate in the SAC group was significantly higher than that in the non-SAC group (112/554 vs 171/1303; 20.2% vs 13.1%; RR 1.70; 95% CI 1.36 to 2.11; I2=0.0%; P=0.466) (figure 5).
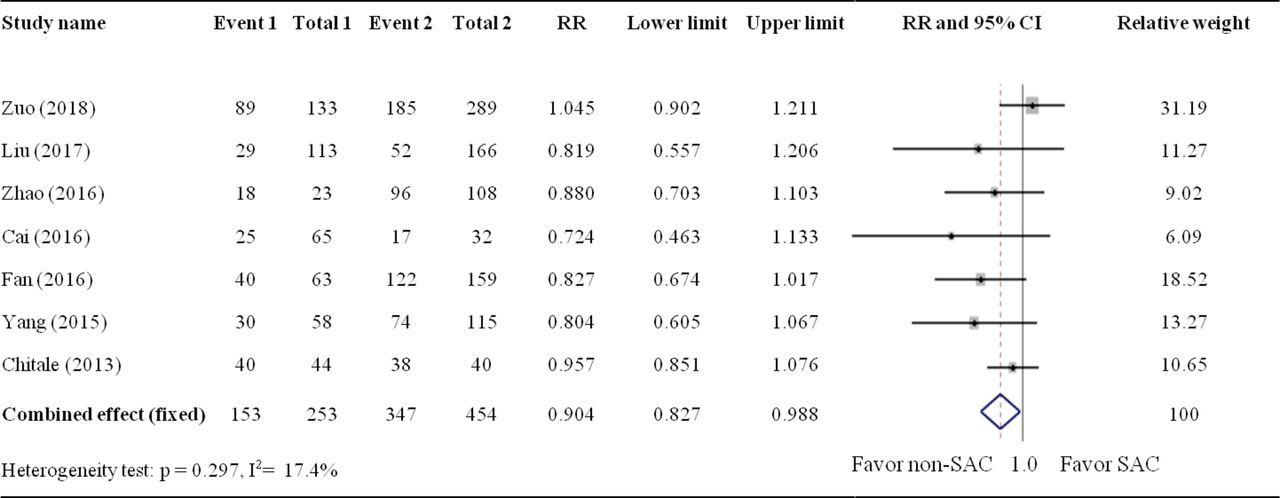
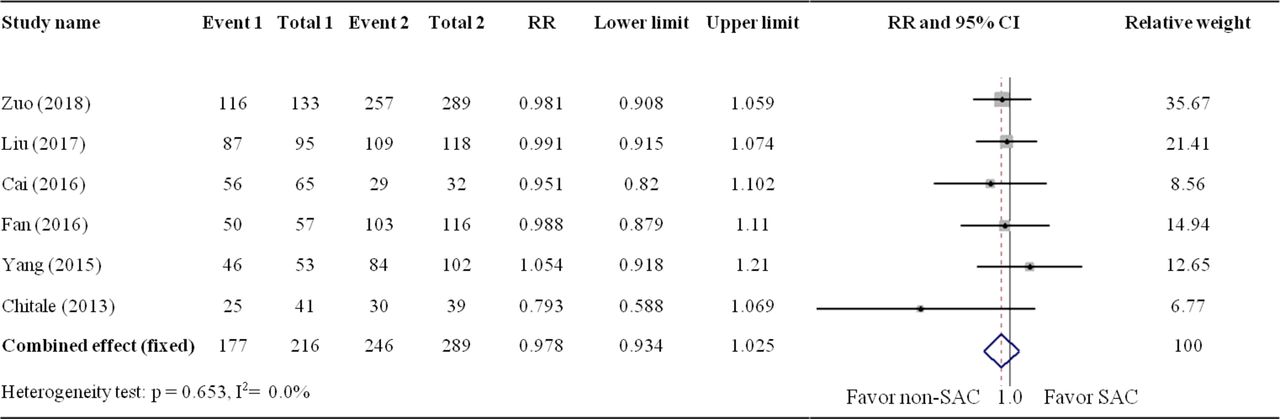
Comparison of immediate complete occlusion rate after the procedure between the stent assisted coiling (SAC) and non-SAC groups.
