Article Text

Abstract
Introduction Technical improvements to enhance distal occlusion thrombectomy are desirable. We describe the blind catheter exchange technique and report the pinning technique with small devices (‘mini-pinning’) for distal occlusions.
Methods A retrospective review of a prospective database from January 2015 to August 2018 was performed for cases of distal occlusion in which the ‘blind exchange/mini-pinning’ (BEMP) techniques were used. The technique involves the deployment of a 3 mm Trevo retriever followed by microcatheter removal and blind advancement of a 3MAX aspiration catheter over the bare retriever delivery wire (‘blind exchange’) until clot contact under aspiration. The retriever is subsequently partially recaptured in order to ‘cork’ the thrombus (‘mini-pinning’) and the system pulled as a unit. Patients with distal occlusions treated with BEMP and standard techniques (either 3 mm Trevo or 3MAX) were compared.
Results Twenty-five vessels were treated in 22 patients. The majority of patients had isolated distal occlusions predominantly in the distal middle cerebral artery (MCA) segments, half of which involved the superior division. The comparison between BEMP (n=25 vessels) and standard techniques (n=144 vessels) revealed balanced groups. One of the highlighted differences was the more distal MCA occlusions among those who underwent BEMP (M3 occlusions 52% vs 22%; p=0.001). Otherwise, the vessel, segments, divisions and luminal diameter were comparable. There was a higher rate of first-pass modified Thrombolysis in Cerebral Infarction 2b–3 (80% vs 56%; p=0.03) and a trend towards higher rates of first-pass full reperfusion (60% vs 40%; p=0.07) with BEMP compared with standard techniques. Final reperfusion and clinical outcomes were comparable.
Conclusion BEMP appears to be a safe and effective technique for the treatment of distal occlusions. Additional studies are warranted.
- stroke
- thrombectomy
- stent
Statistics from Altmetric.com
Introduction
Distal cerebral occlusions can represent a significant proportion of ischemic stroke cases with visible occlusions on non-invasive vascular imaging.1 These occlusions can involve eloquent branches and lead to significant neurological deficits. The limited data on thrombectomy for distal occlusions point towards feasibility and safety.2 However, unsuccessful reperfusion has been described in a significant percentage of cases (up to 25–26% Thrombolysis in Cerebral Infarction (TICI) 0–2a).3 4 Moreover, complete reperfusion may be only achieved in a small fraction (<30%) of cases.5 Therefore, improvement in techniques is important to enhance reperfusion rates and, ultimately, to achieve better clinical outcomes. We describe the blind catheter exchange technique using the stent-retriever delivery wire to advance the thromboaspiration catheter and report the pinning technique with small devices (‘mini-pinning’) for thrombectomy of distal occlusions, which may improve procedural performance.
Methods
This is a retrospective review of a prospectively collected thrombectomy database from January 2014 to August 2018 for consecutive cases of distal occlusion in which the ‘blind exchange/mini-pinning’ (BEMP) techniques were used. This study was approved by the local Institutional Review Board.
Description of blind exchange with mini-pinning technique
A 3×20 mm Trevo retriever (Stryker Neurovascular, Freemont, California, USA) is deployed via a Trevo 14 (0.017 inch) microcatheter followed by microcatheter removal and blind advancement of the 3MAX aspiration catheter (Penumbra, Alameda, California, USA) over the bare retriever delivery wire (‘blind exchange’) under fluoroscopy until clot contact. The retriever is then partially recaptured in order to ‘cork’ the thrombus into the aspiration catheter (‘mini-pinning’) while aspirating. The retriever and aspiration catheters are subsequently pulled as a unit in order to retrieve the clot (figure 1). BEMP was done as a primary maneuver (figure 2) or used as an adjunct when the position of the 3 mm retriever was perceived to be poor, with minimal stent-retriever purchase past the thrombus (figure 3) and expected lower chances of clot retrieval. This technique was used occasionally during the study period due to the additional costs related to the use of an additional thrombectomy device.

Mini-pinning (3 mm Trevo and 3MAX) with corking of the thrombus.

Blind exchange and mini-pinning for a long clot. (A) Lateral angiogram showing an M3 occlusion (arrow: proximal end of clot). (B) 3 mm retriever in place demonstrating a long clot (arrowhead: distal end of retriever). (C) 0.017 inch microcatheter in place after deployment. (D) 3MAX advanced into the face of the clot (black arrowhead) over the bare retriever delivery wire. (E) Final angiogram with successful reperfusion.
