Article Text

Abstract
Background Endovascular therapy (EVT) for stroke improves outcomes but is time sensitive.
Objective To compare times to treatment and outcomes between patients taken to the closest primary stroke center (PSC) with those triaged in the field to a more distant comprehensive stroke center (CSC).
Methods During the study, a portion of our region allowed field triage of patients who met severity criteria to a more distant CSC than the closest PSC. The remaining patients were transported to the closest PSC. We compared times to treatment and clinical outcomes between those two groups. Additionally, we performed a matched-pairs analysis of patients from both groups on stroke severity and distance to CSC.
Results Over 2 years, 232 patients met inclusion criteria and were closest from the field to a PSC; 144 were taken to the closest PSC and 88 to the more distant CSC. The median additional transport time to the CSC was 7 min. Times from scene departure to alteplase and arterial puncture were faster in the direct group (50 vs 62 min; 93 vs 152 min; p<0.001 for both). Among patients who were independent before the stroke, the OR for less disability in the direct group was 1.47 (95% CI 1.13 to 1.93, p=0.003), and 2.06 (95% CI 1.10 to 3.89, p=0.01) for the matched pairs.
Conclusions In a densely populated setting, for patients with stroke who are EVT candidates and closest to a PSC from the field, triage to a slightly more distant CSC is associated with faster time to EVT, no delay to alteplase, and less disability at 90 days.
- stroke
- thrombectomy
Statistics from Altmetric.com
Introduction
Endovascular therapy (EVT) improves outcomes for patients with emergent large vessel occlusion (ELVO) in the anterior circulation, up to 24 hours from symptom onset.1–8 The benefit of EVT diminishes rapidly, such that for every 4 min delay to substantial reperfusion, one additional patient out of 100 is more disabled.9 However, EVT requires specialized teams and resources not available at all hospitals. As a result, patients who are first taken by emergency medical services (EMS) to the closest primary stroke center (PSC) without EVT capability are typically transferred to a more distant comprehensive stroke center (CSC) if deemed EVT eligible.
These transfers may delay time to treatment and are associated with worse outcomes than with direct presentation to CSCs.10–12 Similar to protocols for trauma and ST segment elevation myocardial infarction, direct field triage by EMS to a more distant CSC based on clinical suspicion of ELVO has been proposed as a solution for reducing time to EVT, although potentially at the expense of delaying time to intravenous thrombolysis.13 Mathematical models have suggested that direct field triage may improve outcomes.14–16
Our region has a population of nearly 1.5 million people in Rhode Island and southeastern Massachusetts, and all 16 PSCs in our region use a standardized protocol to transfer patients to the single CSC where all EVT is performed. During the study period, a portion of our region implemented a severity-based, field triage algorithm, directing EMS to bypass closer PSCs and take patients directly to the CSC if they met field severity criteria.17 18 The purpose of this study was to compare the times to treatment and outcomes of patients with ELVO who went to the closest PSC versus those who were taken directly to the more distant CSC. We hypothesized that patients brought directly to the CSC would be treated faster and have less disability at 90 days.