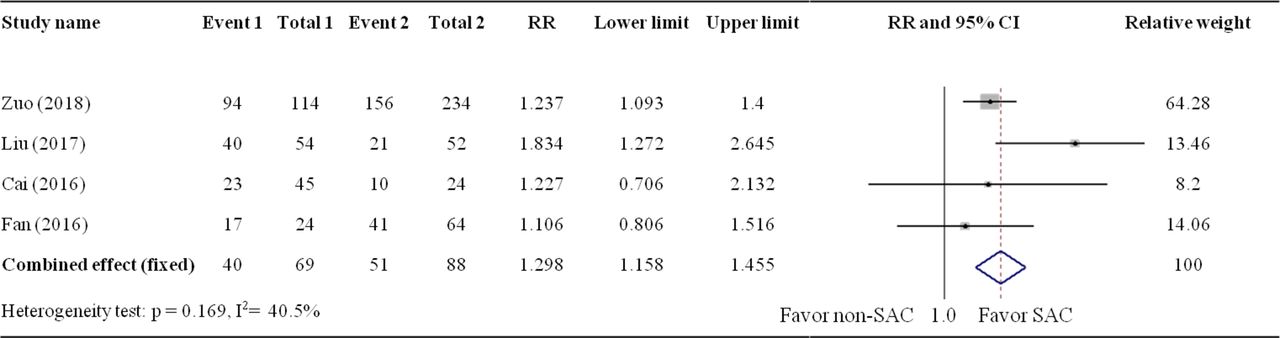
Comparison of complete occlusion rate at follow-up between the stent assisted coiling (SAC) and non-SAC groups.
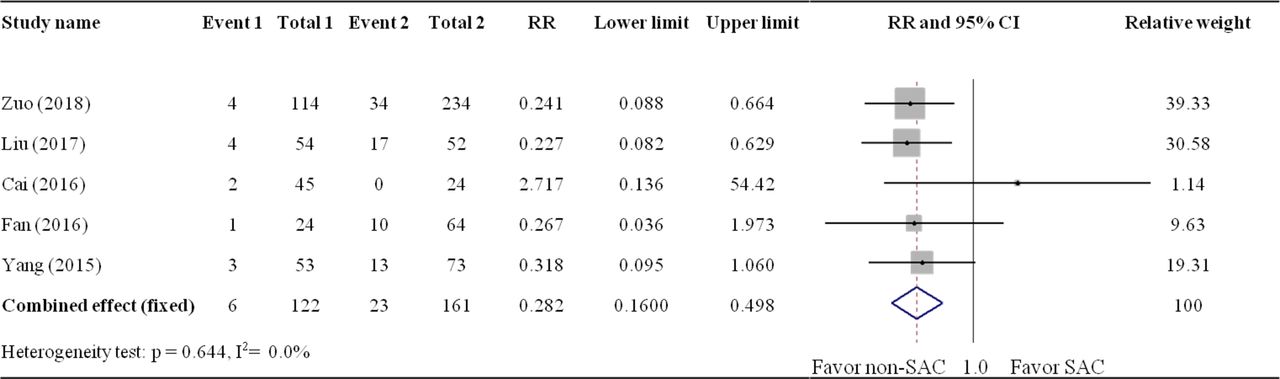
Comparison of recurrence rate at follow-up between the stent assisted coiling (SAC) and non-SAC groups.

Comparison of overall perioperative complication rate between the stent assisted coiling (SAC) and non-SAC groups.