{kind=link}
{kind=link}
{kind=link}
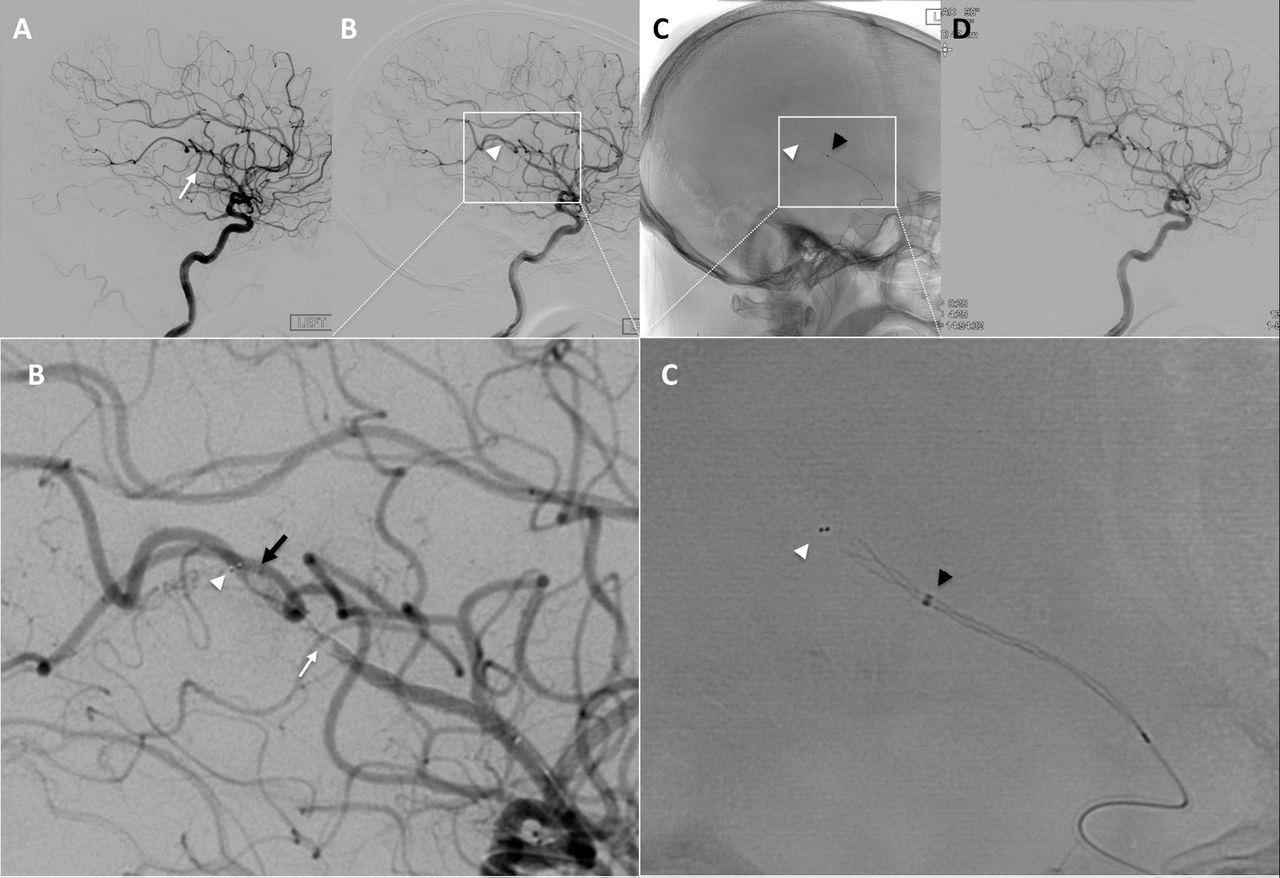
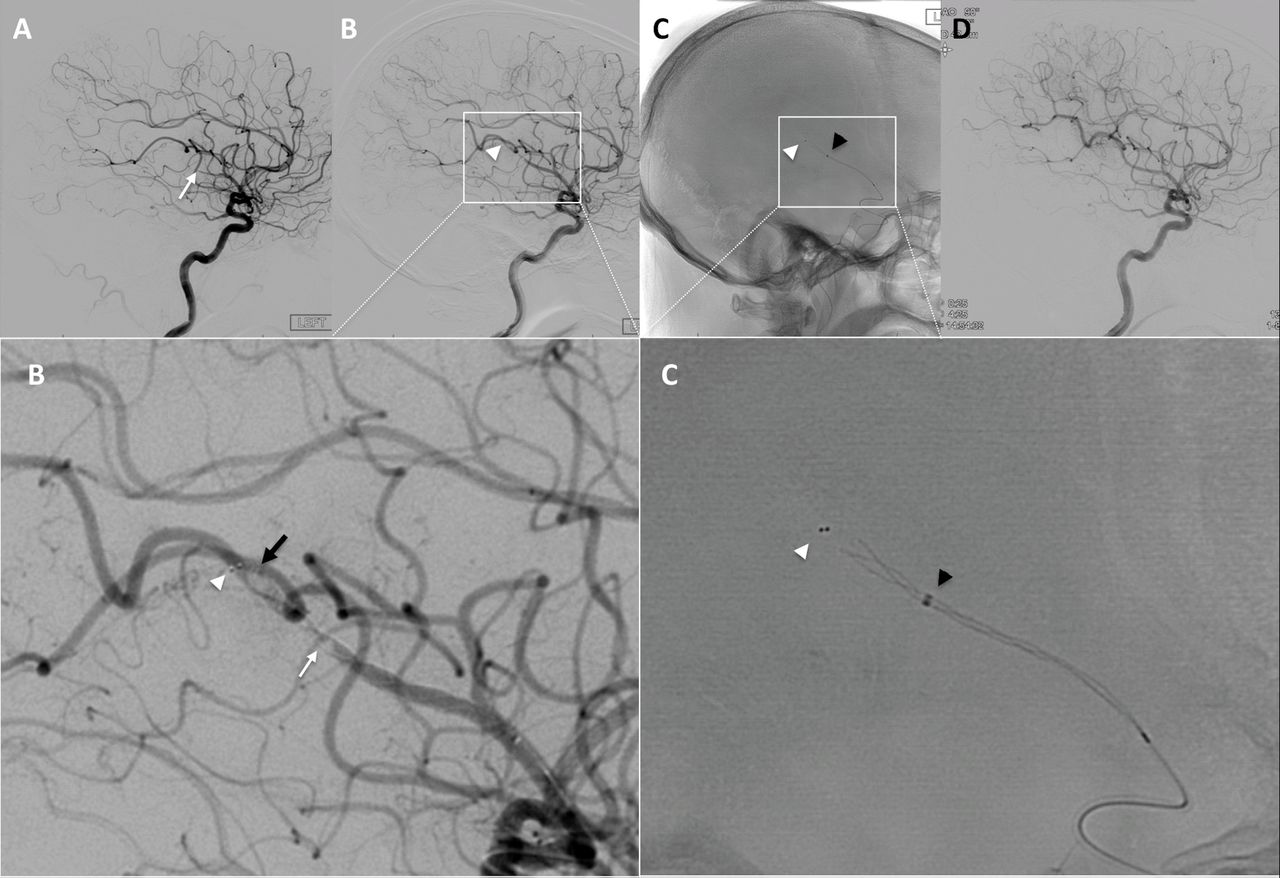
Blind exchange and mini-pinning due to insufficient retriever purchase past the thrombus. (A) Lateral angiogram showing an M3 occlusion (arrow: proximal end of clot). (B) 3 mm retriever in place demonstrating a long clot (white arrow: proximal end of clot; black arrow: distal end of clot; arrowhead: distal end of retriever) with insufficient purchase of retriever past the clot; 0.017 inch microcatheter is observed. (C) 3MAX advanced into the clot (black arrowhead). (D) Final Angiogram
Comparative analysis against standard techniques
We analyzed individual patient-level data comparing BEMP with our previously published experience using standard techniques2 (either 3 mm Trevo retriever or 3MAX thromboaspiration) for patients with distal occlusions. In brief, we included all consecutive patients within the study period treated with a 3 mm Trevo alone, 3MAX alone, or a combination of both for distal arterial occlusions involving the middle cerebral artery (MCA M2, M3 segments), anterior cerebral artery (ACA A1, A2, A3), or posterior cerebral artery (PCA P1, P2). We excluded cases with vessel diameter ≥2 mm. A fellowship-trained neurointerventionist reviewed all procedural reports/modified treatment in Cerebral Infarction (mTICI) scores and analyzed all angiographic images to define per-pass reperfusion grades.6 Baseline characteristics, occlusion site, and reperfusion rates among the techniques were analyzed. The first pass with each device was considered for determination of reperfusion rates.