Methods
Patient identification
We obtained institutional review board approval to query our prospectively collected database for consecutive patients who met the following criteria (see figure 1):
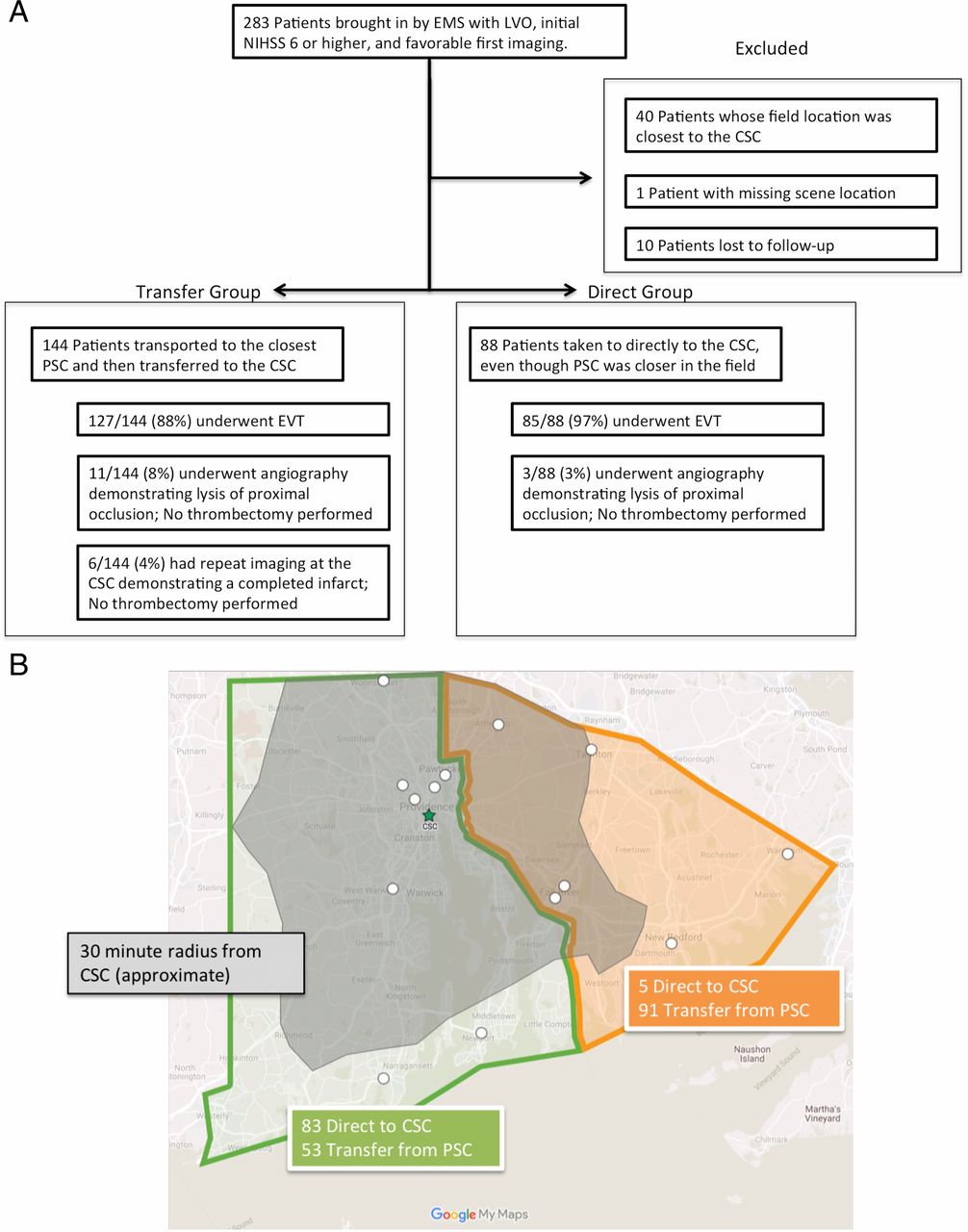
(A) Schematic distribution of the patients in both groups and their treatment. For completeness, patients excluded are also listed. (B) Geographic distribution of patients. The green area represents the region where field triage was mandatory as of March 1, 2017. The orange area represents the region where there is no severity-based triage. The shaded grey area indicates an approximate 30 min transfer time to the CSC. The green star is the CSC, and the white circles indicate PSCs. All patients were closest in the field to a PSC. CSC, comprehensive stroke center; EMS, emergency medical services; EVT, endovascular therapy; LVO, large vessel occlusion; NIHSS, National Institutes of Health Stroke Scale; PSC, primary stroke center.
Brought in via EMS between January 1, 2016 and December 31, 2017.
A new, disabling neurologic deficit (with a score of ≥6 on the National Institutes of Health Stroke Scale (NIHSS)), less than 24 hours’ duration.
Initial non-contrast computed tomography demonstrating lack of large completed infarction (ie, a score of ≥6 on the Alberta Stroke Programme Early CT score (ASPECTS)).
Occlusion of the intracranial internal carotid artery, M1 or proximal M2 segments of the middle cerebral artery on CT angiography (CTA).
The closest hospital from the scene was a PSC.
Clinical follow-up at 90 days available.
EMS protocols and scene geographic information
During the study period, the EMS protocols in Rhode Island, a portion of our catchment area, were updated to a severity-based, field triage model.17 18 Patients were to be taken directly to the CSC if they had a field Los Angeles Motor Scale19 score of ≥4, were within 24 hours from last known well, and within 30 min of the CSC. Compliance was optional before March 1, 2017 and required after that date. In adjacent Massachusetts, EMS protocols directed patients to be taken to the closest stroke center regardless of severity. For every patient, we calculated driving distance and time from the scene to the closest PSC, and to CSC (see online supplementary data). Patients were divided into direct and transfer groups based on actual transport destination. For both, we included all patients who were EVT eligible based on initial imaging. Treatments and geographic distribution of the two groups are shown in figure 1.
Supplemental material
Study treatment and intervention
Patients were divided based on transport destination, with the direct group those which went to the CSC, bypassing a closer PSC and the transfer group those taken to the closest PSC. We included all patients who were EVT eligible based on initial imaging, regardless of whether they received EVT or not. The details of our EMS education program18 and PSC transfer protocol20 have been previously published. More information, including times from scene departure to hospital arrival, is shown in the online supplementary data. Additionally, details of why patients were transported to the PSC in the transfer group are shown in online supplementary table 1.