Analysis of secondary outcomes
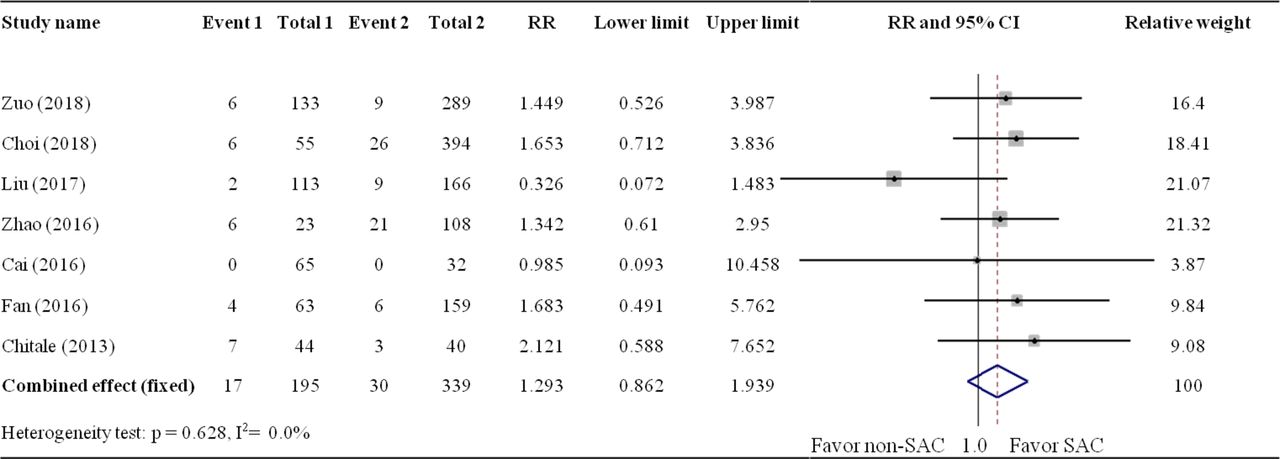
All eight studies reported both hemorrhagic and ischemic complication rates. In a fixed effect model, the hemorrhagic and ischemic complication rates in the SAC group were higher than those in the non-SAC group (41/554 vs 60/1303; 7.4% vs 4.6%; RR 1.60; 95% CI 1.09 to 2.35; I2=14.2%; P=0.319; and 68/554 vs 109/1303; 12.3% vs 8.4%; RR 1.75; 95% CI 1.30 to 2.36; I2=0.0%; P=0.511, respectively) (figures 6 and 7). Specifically, no significant difference in aneurysmal intraoperative rupture rate in either group was observed (23/496 vs 31/1188; 4.6% vs 2.6%; RR 1.32; 95% CI 0.79 to 2.22; I2=10.3%; P=0.350) (figure 8). In addition, seven studies13–18 20 reported periprocedural mortality rate. The mortality rate in both groups was similar (31/496 vs 74/1188; 6.3% vs 6.2%; RR 1.29; 95% CI 0.86 to 1.94; I2=0.0%; P=0.628) (Figure 9).
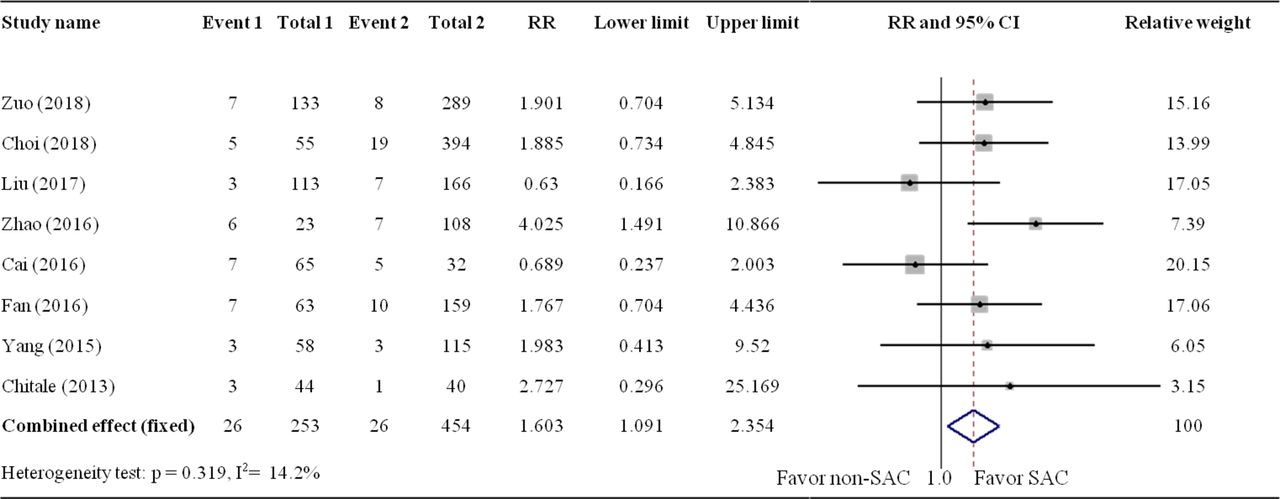
Comparison of hemorrhagic events between the stent assisted coiling (SAC) and non-SAC groups.