Definitions
The occlusion site was defined according to the following criteria. ACA A1: from origin to the anterior communicating artery; A2: from the anterior communicating artery to the callosomarginal takeoff; A3: pericallosal or callosomarginal. MCA mid M2: the distal half (midway or distal) of the vertical segment of first MCA branch from the MCA limen insulae and circular sulcus on anterior–posterior angiography7; distal M2: immediately proximal to or at the M2–3 junction (including occlusions at the circular sulcus); M3: the opercular segment between the circular sulcus of the insula and the cortical surface.8 Angiograms were evaluated for the presence of a distal occlusion (mTICI 0–1) and classified according to their clinical scenario: isolated distal occlusion; distal occlusion in the setting of a concomitant larger vessel/proximal occlusion; emboli to the same or new territory after thrombectomy of a proximal occlusion. The diameter of the vessel was calculated just proximal and distal to the occlusion site via iSite PACS on cine images from fluoroscopic runs obtained on a Phillips Allura biplane machine (Andover, Massachusetts, USA) in all cases.
Outcomes
The primary outcome was the first-pass effect (FPE), defined as mTICI 3 reperfusion after first pass, while the modified first-pass effect (mFPE) was considered as mTICI 2b–3 after first pass. We compared the BEMP technique against the standard technique (use of either a 3 mm Trevo Retriever or 3MAX alone). Safety outcomes were recorded including the presence of any parenchymal hematoma (ECASS III parenchymal hematoma type 1 or 2), subarachnoid hemorrhage (diffuse or focal within the territory of the artery treated for distal occlusion), and arterial spasm (defined as any degree of spasm in treated vessels).
Statistical analysis
Continuous variables are reported as mean±SD or median (IQR). Categorical variables are reported as proportions. For continuous variables, comparisons between groups were made using the Mann–Whitney U test. For categorical variables, between-group comparisons were made using either the χ2 test or Fisher’s exact test for variables with expected cell counts <5. Significance was set at p<0.05. Analyses were performed using STATA 14 (Stata Corp, College Station, Texas, USA).
Results
Baseline characteristics: BEMP cohort
Twenty-five vessels were treated in 22 patients. Median age was 67 (59–76) years, 16 (72%) were male, median National Institutes of Health Stroke Scale score was 17 (9–23), Alberta Stroke Program Early CT Score 8 (6–10), and last normal to puncture was 7 (3–11) hours. Intravenous alteplase was used in five (23%) patients and a balloon guide catheter in 20 (91%). Most patients had isolated distal occlusions (see online supplementary table 1). The occlusions predominantly involved the distal MCA (see online supplementary table 2) and the superior MCA division in half of the patients.
Supplemental material
In the BEMP cohort, mFPE was achieved in 20 (80%) and FPE in 15 (60%) vessels, while final mTICI 2b–3 was obtained in 21 (84%) and mTICI 3 in 16 (64%). The median number of passes was 1 (≥2 in two patients). Blind exchange was possible in all attempted cases. No parenchymal hemorrhages were noted, but three subarachnoid hemorrhages were identified. One patient was found to have subarachnoid hemorrhage/active extravasation after proximal artery treatment but before the distal occlusion approach. One was a focal subarachnoid hemorrhage (attributed to the distal occlusion treatment with no clinical impact), and another had diffuse subarachnoid hemorrhage (unclear if related to the proximal or distal occlusion treatment and leading to hydrocephalus). Ten out of 19 patients (40%) achieved a modified Rankin Scale score of 0–2 at 90 days.
BEMP versus standard techniques
The comparison between BEMP (n=25 vessels) and standard techniques (n=144 vessels treated with 3 mm Trevo (n=92) or 3MAX (n=52)) showed comparable baseline characteristics (see online supplementary table 1). BEMP was performed increasingly in distal MCA occlusions (M3 occlusions 52% vs 22%; p=0.001) (see online supplementary table 2). Vessel location and luminal diameter were otherwise comparable. There was a higher rate of mFPE (80% vs 56%; p=0.03) and a trend towards a higher probability of FPE (60% vs 40%; p=0.07) with BEMP compared with standard techniques (see online supplementary table 3). Final reperfusion rates and clinical outcomes were comparable.