Matched-pairs modeling
Given that some patients in the transfer group might be outside the 30 min radius from the CSC and understanding that stroke severity might affect triage, we developed a matched-pairs model, matching patients from the two groups according to time to CSC and NIHSS. For this model, we planned to look at the interaction between transport time to CSC and time to alteplase and arterial puncture. Details of the matching methodology are shown in the online supplementary data, and a total of 70 matched pairs (n=140) were identified.
Outcome measures
The primary workflow outcomes were times from EMS scene departure to intravenous alteplase and arterial puncture for EVT. The primary clinical outcome was the modified Rankin scale (mRS) score, a commonly used measure of global disability, at 90 (±15) days after the stroke. Since we included patients with pre-existing disability in this series, we specified a priori that we would examine the clinical outcomes for all patients as well as those who had a pre-stroke mRS score of 0 or 1. These measures were examined for all patients and the matched pairs.
Statistical analysis
All analyses were conducted using SAS Software 9.4 (SAS Inc, Cary, North Carolina, USA). Analyses of time to treatment were performed using Kaplan-Meier estimation with 95% confidence intervals; as there was no censoring, the Wilcoxon test was used to compare groups. For completeness and to provide estimates for meta-analyses, workflow was also modeled as a mean using the generalized linear model assuming a negative binomial distribution (online supplementary table 2). Other baseline characteristics were assessed using the Wilcoxon test, Χ2, or Fisher’s exact test, as appropriate.
The primary clinical outcome, 90-day mRS score, was modeled together with pre-stroke mRS score, for the direct and transfer groups using a generalized mixed model assuming a binomial distribution (0–6) with classic sandwich estimation and was examined as both a point estimate (mean) and a shift analysis, examining the odds of having a lower mRS score at 90 days. The assumption of proportional odds was evaluated using the Score Test. Similarly, a generalized mixed model assuming a negative binomial distribution was used to model the interaction between EMS time to CSC and scene departure to alteplase and arterial puncture between the direct and triage groups in the matched-pairs model. Testing of primary outcomes was conducted under a superiority framework. The value of α was established, a priori, at the 0.05 level and all interval estimates were calculated for 95% confidence. False discovery rate was controlled for primary outcomes using the Benjamini–Hochberg procedure, with a false discovery rate of 0. 05.
Results
Demographics and workflow parameters for the two groups are summarized in table 1. There were higher rates of hyperlipidemia in the transfer group (54% vs 39%, p=0.02). However, the remainder of the demographics failed to show significant differences between the two groups. The median time from field to the CSC was significantly shorter in the direct group, 18 versus 30 min (p<0.001) for the transfer group. This was expected, given that those patients who were more than 30 min from the CSC would, in most cases, be taken to the closest PSC. In the matched-pairs model, times to the CSC were not significantly different (online supplementary table 3). Although all patients were EVT eligible based on clinical and imaging characteristics at first presentation, there were 3/88 (3%) in the direct group and 17/144 (12%) in the transfer group who did not undergo EVT (figure 1). The reasons patients did not undergo EVT are summarized in figure 1. Among those who received alteplase, clot lysis obviating EVT was 3/48 (6%) in the direct group and 11/94 (12%) in the transfer group. Higher rates of clot lysis would be potentially expected in the transfer group owing to a greater time interval between alteplase and start of EVT. Additionally, 6/144 (4%) in the transfer group had prolonged interfacility transfer delays, with repeat imaging showing a completed infarct, and did not undergo EVT. These patients were included in the analysis of clinical outcomes. Procedural workflow characteristics, including location of intracranial occlusion, time to recanalization, and completeness of recanalization, were also similar.