Comparison of ischemic events between the stent assisted coiling (SAC) and non-SAC groups.

Comparison of intraprocedural rupture rate between the stent assisted coiling (SAC) and non-SAC groups.

Comparison of perioperative mortality at discharge between the stent assisted coiling (SAC) and non-SAC groups.
Six studies with 1405 aneurysms reported a favorable clinical outcome at discharge.13–16 18 20 The favorable clinical outcome rate of the SAC group (281/383, 73.4%) was similar to that of the non-SAC group (758/1022, 74.2%) (RR 0.95; 95% CI 0.88 to 1.02; I2=12.1%; P=0.338) (Figure 10). A progressively increased favorable clinical outcome rate was observed in both groups, as reported in six studies.13 14 16–19 The follow-up favorable clinical outcome rate for the SAC group (380/444, 85.6%) was similar to that of the non-SAC group (612/696, 87.9%) (RR 0.95; 95% CI 0.88 to 1.02; I2=12.1%; P=0.338) (Figure 11).
Comparison of favorable clinical outcome at discharge between the stent assisted coiling (SAC) and non-SAC groups.

Comparison of favorable clinical outcome at follow up between the stent assisted coiling (SAC) and non-SAC groups.
Sensitivity analysis and publication bias
Funnel plot analysis on immediate occlusion rate is shown in Figure 12, which indicated the very small publication bias. Similar results were also obtained for all of the other outcomes.
Discussion
This study is the first meta-analysis comparing SAC with non-SAC in the management of ruptured intracranial aneurysms. The results showed that SAC significantly reduced the recurrence rate and improved aneurysm progressive occlusion rate compared with non-SAC. However, the overall periprocedural complication rate was significantly higher in the SAC group, for both hemorrhagic and ischemic complications. Moreover, no significant difference in mortality at discharge, or favorable clinical outcome rate at discharge and at follow-up was found between the two groups.
The results of this meta-analysis are consistent with previous studies. Phan et al 22 performed a meta-analysis comparing SAC with coiling alone in the treatment of intracranial aneurysms. The immediate occlusion rates for the two groups were 57.7% and 48.7%, respectively, with no significant difference (RR=1.01; 0.68–1.49). However, the progressive thrombosis rate was significantly higher in the SAC compared with the coiling only group (29.9% vs 17.5%; RR=2.71; 1.95–3.75). Additionally, the recurrence rate was significantly lower in the SAC group (12.7% vs 27.9%; RR=0.43; 0.28–0.66). As reported by Piotin et al,9 stents were associated with a significant decrease in angiographic recurrences (17/114, 14.9% vs 259/774, 33.5%) in the treatment of intracranial aneurysms, but they were associated with more lethal complications compared with coiling without stents (10/216, 4.6% vs 13/1109, 1.2%).
Similarly, for ruptured intracranial aneurysms, our study found that aneurysms treated with SAC tended to progressively advance through thrombosis towards a more complete occlusion at follow-up compared with coiling only or BAC techniques. The angiographic advantage of stent placement was not predominant at immediate angiography. Even the placement of stents tends to reduce the immediate occlusion rate; it promotes progressive thrombosis within the aneurysmal sac by a scaffold effect, which also lowers the recurrence rate and may further reduce the retreatment rate and medical costs.9 23
The balloon remodeling technique provided a contemporary scaffold effect that prevented coil protrusion and was associated with an improved occlusion rate after endovascular therapy in previous studies.24 Wang et al 25 performed a meta-analysis comparing BAC and SAC in intracranial aneurysms. SAC achieved a better complete occlusion rate of aneurysms at 6 months or later after the procedure, with comparable intraprocedural complication and retreatment rates. Lawson et al 23 compared 37 stented and 72 non-stented aneurysms and found that stent coiled aneurysms were 18.5 times more likely to achieve complete occlusion compared with non-stented aneurysms, with a significantly lower rate of recanalization.