Discussion
We describe a novel combined stent-retriever/aspiration catheter technique (BEMP) which appears to be helpful in optimizing the procedural performance in the treatment of distal arterial occlusions.
Considering that the 3MAX is longer than the Trevo 14 microcatheter (160 cm vs 157 cm), they cannot be navigated in a coaxial manner. The blind exchange derived from the need to circumvent this limitation. The stiffness of the retriever delivery wire, the distal anchoring by the deployed stent-retriever, and the coverage of the wire by the the balloon guide catheter eliminate the risk of pushing/losing the delivery wire into the patient. The subsequent straightening of the vessels that can be achieved by a gentle pull of the retriever wire that can greatly facilitate overcoming barriers to the distal navigation of the aspiration catheters.
The pinning maneuver has been described in proximal occlusions.9 The concept is to deploy the retriever and advance the aspiration catheter until it engages the clot. Relatively similar techniques have been described, mostly consisting of single-arm experiences10–13 and some comparative studies14–16 showing that it may be superior to either retriever or aspiration thrombectomy alone. The fundamental aim is to push the aspiration catheter slightly past the proximal end of the clot in order to ‘cork’ (partially ingest) the thrombus into the catheter. This increases the retrieval force by combining the traction from the retriever and the aspiration, which possibly explains the higher rates of mFPE and the trend towards increased FPE in our series. Moreover, the friction for retrieval is attenuated since less retriever is exposed, consequently decreasing stretching and torsion in tortuous and small distal vessels.17 Finally, by adding the distal support in the vicinity of the clot, the vector of force is optimized as it gets closer to the angle of movement. The frequency of hemorrhagic complications was not statistically different between the methods and only one subarachnoid hemorrhage could directly be attributed to BEMP in the present study. The effect of the clot composition on the performance of the different techniques is not well defined but appears to play an integral role in procedural performance.18 19 We successfully applied the pinning technique in a miniature version using a small retriever/aspiration combination, which appears to promote the same benefits as seen when used with larger devices.
This study has the limitations inherent to retrospective analyses. The restricted sample of the BEMP cohort is a shortcoming. The lack of core laboratory imaging adjudication and the uncertainties related to the accuracy of the determination of reperfusion rates in distal occlusions may constitute a significant weakness. Since no formal protocol for device selection was followed, unmeasured variables could have introduced bias. The costs related to the use of an additional device need to be carefully considered. However, the results are encouraging and further studies are justified.
Conclusion
The BEMP appears to be a safe and effective technique for the treatment of distal occlusions. Additional studies are warranted.
References
Footnotes
Contributors DCH: Study conception, design of the work, acquisition of data, interpretation of data, drafting of the manuscript. ARA-B: Data acquisition, critical revision of manuscript. BE: Data acquisition, critical revision of manuscript. KR: Statistical analysis, critical revision of manuscript. GMR: Data acquisition, critical revision of manuscript. MRF: Data acquisition, critical revision of manuscript. RN: Design of the work, acquisition of data, interpretation of data, critical revision of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ARA-B, BE, KR, GMR, MRF: none. DCH: Consultant for Stryker and Vesalio. RN: Principal Investigator, Stryker Neurovascular (DAWN trial, no compensation, Trevo‑2 trial), Cerenovus/Neuravi (ENDOLOW trial, no compensation); consultant to Stryker Neurovascular; steering committee member, Stryker Neurovascular (no compensation), Medtronic (SWIFT trial, SWIFT Prime trial, no compensation), Cerenovus/Neuravi (ARISE‑2 trial, no compensation); angiographic core lab, Medtronic (STAR trial); executive committee member, Penumbra (no compensation); physician advisory board, Cerenovus/Neuravi, Phenox, Anaconda, Genentech, Biogen, Prolong Pharmaceuticals, Allm Inc (no compensation), Viz-AI; stock options, Viz-AI.
Ethics approval Emory University IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The unpublished data from this dataset are held by Grady Memorial Hospital/Emory University and DCH/RN. Requests for data sharing would be required to be discussed with them directly.
Patient consent for publication Not required.