Demographics, EMS scene parameters, and workflow times for all patients
Clinical and workflow outcomes
Direct and transfer groups
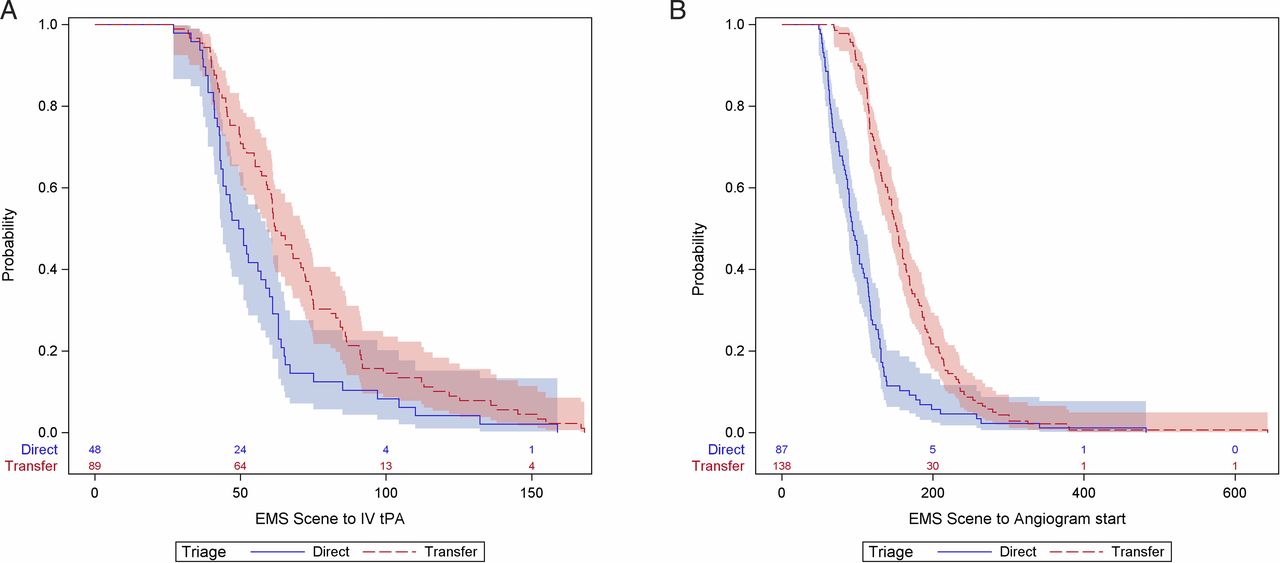
Despite a median of 7 additional minutes of transport time in the direct group, times from scene departure to alteplase and arterial puncture were significantly faster in the direct than in the transfer group (table 2). These workflow times are depicted in figure 2. The faster time to alteplase in the direct group was probably due to significantly faster alteplase administration at the CSC (median door to alteplase time of 33 compared with 53 min at PSCs, p<0.001).
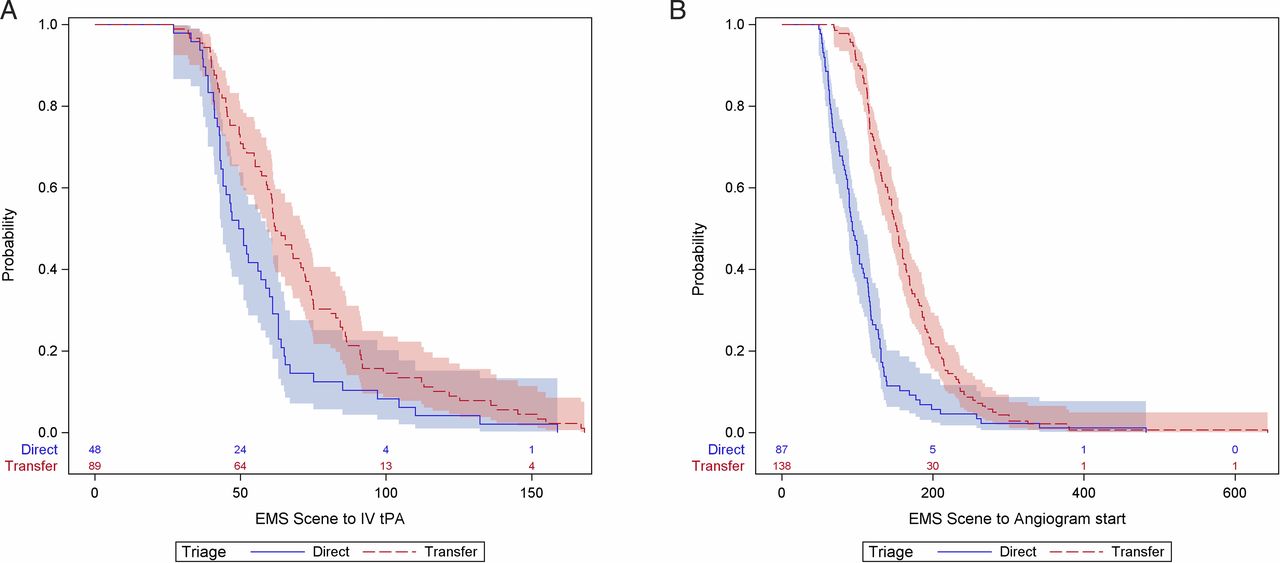
Time to treatment curves for all patients, depicting the time to treatment from EMS scene departure to intravenous alteplase (A) and arterial puncture (B). EMS, emergency medical services; tPA, tissue plasminogen activator.