Dual antiplatelet therapy for patients with subarachnoid hemorrhage (SAH) treated with stents is concerning because of the risk of hemorrhagic events. Further detailed analysis of patients in the International Subarachnoid Aneurysm Trial (ISAT)26 found that standard antiplatelet therapy did not affect the outcome at discharge or at the 1 year follow-up in patients with SAH. Shimamura et al 27 found that preprocedural antiplatelet medication did not affect the outcome of 35 consecutive SAH patients. In addition, Kato et al 28 investigated the influence of previous antiplatelet usage before stroke on the outcome of SAH patients with age. They enrolled 5344 patients with SAH in a multicenter study, and found that the use of antiplatelet agents significantly improved outcome in patients <60 years of age (P=0.04). In contrast, in the older age group (≥60 years), the use of antiplatelet agents tended to worsen outcome; patients aged 70–79 years who had used these agents had a significantly worse outcome compared with those who had not (P=0.03).
Safety evaluation is crucial for determining the therapeutic approach for the management of ruptured intracranial aneurysms. As previously reported, use of stents was related to higher complication and mortality rates compared with coiling alone and BAC. Choi et al 15 found that stent usage was not a risk factor for unfavorable clinical outcomes for acutely ruptured intracranial aneurysms.8 In this review, despite the fact that the complication rate of the SAC group was higher than that of the non-SAC group, no significant difference in mortality rate at discharge was found between the two groups. The favorable clinical outcome rate at discharge and at follow-up was also similar between the two groups. For a definitive decision on whether stent deployment would increase mortality or unfavorable clinical outcome rate for the management of ruptured aneurysms, better controlled clinical trials are still needed.
As complex aneurysms are associated with a higher risk of recurrence and complications, it would not be surprising if the outcome of SAC was poorer or similar compared with coiling alone.22 It might be expected that SAC provides an alternative for complex aneurysms with comparable angiographic outcome. For wide necked ruptured intracranial aneurysms, Tahtinenet al 4 found that 69% of patients treated with stent assistance had a better clinical outcome compared with conventional coiling. The authors also suggested that SAC could be an alternative in treating SAH with complex morphology.8
In previous studies, stent placement has been reported and proved to be feasible and safe for acutely ruptured intracranial aneurysms without focusing on morphology and location.3 4 For ruptured aneurysms that are amenable to BAC or coiling alone, SAC might also be safe and more effective.
More recently, flow diverters, including Pipeline, Silk, and Tubridge, provided a more robust hemodynamic effect compared with conventional stents. According to previous studies, flow diverters tend to achieve improved occlusion rates at immediate and follow-up angiography.29 30 However, the periprocedural complication rate seemed to be higher, especially thromboembolic complications, with comparable clinical outcomes. By improving antiplatelet therapy for acutely ruptured intracranial aneurysms, the thromboembolic and hemorrhagic complication rate might be reduced.
The baseline characteristics of all included studies were similar. However, the results of this meta-analysis should be interpreted with caution as all data were pooled from observational studies while no randomized controlled studies were available. Overall, large prospective multicenter randomized clinical trials with better control of aneurysm heterogeneity would help to provide definitive information on the best therapeutic approach for aneurysms treatment.
Conclusion
SAC has a lower rate of recurrence and immediate complete occlusion, similar rate of favorable clinical outcome and mortality, and a higher rate of progressive complete occlusion compared with coiling alone and BAC. However, SAC was associated with a higher rate of periprocedural complications. The question remains of whether SAC should be systematically used for ruptured intracranial aneurysms regardless of morphology or clinical status. Further randomized controlled trials are warranted to answer this question.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of immediate complete occlusion rate.
Supplementary file 1
References
Footnotes
XZ, QZ and HT contributed equally.
Contributors Conception and design, acquisition of the data, and analysis and Interpretation of the data: XZ, QZ, and HT. Drafting the article: XZ, QZ , andJL. Critically revising the article: XZ, QZ, QH, and JL. All authors reviewed the submitted version of the manuscript and approved the final version of the manuscript. Statistical analysis: XZ, QZ, and HT. Study supervision: QH and JL.
Funding This work was supported by the National Key R&D Program of China, grant No 2016YFC1300700, and National Natural Science Foundation of China, grant No 81701136.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.