Primary outcomes for all patients
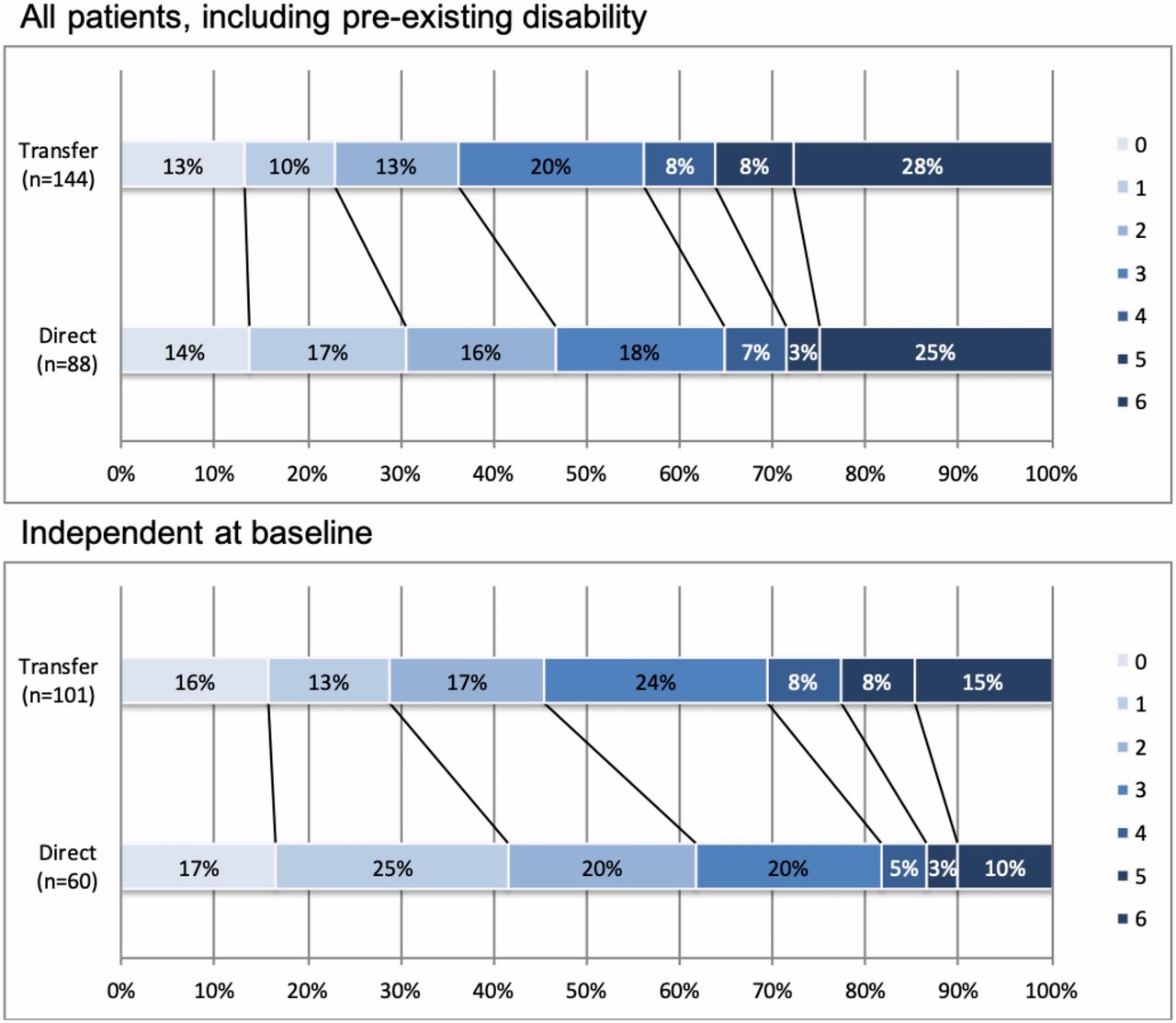
Direct transport to the CSC was associated with less disability at 90 days, for all patients including those with pre-existing disability (table 2). Among those patients who were independent before treatment, the OR for being less disabled at 90 days (a decrease of ≥1 point on the mRS) was 1.47 (95% CI 1.13 to 1.93, p=0.0049). Overall rates of functional independence at 90 days increased to 46% in the transfer group and 62% in the direct group (figure 3).

Distribution of modified Rankin scores at 90 days for all patients in the series, as well as those without pre-existing disability.
Rates of symptomatic intracranial hemorrhage (defined as a new parenchymal hematoma, extensive subarachnoid hemorrhage, or intraventricular hemorrhage on imaging with a concomitant four-point increase in NIHSS score) were 10/144 (7%) in the transfer group, and 1/88 (1%) in the direct group (p=0.06).
Ten patients were excluded owing to missing 90-day outcomes (seven in the transfer group, three in the direct group). To account for possible confounding due to missing data, we performed a sensitivity analysis on the primary workflow and clinical outcomes incorporating the 10 with missing outcomes. We assumed a worst-case scenario, in which all patients in the direct group were dead (mRS score 6) at 90 days, and all patients in the transfer group were at their pre-stroke mRS score at 90 days. The primary clinical and workflow outcomes are presented in online supplementary table 4. There remained significantly faster time to alteplase and EVT in the direct group. For patients without pre-existing disability, the OR for less disability in the direct group at 90 days in the sensitivity analysis was 1.4 (95% CI 1.0 to 1.8, p=0.013).
Matched pairs
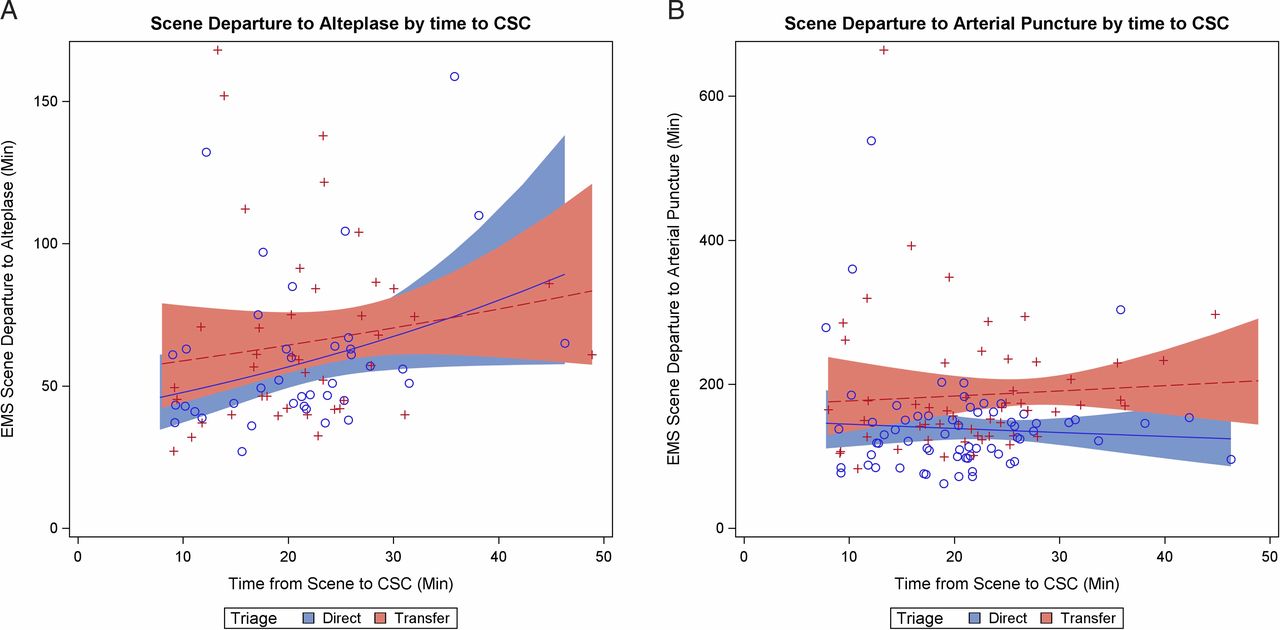
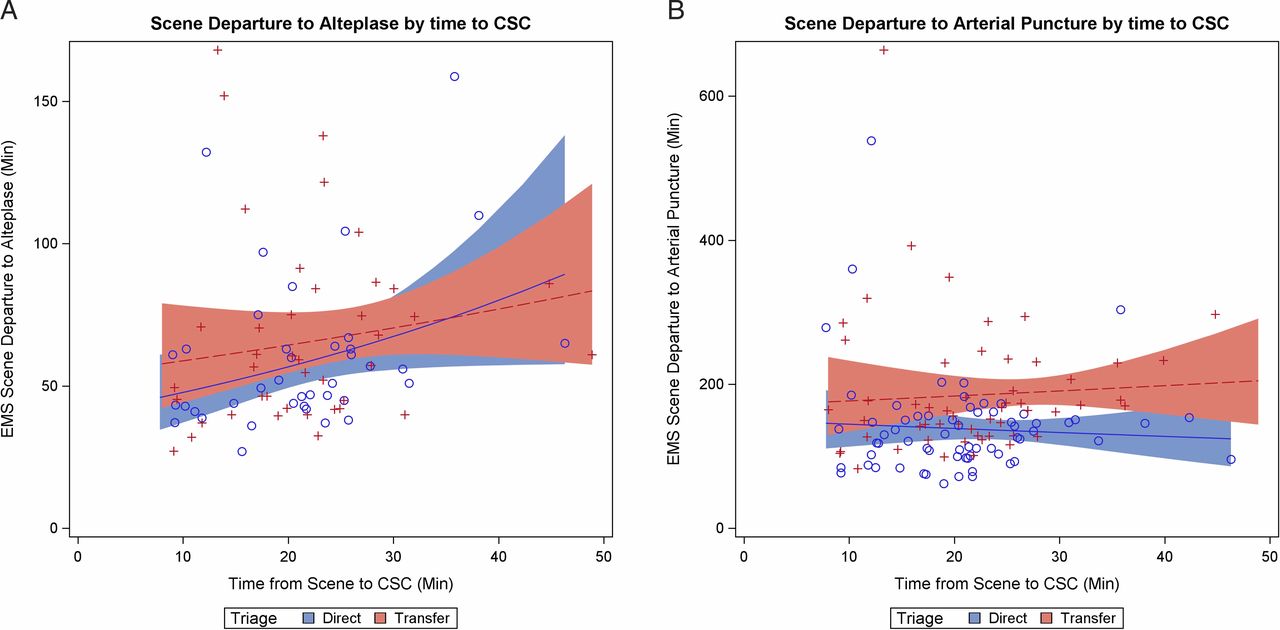
In the matched-pairs model (matched according to stroke severity and time to CSC), there was no evidence of a difference in time from field scene departure to alteplase, but the direct group had significantly faster time to arterial puncture (table 2). When examining the interaction between time to CSC and time to treatment in the matched pairs, there was no evidence of a difference in time to alteplase, but time to arterial puncture remained significantly faster in the direct group, even as time from the field to the CSC increased (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examining the interaction between time from scene to CSC and times to treatment for the matched pairs, examining scene departure to alteplase (A) and scene departure to arterial puncture (B) CSC, comprehensive stroke center; EMS, emergency medical services.
No statistically significant difference was seen in pre-stroke mRS score between direct and transfer groups (0.80 (0.53, 1.19) vs 0.83 (0.55, 1.20)), (OR=1.04 (95% CI 0.56 to 1.90), p=0.90). However, the direct group had a mean 90-day mRS score that was almost one point lower than that of the transfer group (online supplementary figure 1). The OR for being less disabled in the direct group was 1.9 (95% CI 1.03 to 3.31, p=0.02). When analysis was limited to only those patients in the matched pairs without pre-existing disability, mean 90-day mRS score was 1.7 (direct) versus 2.7 (transfer), an OR of 2.06 (95% CI 1.10 to 3.89, p=0.01) for less disability. Functional independence at 90 days increased from 42% in the transfer group to 68% in the direct group (online supplementary figure 2).
Discussion
For patients with anterior circulation ELVO, EMS triage past the closest PSC to a more distant CSC is associated with earlier EVT, better clinical outcomes, and no delay to treatment with intravenous alteplase. This benefit was observed for the entire cohort, and in a model matching pairs according to stroke severity and time to CSC. Faster treatment and better outcomes were seen in the direct group irrespective of time from scene to CSC. We believe these results will have significant implication for stroke systems of care, especially given that every minute reduction in time to EVT is estimated to save the healthcare system US$105921.
Our results align with models suggesting that where the CSC and PSC are in close proximity, direct transport to the CSC was likely to result in better outcomes.14–16 One previous clinical series specifically examining direct field triage to a more distant CSC in Denmark observed similar results, with increased independence at 90 days (62% vs 43%), and a 58 min reduction in time to EVT with direct transport.12 However, they had historical rather than contemporaneous groups as in our series, and their geographic situation is vastly different, with one PSC and one CSC, located 75 miles apart. In a recent report of a large registry, transferred patients had a significantly lower rate of functional independence at 90 days (52.2% vs 60.0%).11 That registry evaluated only patients who actually underwent EVT, whereas we also included patients who lysed with alteplase and those with infarct progression precluding EVT. As such, our series is likely more representative of a population of EVT-eligible patients.
It may be argued that these results are applicable only in our region. In the Greater Cincinnati region the median additional transport time to CSC was 8 min, and 85% were <15 min additional transport time to the CSC, both similar to our series.22 An analysis of prehospital data in the United States showed approximately 80% of EMS transport occur in urban regions, with a median scene to first hospital transport time of 12 min, similar to our patients.23 Within the United States, 56% of the population was within 60 min ground transport to a center providing EVT in 2011, and that number may be higher now.24 In the Systematic Evaluation of Patients Treated with Neurothrombectomy Devices for Acute Ischemic Stroke (STRATIS) Registry, with 985 patients across 55 sites in the United States, 65% of the patients incurred their stroke within 25 miles of the hospital where EVT was performed, and over 40% within 10 miles.25 It is likely that there are many other regions that are similar to ours.
Our protocol was developed based on an absolute transport time to the CSC of <30 min, in order to mimic protocols used for ST elevation myocardial infarction and trauma in our region. However, the optimal time parameters to determine triage to a more distant center are unknown. The American Heart Association has suggested a 15 min additional transport time threshold for patients with suspected ELVO in their most recent recommendations.26 A recent decision analysis suggested that both time to CSC and time from onset play a role in determining an optimal triage radius, and that for early presenting patients, the bypass threshold may increase up to 56 minutes.27 Our results would concur, as time from scene departure to recanalization was faster in the direct group irrespective of time to CSC, with no delay to alteplase (figure 4). It is possible that time from EMS scene departure to alteplase will increase with direct triage to CSCs with longer prehospital transport times than those represented in this population. Further research to determine the optimal threshold for triage to a more distant center is warranted.
For PSCs, door to needle (DTN) for intravenous alteplase and door in door out time (DIDO) are key performance metrics, with longer times associated with worse outcomes.28 It is worth noting that median DTN times in this series are not dissimilar from those of other series. In an analysis of DTN from nearly 1000 PSCs treating almost 500 000 patients in the United States, the median DTN was 71 min, as compared with 53 min in our series.29 Additionally, in the STRATIS registry the median DTN at PSCs was 56 min, compared with 36 min at CSCs, a similar difference to this series. As such, the DTN times in our series at PSCs are unfortunately probably representative of real-world performance at PSCs across the United States. The median DIDO at the PSCs would have to decrease from 85 to 26 min for the entire cohort and from 79 to 39 min in the matched-pairs model in order to equal the treatment times in the direct group. Improving workflow at PSCs will remain critical for all patients with a stroke, including those without ELVO, as well as patients with ELVO with milder deficits who do not meet triage criteria, those who are mis-triaged, and those who are beyond the triage radius.
Limitations
A drawback to this series is the lack of documented field severity score for all patients. As a point of reference, during the study period, a total of 1170 patients with a final diagnosis of acute ischemic stroke were brought by EMS directly to the CSC, and of these, 147 (12.6%) underwent thrombectomy. It is beyond the scope of this work to determine the accuracy of EMS assessment and rates of over- or under-triage. The vast majority of our patients had an admission NIHSS score of ≥10, and would probably have been appropriately classified using any of the common field severity scores.30 The assessment of the degree of over- and under-triage is an important area for future study, as over-triage might overwhelm CSC resources. Additional techniques for field triage, including mobile telemedicine consultation, ultrasound, or impedance based portable diagnostic tools, are promising and require further study.31 Mobile stroke treatment units, capable of scanning and administering alteplase in the field, would essentially bring a PSC to the patient, and are worthy of further study.32 Finally, the volume of patients with ELVO seen at our referring PSCs would seem insufficient to implement mobile interventional stroke teams, but that may be a valid solution in other regions.33 The lack of delay to alteplase would suggest that patients in our region without ELVO who were triaged past a closer PSC to the CSC would probably not have been delayed in receiving alteplase, which has been discussed as a potential drawback to triaging patients to distant centers. For this same reason, concerns about delays to potentially more effective thrombolytic agents (such as tenecteplase) are probably unfounded.13
This series has other limitations. This is a non-randomized series from a single geographic region. A randomized trial is currently ongoing in Spain (NCT02795962), but a similar trial in the United States may be logistically difficult given the fragmented nature of our healthcare system. As such, a contemporaneous population-based comparison of two different protocols within one geographic region may be the most reasonable alternative. Additionally, we feel that our matched-pairs design with mixed modeling of pre-stroke and 90-day mRS score, matching according to time to CSC and NIHSS score, provides a strong alterative to randomization for these observational data. We have substantially improved EMS knowledge of our severity-based field triage protocol, optimized PSC and CSC workflow through an extensive quality improvement process, standardized imaging and procedural technique, avoiding general anesthesia, and transporting most transfer patients directly to the angiography suite without repeat imaging.18 20 28 34 35 Our results should be interpreted with caution in regions where the distribution and workflow metrics of stroke centers are not similar. Prehospital triage may be the last remaining, yet modifiable, bottleneck within an otherwise optimized stroke system of care.36
Conclusions
For patients with ELVO who are EVT candidates, triage based on EMS field severity assessment to a more distant CSC rather than a closer PSC was associated with significantly shorter time to EVT, better clinical outcomes, and no delay to alteplase. This association held true for our entire cohort and for a matched-pairs model. Seven additional minutes of prehospital transport was associated with nearly an hour faster time to EVT, and a 16–26% absolute increase in functional independence.
Acknowledgments
We acknowledge the EMS professionals, who have worked diligently to implement severity-based triage in our region.
References
Footnotes
Contributors All authors: substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Approved by the Lifespan institutional review board as a retrospective review of prospectively collected stroke center quality database, with waiver of informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.